Should Universities Demand Mental Health Disclosures for Housing?
Analysis reveals 7 key thematic connections.
Key Findings
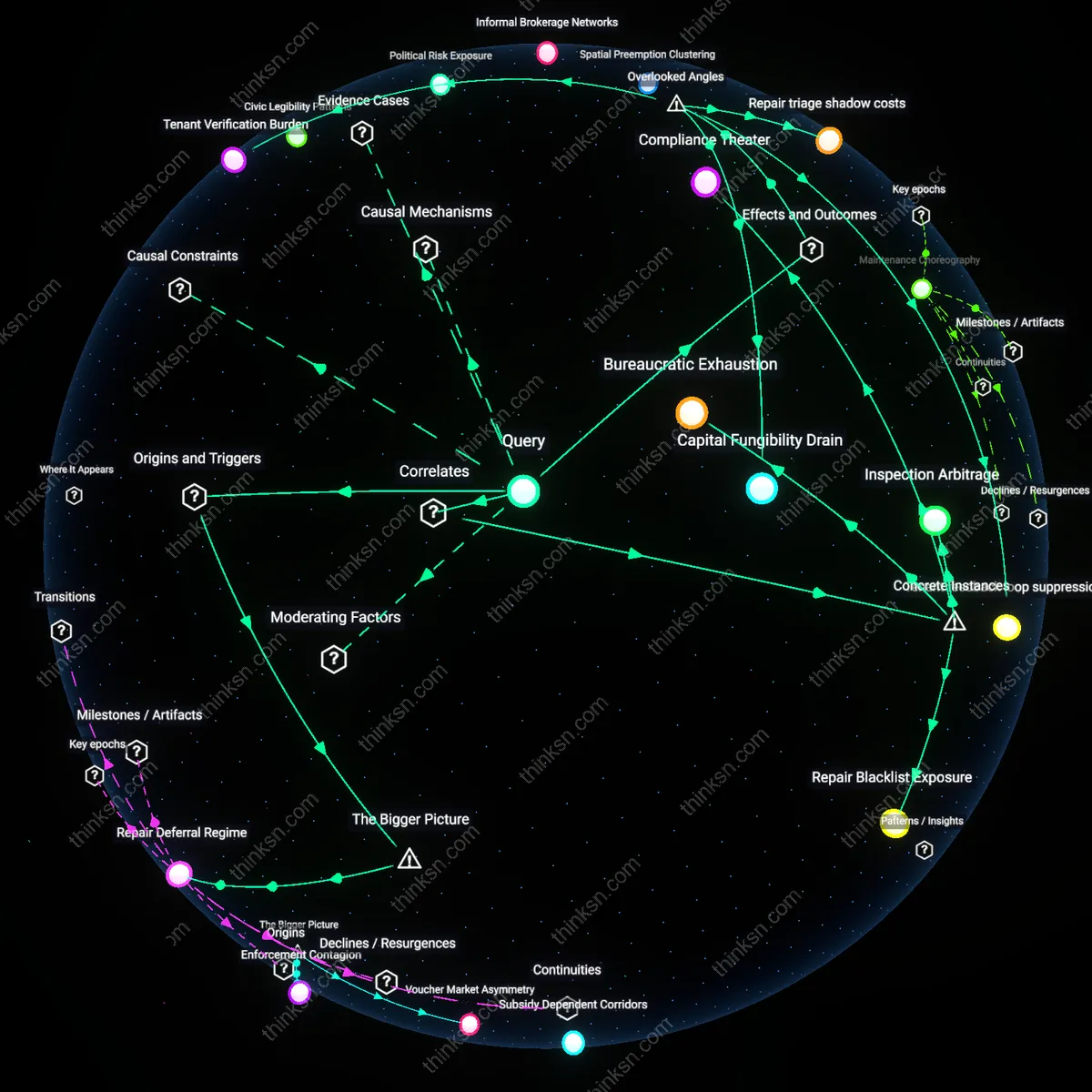
Administrative Visibility Regime
Universities should not require disclosure of ongoing mental-health treatment because such mandates intensify a post-1980s shift toward institutional risk management that redefines student privacy as a liability to be mitigated rather than a right to be protected. Beginning in the 1990s, particularly after high-profile campus crises, universities increasingly adopted protocols that treat personal health data as part of administrative oversight, aligning with federal safety compliance trends like Clery Act enforcement; this transforms clinicians, housing officers, and disability coordinators into de facto monitors, normalizing surveillance under the guise of accommodation. What is underappreciated is that this system does not primarily emerge from medical or therapeutic logics, but from legal defensibility—where the residual effect is not safer students, but a structural demand for visibility that undermines trust in support services.
