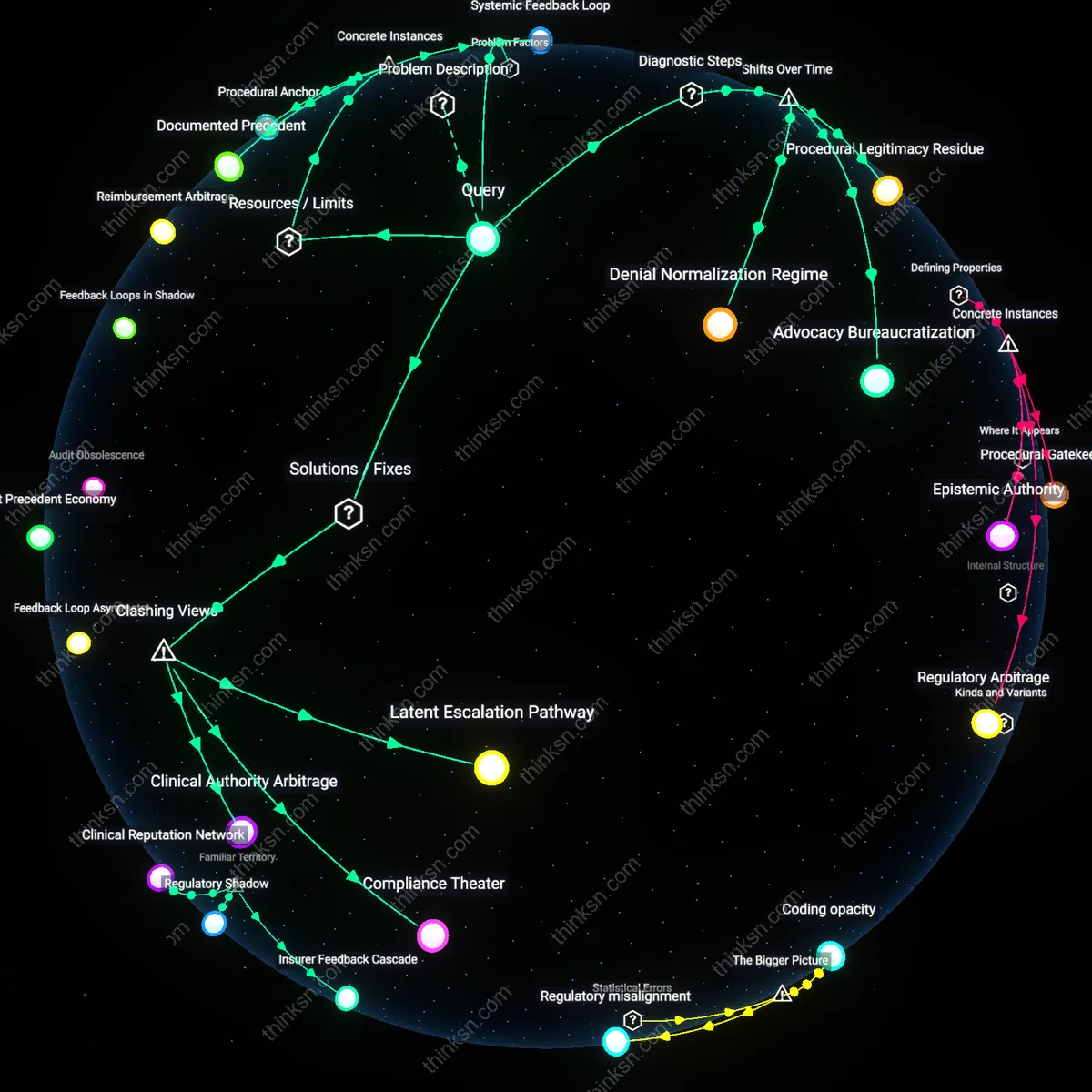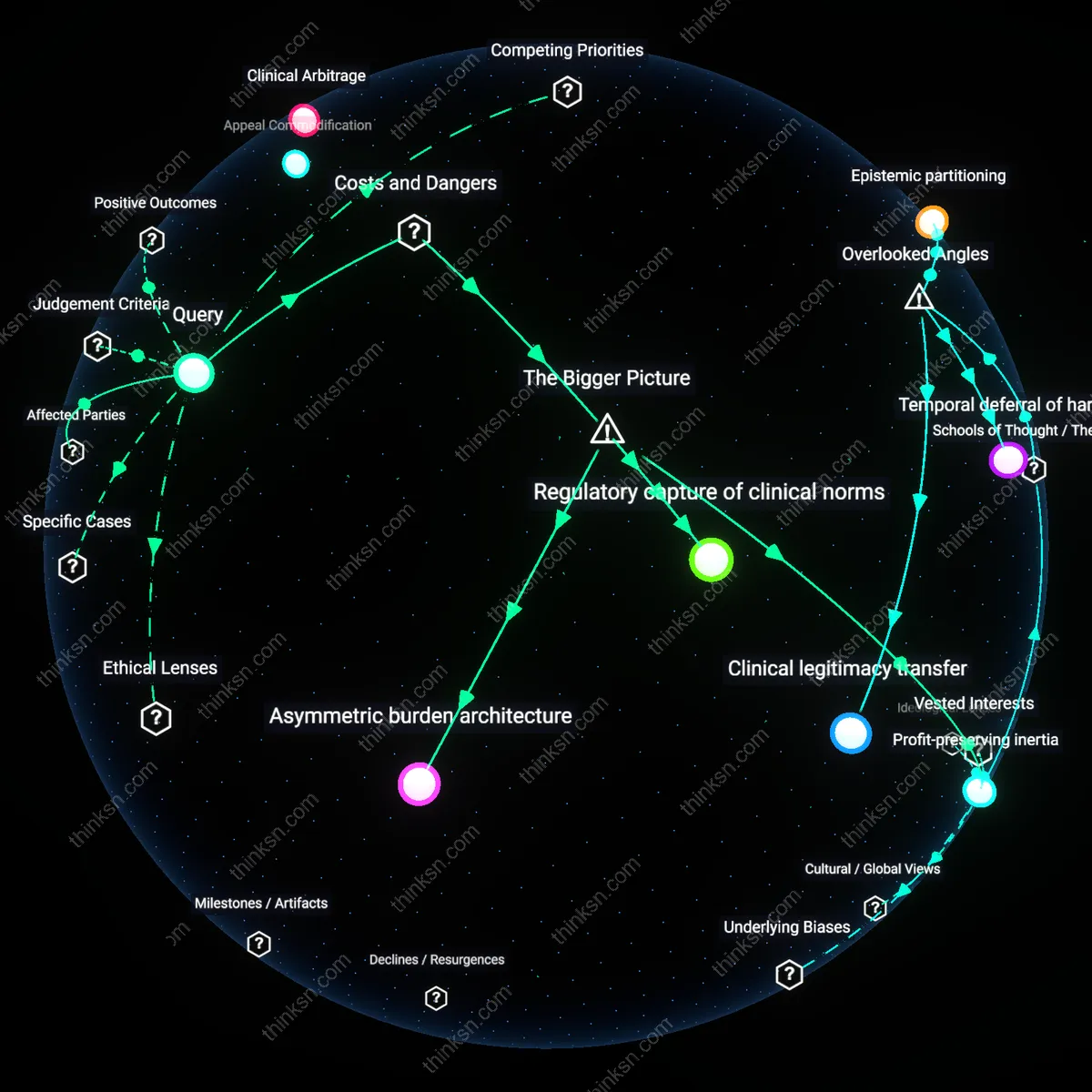
Why Does Prior Authorization Drag On Despite Streamlining Tech?
Analysis reveals 9 key thematic connections.
Key Findings
Institutional Inertia
The administrative burden of prior authorization persists because payer-side risk management infrastructures, developed during the managed care expansion of the 1990s, institutionalized manual review as a cost-containment norm, embedding it into legacy claims-processing systems that resist interoperable automation despite the availability of real-time decisioning tools. This persistence is not due to technological absence but to the path-dependent consolidation of utilization review as a core actuarial function—where insurers retained control over clinical adjudication rhythms even as electronic data interchange matured, ensuring that any shift toward automation would require overhauling entrenched risk-assessment workflows. The non-obvious consequence of this historical entrenchment is that streamlining efforts are systematically undermined not by payer malice but by organizational memory that treats delays as necessary friction, revealing how 1990s-era skepticism toward physician autonomy still governs 21st-century digital architectures.
