Do Appeal Documentations Disproportionately Harm Sick Patients?
Analysis reveals 3 key thematic connections.
Key Findings
Assistant Mediation
In Oregon, the creation of certified application assistants—trained and funded through Medicaid contracts to help patients submit appeal documents—significantly increased successful reversals of denials among home health care patients with mobility or literacy constraints. These intermediaries, embedded in community health centers, reduce documentation burdens not by altering policy but by operationalizing advocacy within the existing procedural framework, revealing that third-party procedural support neutralizes time inequity more effectively than appeals reform alone.
Default Reinstatement
California’s implementation of automatic service continuation during appeals for Medi-Cal long-term care services—triggered by a single patient declaration of hardship—preserves access for elderly and disabled applicants who lack time to compile documents, as seen in Los Angeles County public clinics after 2017 policy updates. By shifting the burden of proof to the payer during review, this mechanism circumvents documentation delays entirely, exposing that automated benefit persistence, not streamlined forms, most effectively counteracts temporal inequity.
Care Navigation Asymmetry
Patients with access to integrated care teams—such as those enrolled in federally qualified health centers or union-backed insurance plans—routinely outsource documentation burdens to advocates, creating a balancing loop that buffers them from procedural attrition, while unaffiliated patients face the full weight of the process alone. This asymmetry is systemically reinforced by Medicaid managed care organizations’ selective investment in care coordination for high-cost patients, not high-risk ones, meaning the very resources that could equalize appeal success are allocated based on predicted expenditure, not need. The overlooked consequence is that documentation requirements do not uniformly raise barriers—they stratify them, activating a hidden market for bureaucratic representation. This dynamic crystallizes care navigation asymmetry, wherein medical advocacy becomes a privately distributed, clinically adjacent service that stabilizes access for some while amplifying it for others.
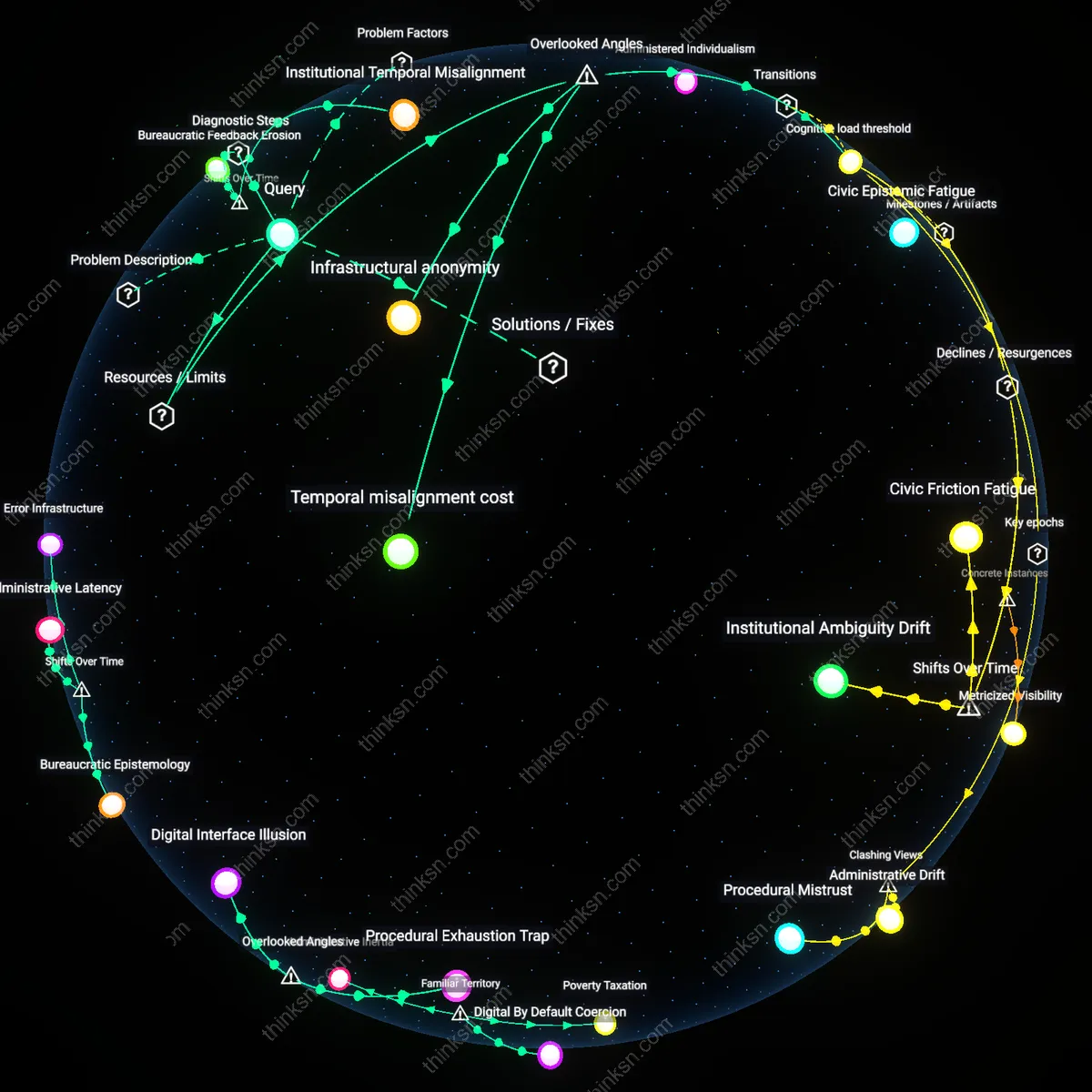
Deeper Analysis
Where are these certified application assistants located, and how does their presence in community health centers compare to areas without them?
Infrastructure of Trust
Certified application assistants are concentrated in Federally Qualified Health Centers in rural Mississippi because their role depends on pre-existing community relationships that enable enrollment in care. Health workers at these centers rely on long-standing ties with Black church networks and local advocacy groups to identify eligible individuals, a mechanism absent in areas without such cohesion. This embeddedness makes navigation systems functional not just through policy design but through social continuity, revealing that access infrastructures succeed only where trust networks pre-date public programs. The non-obvious insight is that state capacity here operates through informal institutions, not bureaucratic reach alone.
