How Far Should We Trust FDA Amid Pharma Lobby Influence?
Analysis reveals 11 key thematic connections.
Key Findings
Moral Hazard of Trust
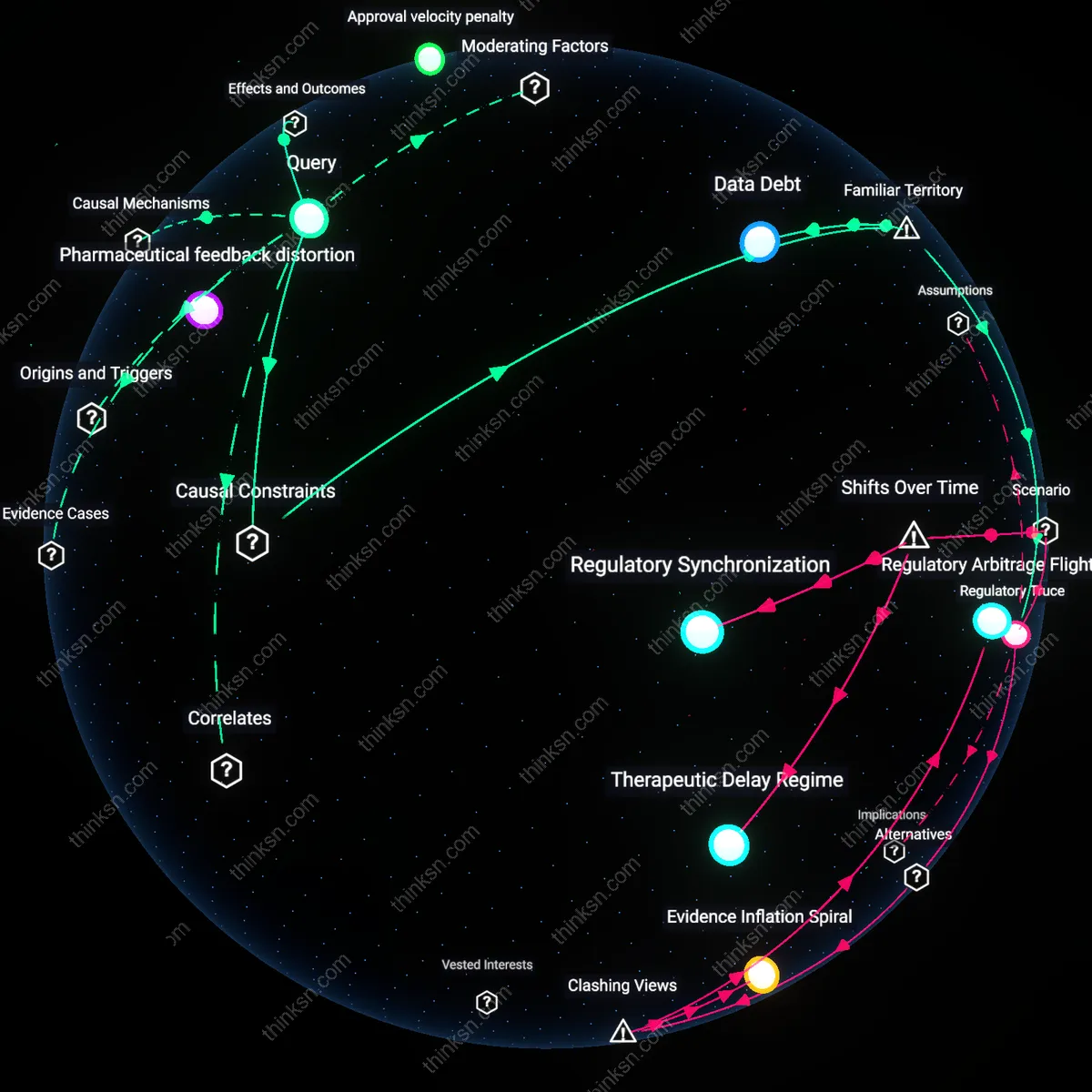
Citizens should treat the FDA’s safety commitment as a managed illusion because independent oversight is structurally avoided through the legitimizing function of procedural compliance. The agency’s gold-standard image stems from visible processes—advisory committees, public dockets, statistical rigor—but these serve more to validate decisions ex post than to constrain lobbying-driven timelines. When lobbying shapes trial design or endpoint selection before submission, the safety framework merely ratifies choices made elsewhere. The friction here is that transparency and methodological rigor, usually seen as safeguards, instead provide moral cover for regulatory capture, transforming safety as practice into safety as pageantry.
