Do Drug Makers Studies Earn More Patient Trust Than Independent Research?
Analysis reveals 5 key thematic connections.
Key Findings
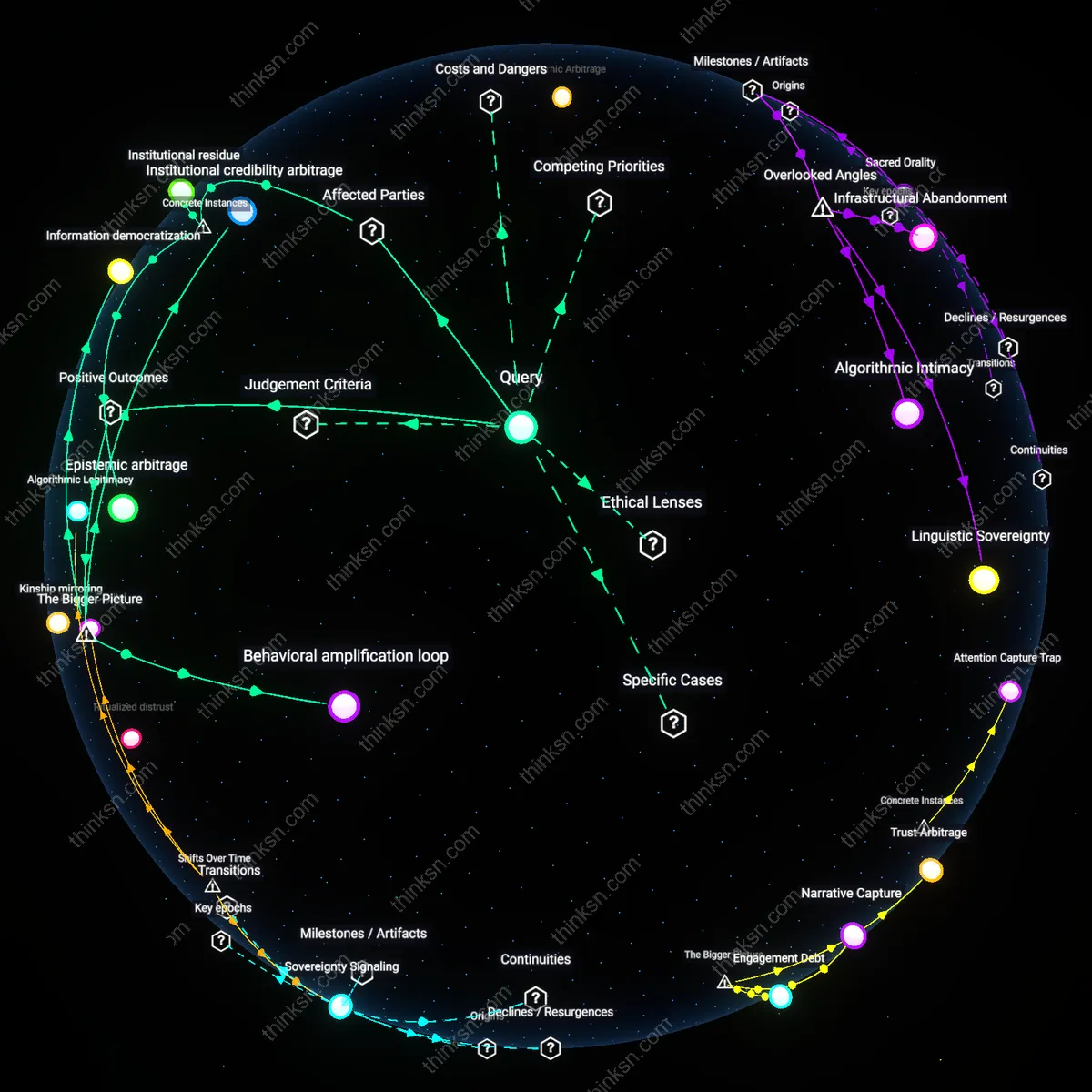
Regulatory arbitrage pathways
Drug manufacturers systematically exploit jurisdictional misalignments by generating real-world evidence in countries with weaker oversight to pre-empt stricter post-marketing requirements elsewhere, creating a backdoor standardization that undermines independent scrutiny; because regulatory bodies in high-income nations often accept foreign real-world data as preliminary validation, firms channel studies through permissive environments where methodological flaws or selective reporting face less challenge, effectively colonizing evidence norms through asymmetry rather than scientific merit—this dynamic is rarely examined because most conflict-of-interest debates focus on financial ties rather than geographically nested regulatory stratagems, yet it reshapes evidentiary hierarchies from the periphery inward.