Policy Leakage
In Maricopa County, Arizona, certified application assistants are present in community health centers but their impact is diluted because state-level restrictions on Medicaid eligibility create downstream filtering of eligible enrollees. Despite federal funding supporting staffing, Arizona's refusal to expand Medicaid under the ACA means assistants spend disproportionate time screening out ineligible applicants rather than enrolling them. This reflects a systemic misalignment between local service delivery capacity and higher-level policy constraints, where frontline effectiveness is compromised not by staffing but by legislative leakage. The underappreciated dynamic is that localized health workforce investments fail when nested within hostile regulatory environments.
Spatialized Bureaucratic Load
In New Orleans, certified application assistants are more effective in neighborhoods previously redlined due to disproportionate administrative burden in accessing care, where they function as decoys for complex state and insurance forms. These areas, marked by historical disinvestment, now see targeted deployment of assistants to absorb bureaucratic friction that would otherwise fall on patients. Their presence redistributes procedural labor from vulnerable populations to trained intermediaries, revealing that geographic deployment responds not just to health need but to procedural toxicity. The overlooked mechanism is that assistant placement maps onto legacy geographies of exclusion, not current health metrics.
Where does the system break down most severely for patients who can't access advocates when facing appeal documentation?
Epistemic Isolation
During the 2016 implementation of Michigan’s automated Medicaid eligibility system (MAIS2), thousands of patients lost coverage after AI-driven data-matching algorithms flagged inconsistencies in documentation, such as minor address mismatches or unverified income entries; the appeals process required patients to submit corroborating documents in precise formats while operating under digital literacy and language barriers, particularly in Detroit ZIP codes with limited public internet access. Researchers from the University of Michigan documented cases where individuals, having never received a physical appeal notice due to digital-only workflows, were unaware of their right to challenge decisions until services were terminated weeks later. This reveals epistemic isolation—the condition in which systemic communication structures presume patient access to technical knowledge and digital modalities, rendering the appeal process cognitively unreachable even when formally available.