Regulatory Arbitrage
Prior authorization endures because the post-D Affordable Care Act pivot toward evidence-based coverage created a loophole where payers could justify administrative stringency as clinical rigor, transforming what was originally a utilization gatekeeping tool into a legally defensible risk stratification mechanism that shields insurers from litigation and regulatory penalties. As CMS shifted from volume- to value-based benchmarks in the 2010s, the precision of medical necessity criteria increased, but so did the incentive to offload decision-making latency onto providers—making authorization delays a de facto compliance shield rather than mere inefficiency. The underappreciated outcome is that the burden functions not as a flaw but as a calculated temporal buffer, enabling payers to align with evolving regulations while avoiding liability for adverse outcomes tied to delayed care, thereby institutionalizing friction as a compliance asset.
Asymmetric Data Leverage
The persistence of prior authorization stems from a reversal in data power dynamics after the 2009 HITECH Act incentivized EHR adoption, where payers gained unprecedented access to longitudinal claims and clinical datasets while providers became dependent on opaque authorization APIs with limited reciprocity, shifting the balance toward payer-controlled decision lags that extract behavioral insights under the guise of clinical review. Unlike the pre-2010 era, when delays were administrative overhead, today’s bottlenecks are data-capturing mechanisms—enabling payers to refine risk models using real-time care patterns withheld from providers, thus converting time spent on appeals into actuarial capital. The overlooked consequence is that technological streamlining is selectively suppressed not to preserve bureaucracy but to sustain an asymmetry where payment entities profit from temporal drag by transforming clinical delays into predictive intelligence.
Insurer Control Routines
Insurers maintain prior authorization to enforce cost-containment protocols that delegate administrative friction to providers and patients. This system leverages standardized denial or delay mechanisms to modulate service utilization without overtly restricting coverage, allowing payers to retain financial predictability amid competitive premium pricing. What’s underappreciated is how much clinical workflow disruption is not a flaw but a calculated feature—shifting labor costs to clinics ensures compliance while insulating insurers from direct accountability for access delays.
Regulatory Misalignment Incentives
State and federal regulations fail to penalize administrative complexity, inadvertently rewarding insurers for exploiting gaps between clinical standards and reimbursement rules. This dynamic allows prior authorization to persist as a low-risk compliance theater, where documentation satisfies oversight appearances without requiring real-time medical justification. The non-obvious reality is that regulators often equate procedural adherence with quality control, mistaking bureaucratic output for patient protection.