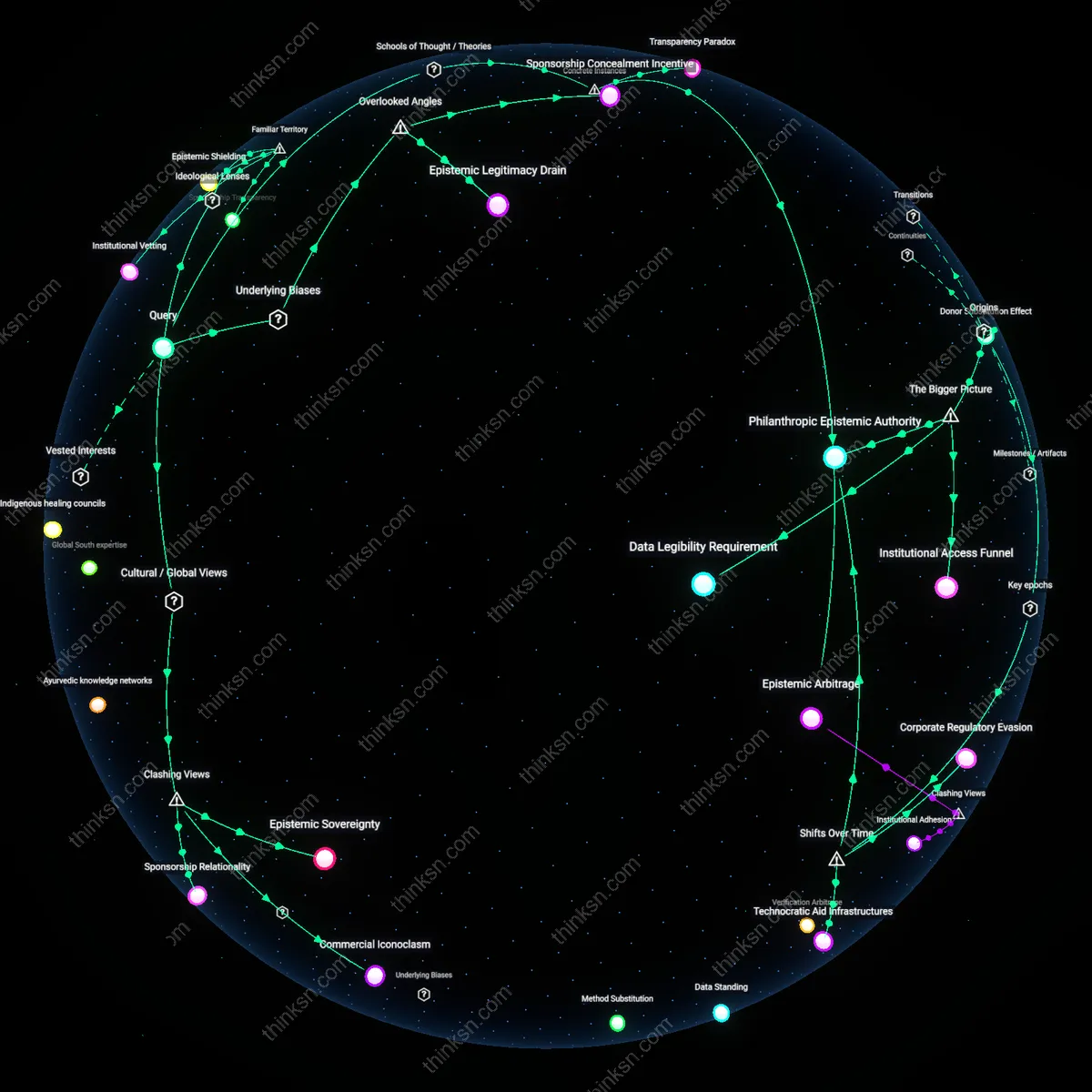
Clinical trial infrastructures
When drug manufacturers control the collection of real-world evidence, they extend the operational logics of pre-approval trials—such as narrowly defined endpoints and curated patient populations—into post-market settings, thereby distorting what counts as clinically meaningful; this procedural continuity hides how manufacturer systems actively devalue outcomes not tracked during development, like rare or delayed adverse events managed outside structured follow-ups, which independent studies are more likely to detect precisely because they lack infrastructure alignment—this overlooked continuity between trial machinery and real-world data pipelines sustains blind spots not by deception but through embedded procedural inertia.