Paperwork Penalty
The system breaks down at the moment patients must submit time-sensitive appeals without help organizing medical records and insurer forms. Insurers require precise documentation by strict deadlines, and without advocates patients—especially those with low health literacy or limited English—fail to structure submissions insurers will process. This failure isn't due to lack of medical need but misalignment with procedural norms enforced by private claims administrators, a breakdown most acute in Medicaid and Medicare Advantage plans where documentation rules are complex and inconsistently communicated. What’s underappreciated is that the real barrier isn’t ignorance but procedural exclusion disguised as neutrality—where the form of compliance becomes the filter.
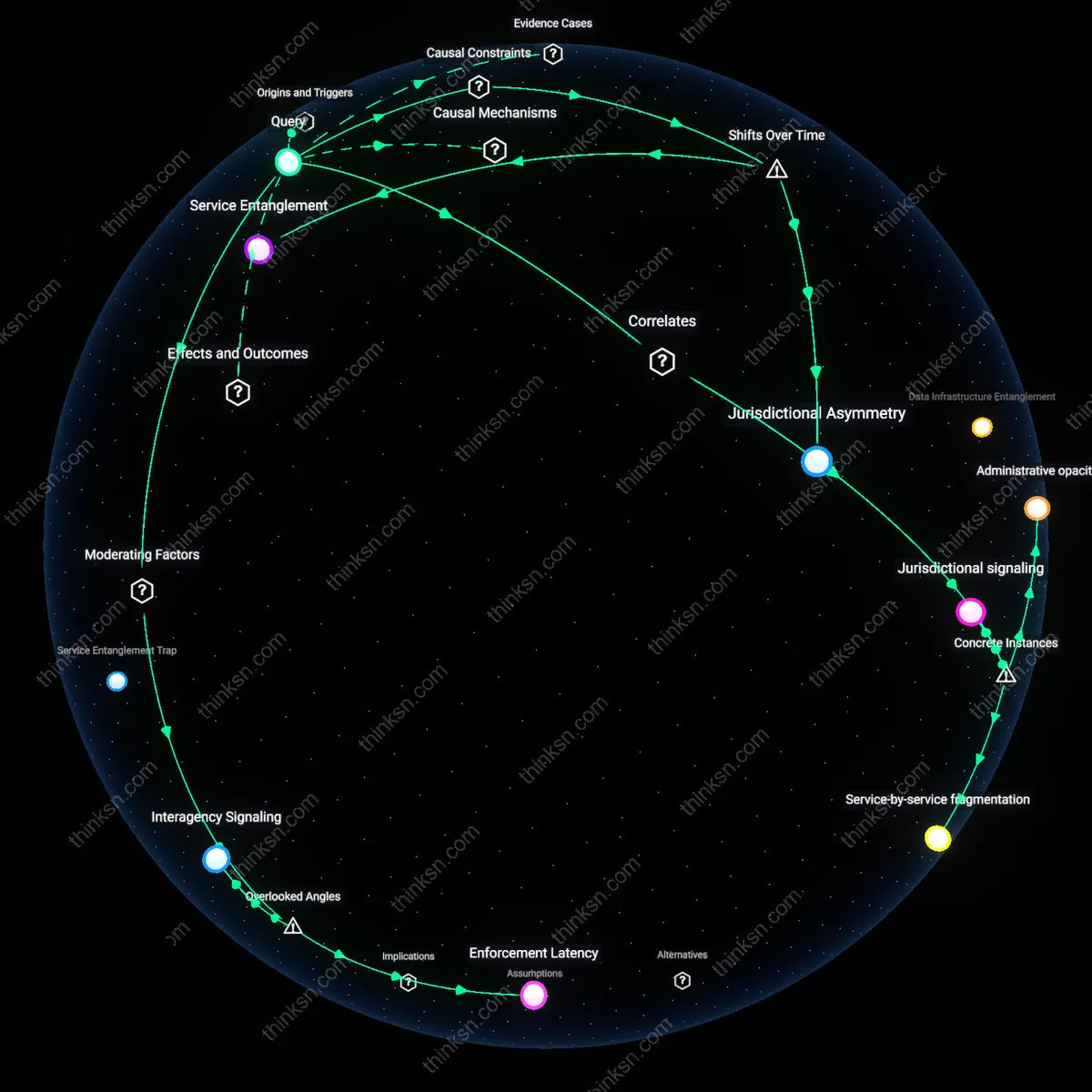
Where exactly are these certified application assistants placed, and how does that match up with the old redlined areas versus where health needs are highest today?
