Fewer Clinic Visits, More Data Stress for Heart Patients?
Analysis reveals 6 key thematic connections.
Key Findings
Clinical Triage Efficiency
Reducing clinic visits in the Veterans Health Administration’s telehealth program for heart-failure patients revealed that automated vital sign uploads increased nurse workload due to unstructured data influx, exposing a mismatch between data volume and clinical staffing models. Nurses spent more time filtering false alarms and low-priority signals than managing critical cases, undermining the efficiency gains expected from remote monitoring. This shows that efficiency in patient throughput can be offset by inefficiency in clinician attention allocation when data streams lack embedded triage logic, a trade-off rarely accounted for in remote care rollout designs.
Data Sovereignty Friction
In the NHS’s ‘Wearables for Heart Failure’ pilot in Greater Manchester, patients expressed distress over continuous data collection by private vendors like Philips, fearing loss of control over how biometrics were stored and used—despite fewer in-person visits improving convenience. The erosion of perceived autonomy intensified when patients discovered their data could be shared with third-party analysts without explicit re-consent, triggering opt-outs that degraded program continuity. This instance reveals that data overload is not merely a provider-side challenge but also a patient-experienced breach of informational self-determination when monitoring bypasses transparent governance.
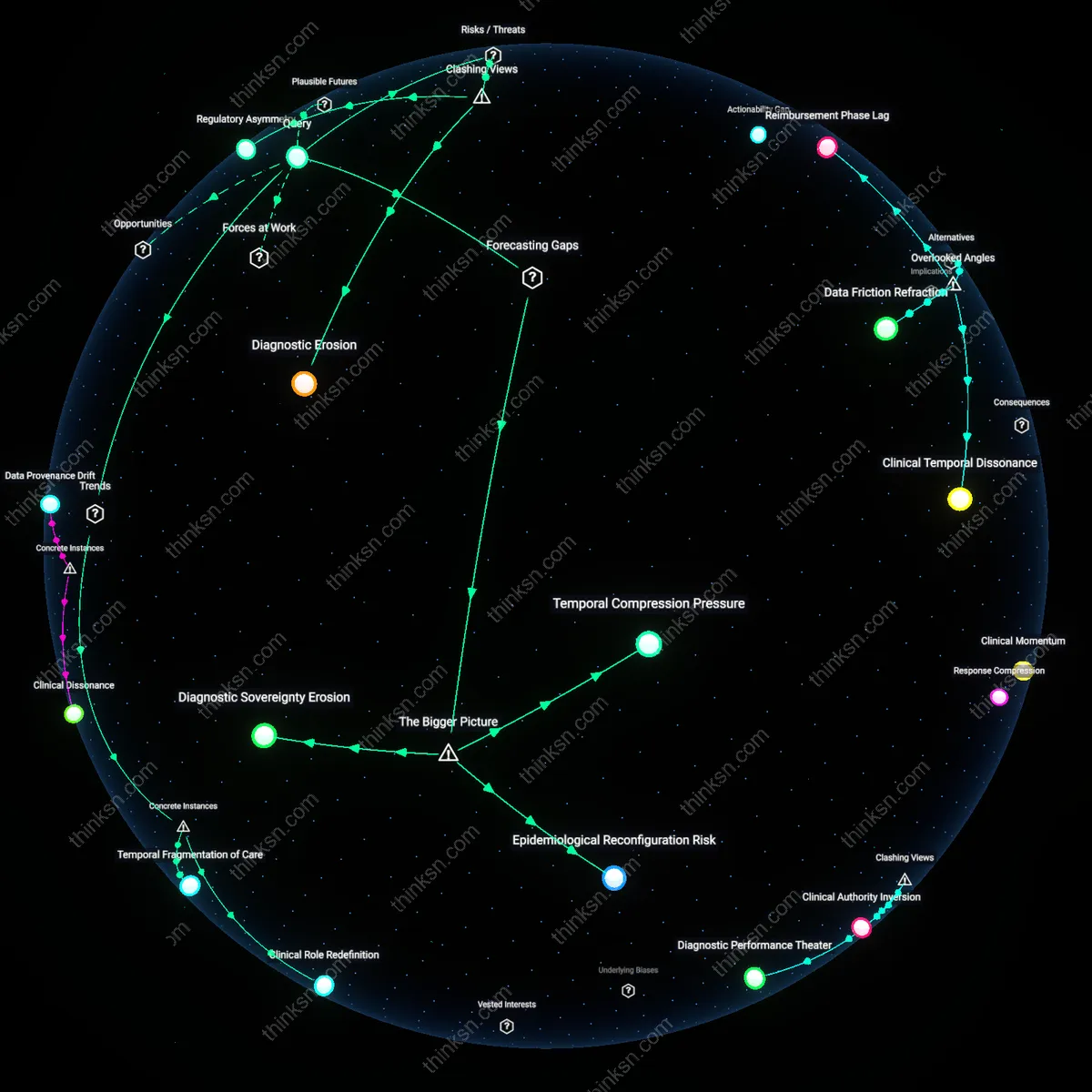
Diagnostic Delay Risk
A 2021 study of remote monitoring in Cleveland Clinic’s Home Telemonitoring Program found that reduced visit frequency, combined with intermittent patient self-reporting, led to delayed recognition of gradual ejection fraction decline in 18% of participants, as subtle trends were obscured by data noise and irregular transmission. Clinicians relied on thresholds for alerts, missing subclinical progression that would have been detected during routine physical assessments like jugular venous pressure observation. This demonstrates that minimizing visits without compensatory analytical tools risks substituting acute crisis prevention for chronic deterioration detection, privileging operational efficiency over longitudinal diagnostic sensitivity.