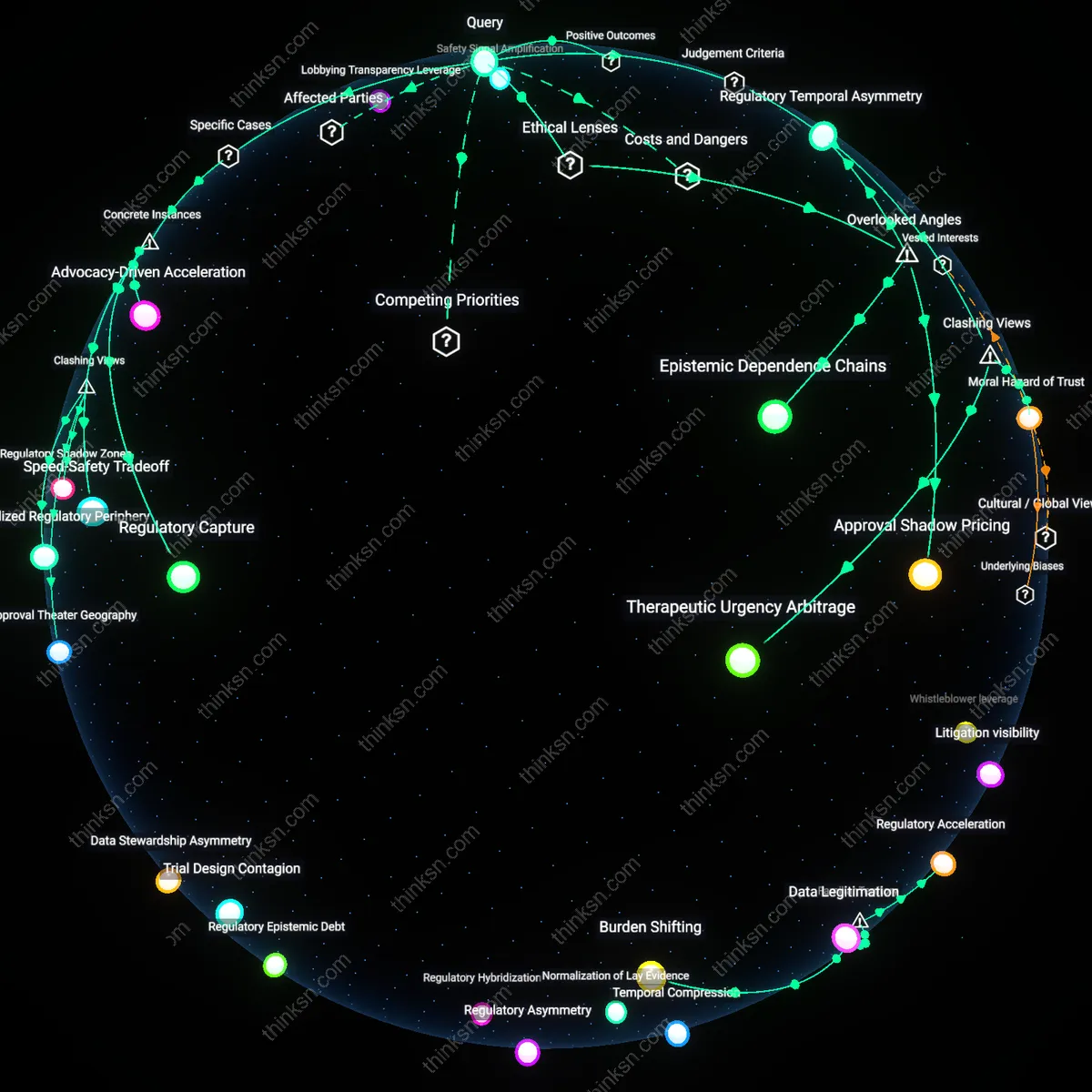
Evidentiary timing markets
Pharmaceutical firms accelerate real-world evidence publication not solely to inform care but to saturate medical discourse ahead of independent studies, effectively cornering the window in which clinicians and payers form conclusions about drug performance, and because rapid dissemination creates perception of validation, slower but more rigorous post-marketing analyses struggle for traction even when they contradict manufacturer claims—this temporal weaponization of evidence is rarely discussed because conflict debates center on bias or funding rather than the strategic sequencing of information release, yet speed becomes a form of epistemic dominance independent of truth.
Commercial Epistemology
Patients should distrust manufacturer-collected real-world evidence more than independent studies because pharmaceutical firms fund and design data collection systems—like electronic health record partnerships or patient support programs—that structurally embed commercial objectives into knowledge production. These systems often treat adverse events as service issues rather than safety signals, and channel data through proprietary analytics that obscure underlying assumptions, effectively privatizing the interpretation of public health outcomes. Independent studies, by contrast, are subject to peer scrutiny and replication, making them resistant to such epistemic capture. The phenomenon illustrates how private control over data infrastructure enables a form of knowledge governance where market logic displaces scientific disinterestedness, distorting the evidentiary basis of medical decisions.
Surveillance Trade-off
Patients should distrust manufacturer-collected real-world evidence more than independent studies because the expansion of industry-led digital surveillance—through apps, wearables, and adherence tracking—enables unprecedented data volume but erodes methodological transparency in exchange for patient engagement. Firms like Novartis or Pfizer deploy these tools under the banner of personalized medicine, yet the data they collect are often siloed, analyzed with undisclosed algorithms, and selectively reported to regulators, privileging signal detection over bias correction. Independent post-marketing studies, while slower and sparser, maintain auditability and adversarial review, offering compensatory rigor where commercial systems prioritize scale and speed. This trade-off exposes how the drive for continuous health monitoring inadvertently sacrifices epistemic accountability, entrenching a surveillance dynamic where data abundance masks evidentiary fragility.