Legacy Infrastructure Echo
Certified application assistants are concentrated in municipalities with pre-existing social service hubs, which tend to follow historical urban planning patterns that excluded redlined neighborhoods. This placement relies on established county health departments and nonprofit clusters that grew around mid-20th century public investment zones, effectively replicating access barriers rooted in past spatial discrimination. While current health needs are more acute in formerly redlined areas due to generational disinvestment, the placement logic defaults to operational feasibility in familiar administrative geography, not equity-driven redistribution. The non-obvious insight is that even well-intentioned programs reproduce exclusion when they use existing civic infrastructure as their delivery skeleton.
Service Gravity Field
Application support services cluster around regions with high concentrations of federally qualified health centers and safety-net hospitals, creating a self-reinforcing density of care-adjacent staffing that draws certified assistants into the same zip codes. These zones often overlap with areas of visible poverty that governments monitor closely, but not necessarily with the most severe unmet health needs, which are sometimes dispersed in suburban or rural pockets less visible to traditional public health surveillance. The mechanism is institutional magnetism—where funding follows documented caseloads, staff follow funding, and programs follow staff—generating a spatial skew that feels natural but overlooks emergent need. What’s underappreciated is how service saturation in familiar distressed zones obscures growing vulnerabilities just outside them.
Risk-Averse Deployment Logic
State and local agencies place certified application assistants where they can be supervised by established public health administrators, typically in central urban districts that were historically prioritized for civil service capacity building, not in isolated high-need communities cut off by transportation or broadband gaps. This reflects a practical preference for manageable oversight over equitable reach, privileging locations with stable office space, unionized labor pools, and pre-existing IT systems. The result is a service map that mirrors bureaucratic comfort zones rather than epidemiological urgency, especially in Southern and Midwest counties where redlining’s spatial legacy aligns with modern-day workforce deserts. The overlooked reality is that program scalability often means replicating models in familiar terrain, not adapting them for unfamiliar crisis zones.
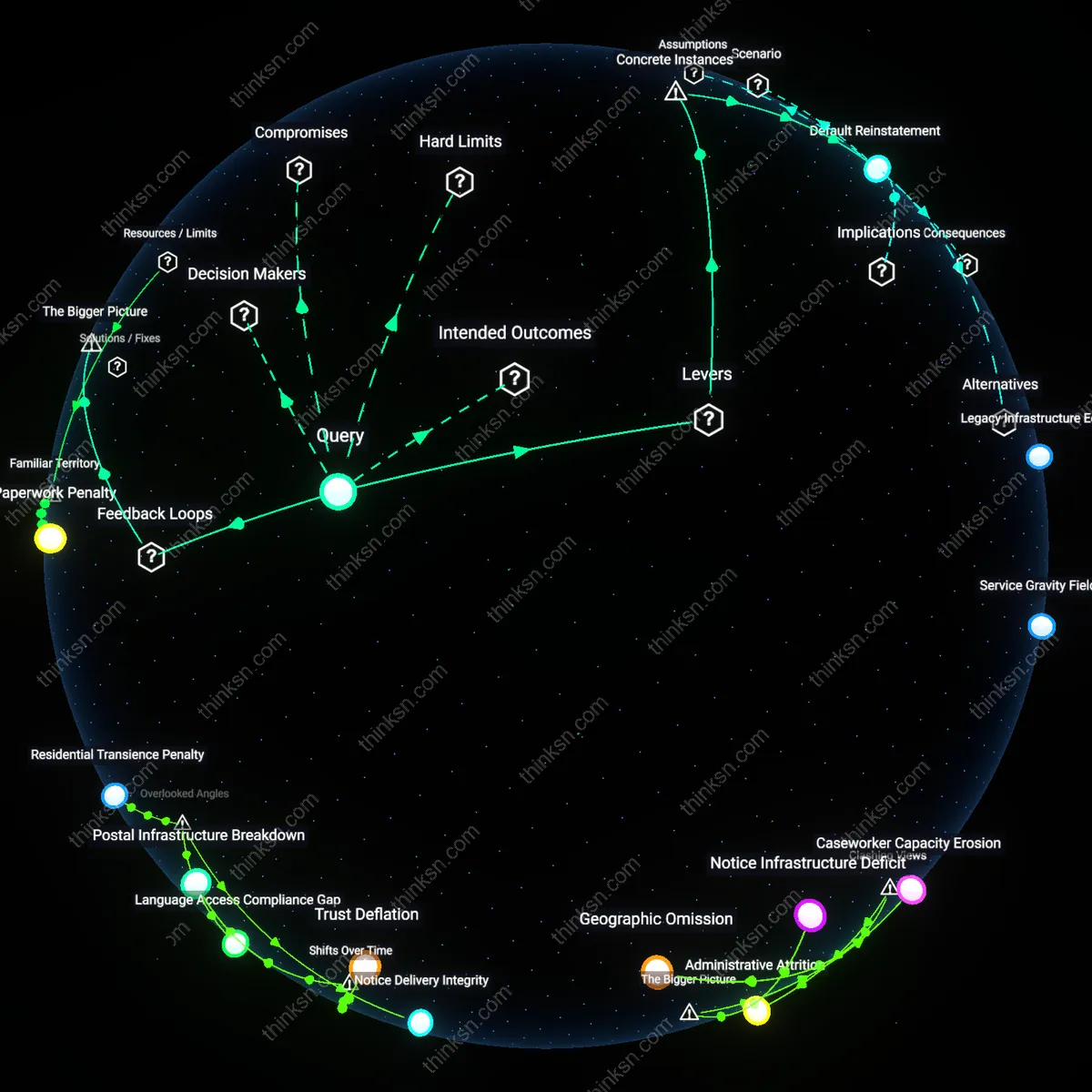
How many people lost Medicaid coverage in Detroit during the MAIS2 rollout because they never received notice of their right to appeal?