Information Asymmetry Leverage
Universities should require disclosure of ongoing mental-health treatment because it enables administrators to allocate scarce housing resources more efficiently by identifying students whose accommodations are actively tied to measurable clinical interventions. Housing offices at large public universities, like those in the University of California system, face escalating demand for disability housing; requiring documentation from licensed providers creates a verifiable threshold that prevents self-referral inflation and ensures that limited single-occupancy or sensory-modified units go to students with treatment-backed needs. This mechanism counters the intuitive ethic of absolute privacy by revealing that controlled disclosure can enhance equity in resource distribution—what appears to be a privacy violation becomes a tool for fairer access, exposing how asymmetrical information can be leveraged to stabilize strained systems.
Institutional Risk Immunization
Mandating disclosure of mental-health treatment protects universities from liability by creating a documented chain of care that insulates them during student crises or adverse events. When a student in a modified housing arrangement experiences a psychiatric emergency, institutions like those in the Pennsylvania State System of Higher Education can demonstrate due diligence if they have required and maintained treatment records, transforming the accommodation process into a risk-mitigation protocol rather than a purely supportive act. This reframes the apparent conflict between privacy and care as a strategic alignment of student support and legal self-preservation, revealing that disclosure requirements are less about monitoring individuals and more about constructing institutional defenses against unpredictable harm.
Therapeutic Bureaucracy