Clinical Dehumanization
Reducing clinic visits in remote heart-failure monitoring risks eroding the physician-patient relationship by replacing embodied clinical encounters with algorithmic surveillance. This shift operates through institutionalized efficiency mandates in value-based care systems, where cost containment and data productivity are prioritized under neoliberal health policy frameworks—particularly in U.S. Medicare Advantage programs that incentivize telemonitoring over in-person visits. What is underappreciated in public discourse is that the 'convenience' of fewer visits is not merely logistical but ethically transformative, as it redefines care from relational accountability to data compliance, subtly displacing empathy with analytics.
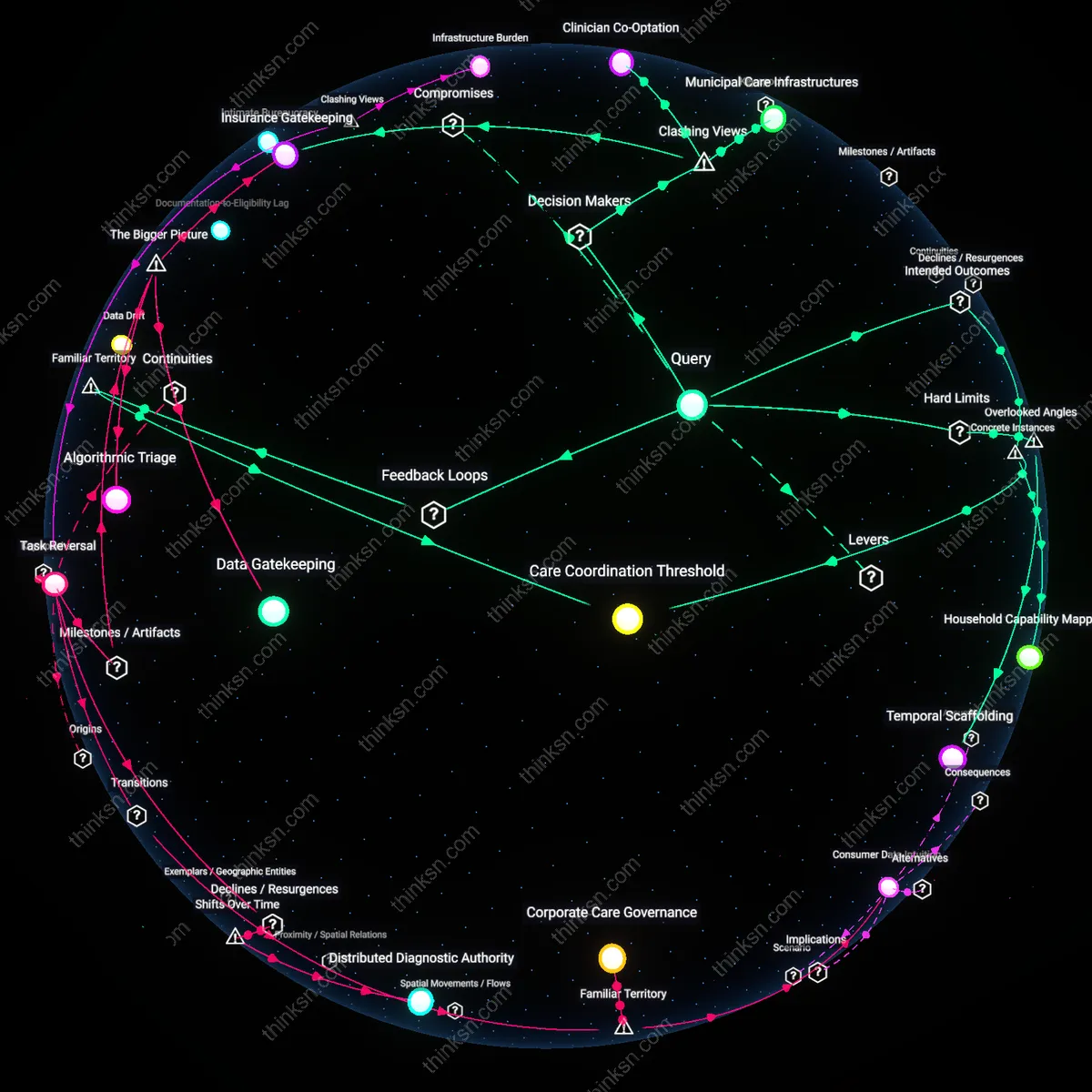
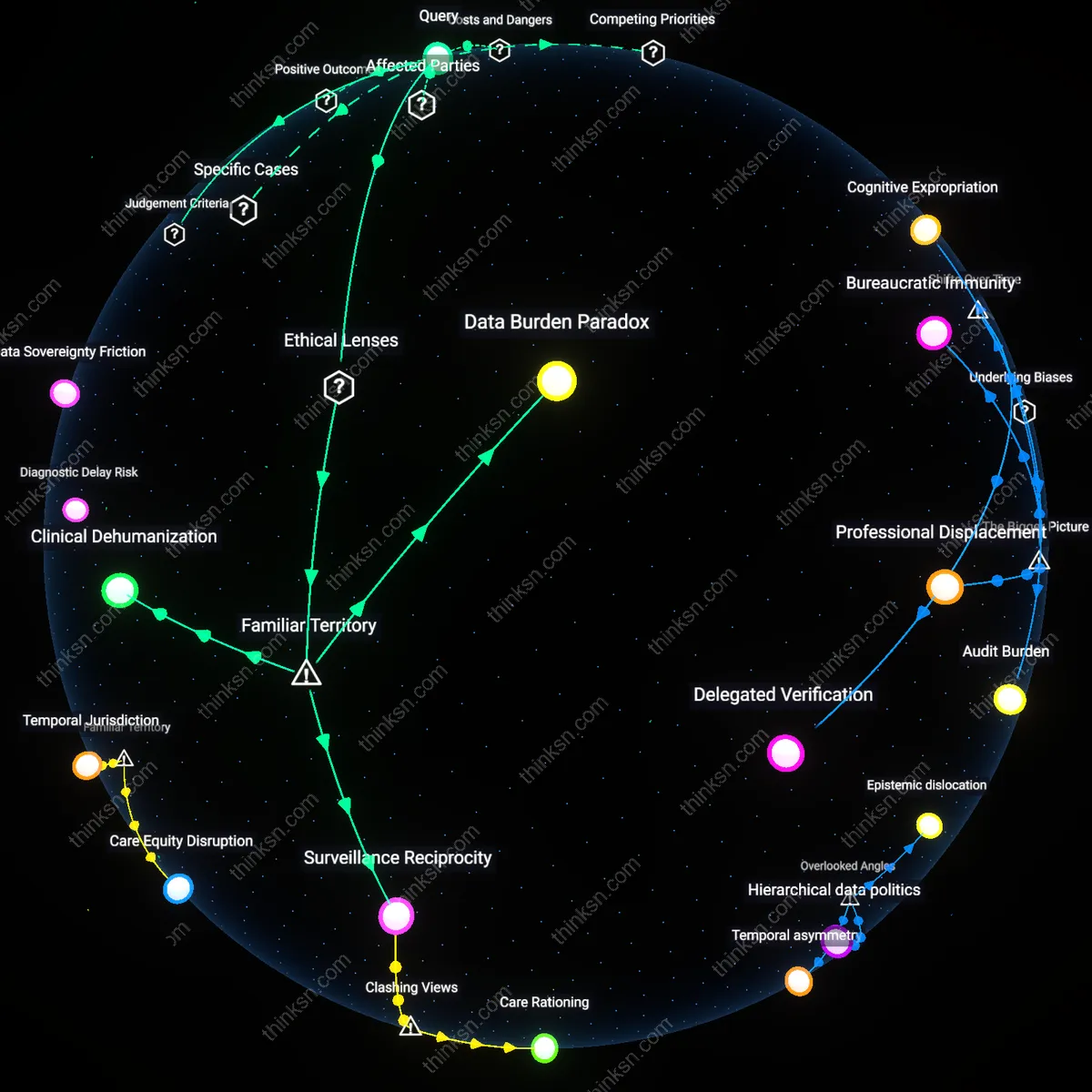
Data Burden Paradox
Remote monitoring generates excessive patient-generated health data that overwhelms clinicians, undermining the intended efficiency of reduced visits. This occurs within clinical workflows governed by utilitarian principles that assume more data leads to better outcomes—embedded in Meaningful Use regulations and EHR-driven performance metrics—yet the mechanism of data aggregation outpaces sense-making capacity, especially in safety-net hospitals with understaffed cardiology teams. The non-obvious insight is that the public assumes data abundance equates to control, but in practice, uncurated inputs create cognitive overload, shifting error risk from under-monitoring to misinterpretation.
Surveillance Reciprocity
Patients experience remote monitoring as asymmetric surveillance when they transmit data frequently but receive minimal feedback, amplifying distrust despite fewer clinic visits. This dynamic is rooted in liberal bioethical frameworks that emphasize patient autonomy while neglecting reciprocal obligations of clinicians to respond—a gap reinforced by reimbursement models like CMS’s Remote Patient Monitoring (RPM) codes, which pay for data collection but not for relational follow-up. The underappreciated reality is that the public equates monitoring with care, yet the one-way flow of information often replicates power imbalances long criticized in medical paternalism, now masked as technological engagement.