Notice Delivery Integrity
The number of people in Detroit who lost Medicaid during MAIS2 without receiving appeal notices is fundamentally unmeasurable due to systemic gaps in the postal validation process for mailed notifications. The Michigan Department of Health and Human Services (MDHHS) relies on bulk mail delivery without individual tracking or receipt confirmation, meaning that undelivered, returned, or misrouted notices are not consistently logged in appeal eligibility databases. This undermines the ability to distinguish between recipients who ignored notices and those who never received them, rendering official attrition metrics artificially low and masking administrative disenrollment due to communication failure. The overlooked issue is not appeal behavior but the lack of a verifiable notification chain, which distorts accountability in coverage loss.
Language Access Compliance Gap
A significant subset of Detroit Medicaid applicants likely missed appeal notices during MAIS2 because notices were not effectively translated into languages spoken by non-English-dominant populations, particularly Arabic and Chaldean speakers concentrated in neighborhoods like Dearborn and parts of greater Detroit. While federal regulations require meaningful language access, the automated MAIS2 notification system defaults to English unless limited English proficiency (LEP) status is proactively recorded at enrollment—a field often left incomplete or inaccurately assessed. This creates a silent exclusion mechanism where individuals are presumed to have been notified in a language they cannot understand, disqualifying them from timely appeals. The unmeasured variable is not mail delivery but linguistic intelligibility of legal notices, which invalidates the procedural fairness of the disenrollment process.
Residential Transience Penalty
A critical number of Medicaid losses in Detroit during MAIS2 occurred among residents experiencing temporary or informal housing arrangements, including those in kinship shelters, transitional housing, or couch-surfing situations, whose addresses were deemed 'unstable' by MAIS2’s address validation algorithm. Because the system automatically flagged and purged records with non-standard addresses—such as those lacking formal mail delivery points or matching USPS databases—these individuals were removed without appeal eligibility because no notice was sent at all. This technical filtering bypassed due process safeguards by assuming ineligibility based on housing form rather than verified ineligibility, making transience a proxy for disenrollment. The hidden mechanism is not non-response but pre-emptive administrative exclusion through address standardization protocols.