Requiring disclosure institutionalizes mental-health treatment as a legitimate, normalized pathway to accessing resources, thereby reinforcing treatment adherence through structural incentives rather than stigma. At universities with integrated health and housing services, such as the University of Michigan, students who must submit treatment records for accommodation often experience increased continuity of care because the administrative act of disclosure synchronizes clinical and academic support systems. This contradicts the conventional view that disclosure deters help-seeking; instead, it shows how bureaucratic processes can become therapeutic conduits, where the demand for information functions not as surveillance but as a scaffold for sustained engagement.
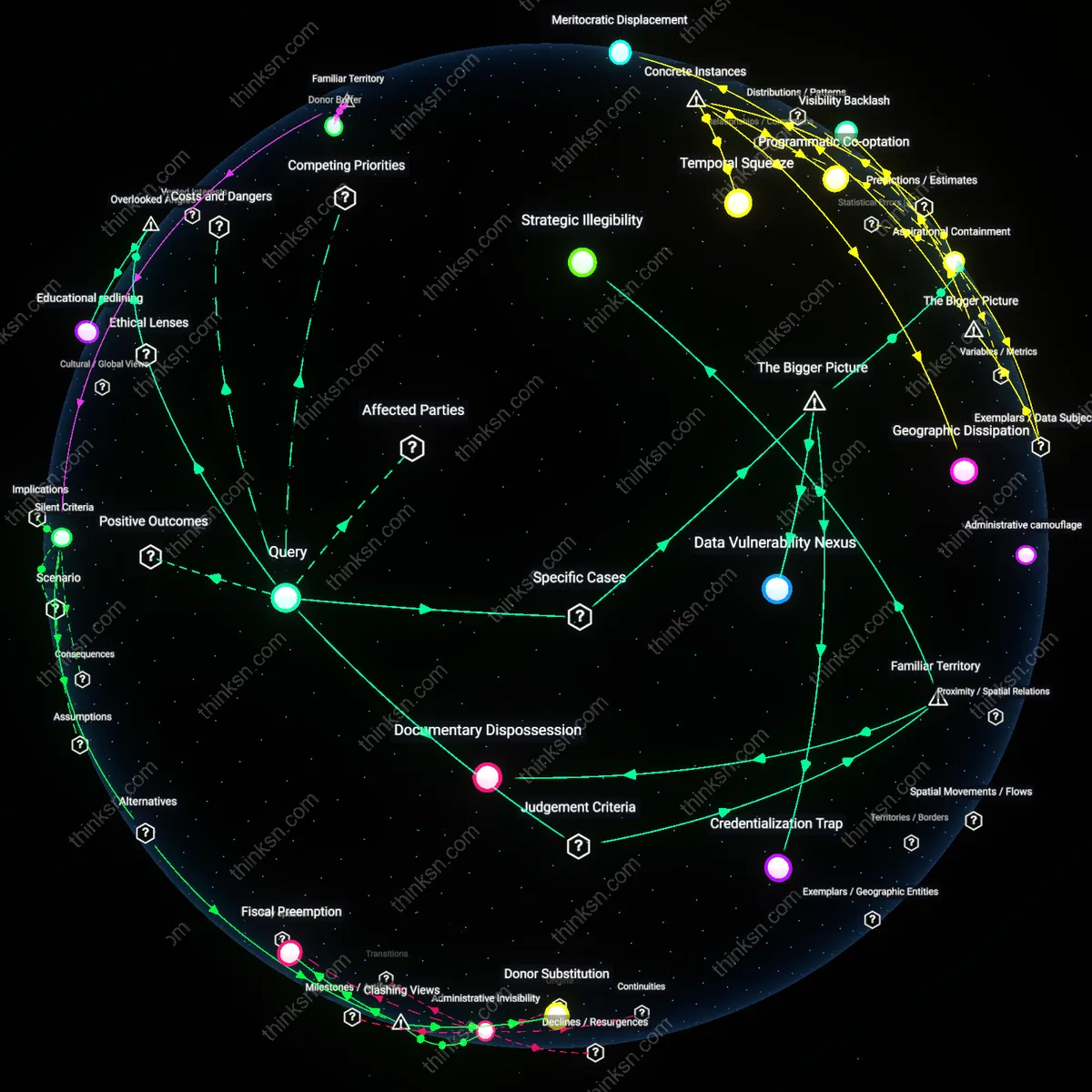
Therapeutic Surveillance Drift
Universities should not require disclosure of ongoing mental-health treatment for housing accommodations because such policies institutionalize a form of passive surveillance that gradually reshapes student self-disclosure norms through administrative routines rather than explicit coercion, leveraging bureaucratic categorization under the guise of care—this mechanism operates through housing intake forms that embed clinical presumptions into non-clinical systems, shifting the boundary of therapeutic oversight into everyday campus logistics in a way that is rarely challenged because it appears procedural rather than disciplinary, thus normalizing medical monitoring under administrative neutrality. This creates Therapeutic Surveillance Drift—the unnoticed migration of clinical scrutiny into non-clinical decision points through seemingly neutral documentation requirements—which distorts student autonomy not through overt force but through incremental absorption of personal data into governance structures that were originally designed for logistical convenience rather than health oversight, fundamentally altering the student-institution relationship in a way that evades traditional privacy frameworks.