Clinical System Dependency Loops
Health systems tolerate prior authorization burdens because they become operationally dependent on insurer-defined workflows, embedding payer logic into electronic health records and staffing models. This creates a feedback loop where providers adapt to authorization demands as fixed constraints, reinforcing the perception that no alternative is viable. The overlooked insight is that familiarity with the burden—not its necessity—sustains its legitimacy, making streamlining technologies seem disruptive rather than corrective.
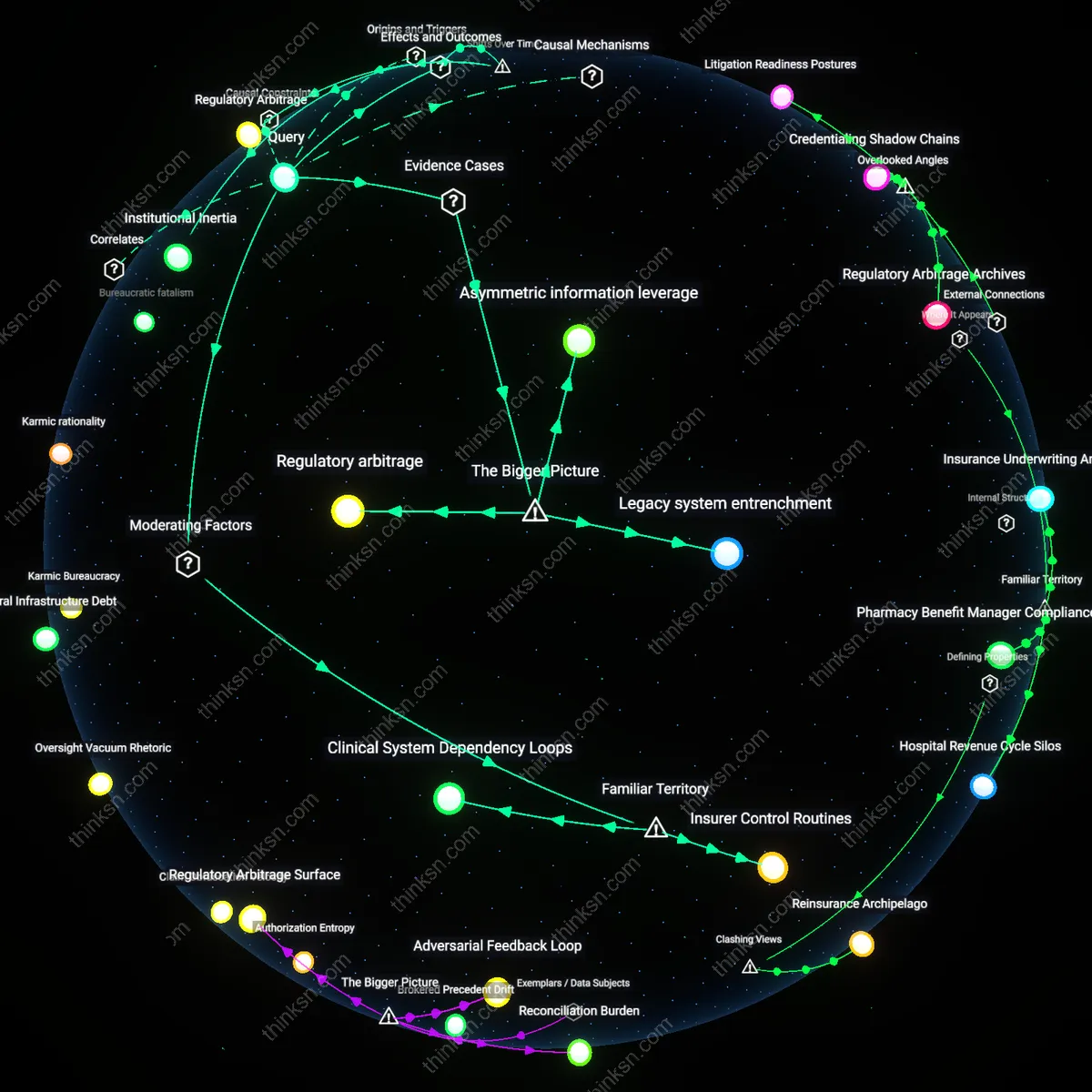
Regulatory arbitrage
Insurers maintain prior authorization bottlenecks because existing federal and state compliance frameworks allow them to shift medical oversight costs onto providers while remaining within legal bounds. Medicaid managed care organizations in states like Texas and Florida, for instance, exploit flexibility in network adequacy rules to delegate utilization control to administrative processes rather than clinical staffing, reducing their financial risk without violating access mandates. This reveals how compliance systems designed to ensure accountability can be subverted to legitimize cost-shifting, a dynamic rarely scrutinized because it operates at the intersection of legal permissibility and operational opacity.
Asymmetric information leverage
Pharmaceutical benefit managers like Express Scripts and OptumRx retain prior authorization complexity to amplify their influence over formulary adherence and rebate capture, particularly in specialty drug tiers. By structuring approval protocols around proprietary clinical justification models, they convert provider dependency on rapid approvals into a channel for enforcing payer-preferred drug selection, as seen in restricted access to biosimilars despite FDA equivalence. This demonstrates how technical gatekeeping functions are repurposed not for patient safety but for reinforcing supply chain control, a mechanism obscured by framing approvals as clinically necessary rather than commercially strategic.
Legacy system entrenchment
Hospital systems such as those in the legacy Epic-Cerner interface environments continue to support manual prior authorization pathways because integrated digital workflows would require synchronized upgrades across payer-provisioner data silos, which no single actor has incentive to lead. The fragmented EHR interoperability in large IDNs like CommonSpirit Health sustains this inertia, where IT modernization is deprioritized due to capital constraints and misaligned cost-benefit distributions between clinicians and administrators. The persistence of friction here is not from absence of technology but from pooled risk in upgrading systems, making systemic agility impossible even when point solutions exist.