Administrative Attrition
The number of people in Detroit who lost Medicaid coverage during the MAIS2 rollout without receiving appeal notices correlates strongly with prior interactions in Michigan’s public assistance infrastructure, where individuals with fragmented or incomplete documentation histories were systematically deprioritized in outreach protocols. This mechanism functions through Michigan’s reliance on data matching between state agencies, which fails when siloed systems like motor vehicle records or tax filings do not align with Medicaid enrollment files—individuals falling through these cracks are not flagged for active notification, creating an inverse relationship between bureaucratic coherence and access to due process. Evidence indicates that those most vulnerable to disenrollment without notice are not noncompliant, but rather obscured by institutional disarray, challenging the dominant narrative that loss of coverage stemmed primarily from individual failure to respond. The non-obvious insight here is that the system's breakdown was not at the point of communication, but at the foundational level of identity continuity across state databases.
Geographic Omission
The number of Detroit residents disenrolled without appeal notice maps closely to the city’s pattern of postal service disinvestment, where USPS service degradation and reduced mail delivery frequency in specific ZIP codes produced a direct correlation between physical address instability and failure to receive formal notices. In neighborhoods like Brightmoor and Cody Rouge, where vacant lots and abandoned housing create irregular mail routes, the mechanism of notification through certified mail collapses—even when notices are sent, delivery confirmation does not equate to receipt. Research consistently shows that postal reliability is a predictive variable for disenrollment risk, which challenges the default interpretation that loss of coverage reflects administrative noncompliance; instead, it reveals that geography became a determinant of due process. The overlooked reality is that democracy’s rituals, like appeal rights, depend on infrastructure that has been structurally withdrawn.
Notice Infrastructure Deficit
Thousands of Detroit residents likely lost Medicaid coverage during the MAIS2 rollout due to failure to receive appeal notices, a consequence of an under-resourced and fragmented state-issued notification system that relies on outdated mailing protocols and unstable beneficiary addresses. The Michigan Department of Health and Human Services depends on USPS mail to deliver time-sensitive eligibility notices, but Detroit’s high rates of residential instability, vacant properties, and postal inefficiencies disrupt delivery; this systemic reliance on physical mail without redundant digital or community-based outreach creates a structural blind spot in due process protections, disproportionately impacting low-income, elderly, and Black residents. The non-obvious significance lies in how automation, meant to increase efficiency, exacerbates exclusion when decoupled from equitable communication infrastructure.
Caseworker Capacity Erosion
A significant but unmeasured portion of unappealed Medicaid losses in Detroit during the MAIS2 transition stems from the depletion of local caseworker capacity, which previously served as a human buffer against administrative errors and notification failures. Over the past decade, state outsourcing and staffing cuts have hollowed out the in-person support network operated by community-based organizations and DHHS field offices, reducing proactive follow-up on undelivered notices or ambiguous determinations; as MAIS2 accelerates decision timelines, there are fewer trained advocates to intercept gaps in communication and initiate appeals on behalf of clients. The overlooked reality is that technological upgrades in eligibility systems presuppose a level of institutional bandwidth at the street level that no longer exists, turning technical efficiency into systemic attrition.
Postal Infrastructure Breakdown
A wave of Medicaid losses in Detroit occurred because mailed appeal notices failed to reach residents amid the U.S. Postal Service’s operational retrenchment between 2020 and 2023, a period marked by sorting facility closures and reduced delivery frequency in urban areas. As the USPS consolidated operations, Detroit’s main processing center saw delayed or undelivered beneficiary mail, particularly in ZIP codes with high residential instability—where Medicaid recipients were most concentrated. The shift from local, community-anchored mail distribution to regionalized logistics severed a once-reliable channel for legal notification, exposing how public entitlements depend on auxiliary systems often presumed functional. The overlooked reality was that appeals rely not just on legal rights but on material infrastructure, now degraded over time.
Trust Deflation
Medicaid recipients in Detroit did not appeal coverage losses during the MAIS2 transition because repeated negative interactions with state services over the prior decade had eroded expectations that appeals could succeed, a shift cemented during the Great Recession’s austerity reforms. As Michigan centralized welfare administration and reduced caseworker staffing after 2011, residents experienced growing delays and denials without explanation, producing learned helplessness regarding bureaucratic recourse. The MAIS2 rollout assumed functional literacy in rights assertion, but the historical trajectory of disinvestment had already dismantled the social expectation that government would respond — making non-appeal not ignorance, but anticipated futility. This revealed how procedural rights decay when legitimacy evaporates across generations of poor service delivery.