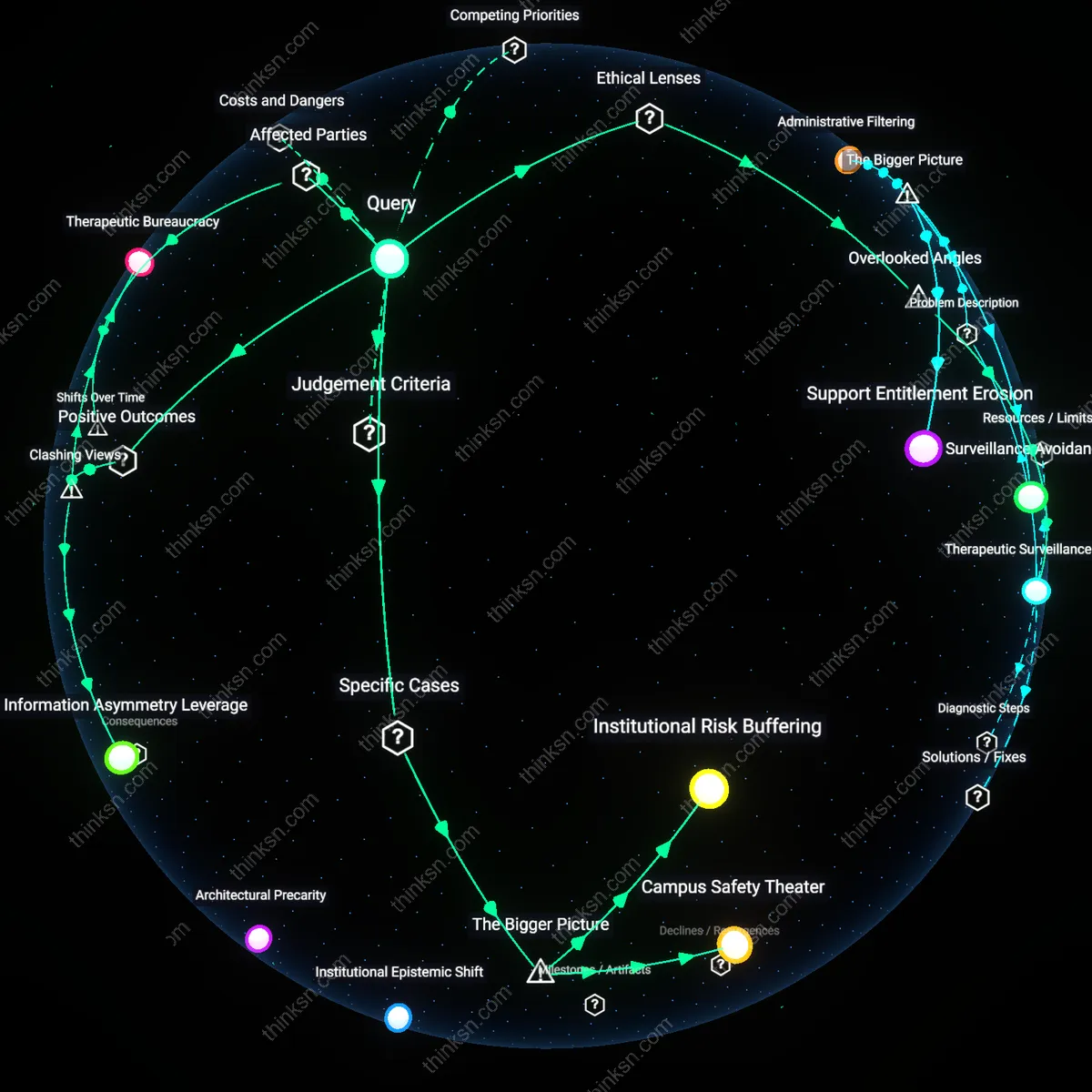
Institutional Risk Buffering
Universities require disclosure of ongoing mental-health treatment because legal compliance units prioritize minimizing liability over student autonomy, especially in residence halls where universities assume greater in loco parentis responsibility. Higher education administrators at schools like the University of Michigan and Penn State have institutionalized medical disclosure forms for housing accommodations, justified by potential liability in suicide or self-harm incidents—transforming medical privacy into a risk-management variable. This reveals how legal risk, not clinical need, becomes the dominant criterion in accommodation decisions, making the university an administrative legal shield rather than a neutral support provider. The non-obvious consequence is that mental health disclosures are treated less as therapeutic tools and more as contractual defenses in a preemptive litigation landscape.
Campus Safety Theater
Housing staff at universities such as the University of Oregon use mental health disclosure not to support care, but to categorize students into risk tiers that determine dorm assignments, often relocating 'high-risk' individuals to monitored or isolated spaces. This operationalizes psychological treatment status as a proxy for behavioral threat, driven by campus police and housing departments' shared goal of preventing high-profile incidents—regardless of actual impairment. The result is a covert segregation system justified under medical pretenses but motivated by public relations and safety optics. The overlooked mechanism is how therapeutic information becomes repurposed into spatial control, normalizing surveillance under the guise of accommodation.