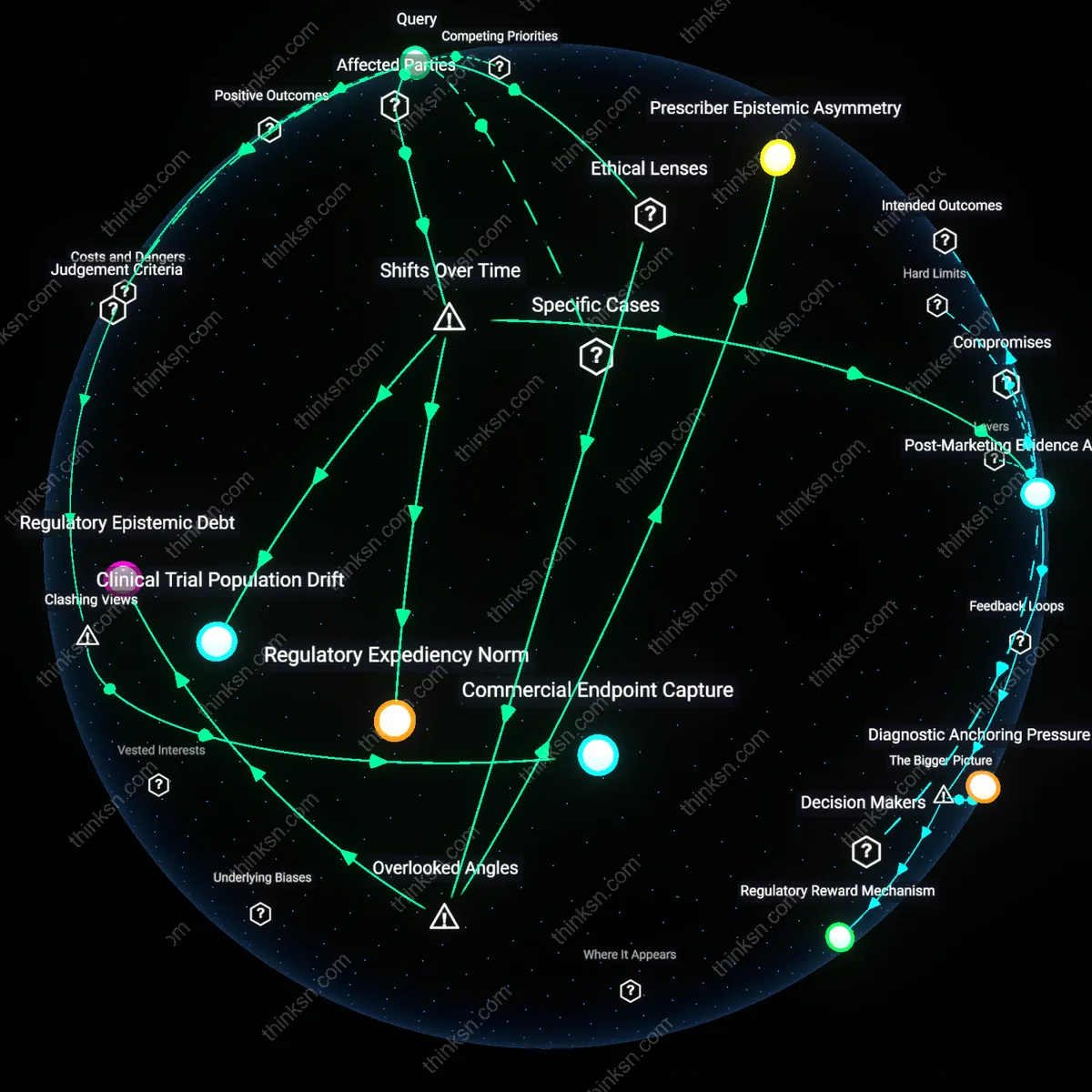
Therapeutic Urgency Arbitrage
Citizens must recognize that pharmaceutical lobbying exploits diagnostic categorization to accelerate approvals under the moral banner of unmet medical need, thereby short-circuiting safety scrutiny. By redefining diseases into narrower, biomarker-defined subpopulations—such as specific genetic mutations in cancers—firms create pseudo-urgent markets eligible for breakthrough therapy designation. This reclassification, driven more by regulatory strategy than epidemiological shift, enables speed without overtly violating safety standards, since risk-benefit calculations are confined to narrowly framed patient groups. The overlooked mechanism is that urgency is not discovered but manufactured through disease segmentation, making safety appear preserved while fundamentally altering the terms of evaluation.
Regulatory Trust Anchors
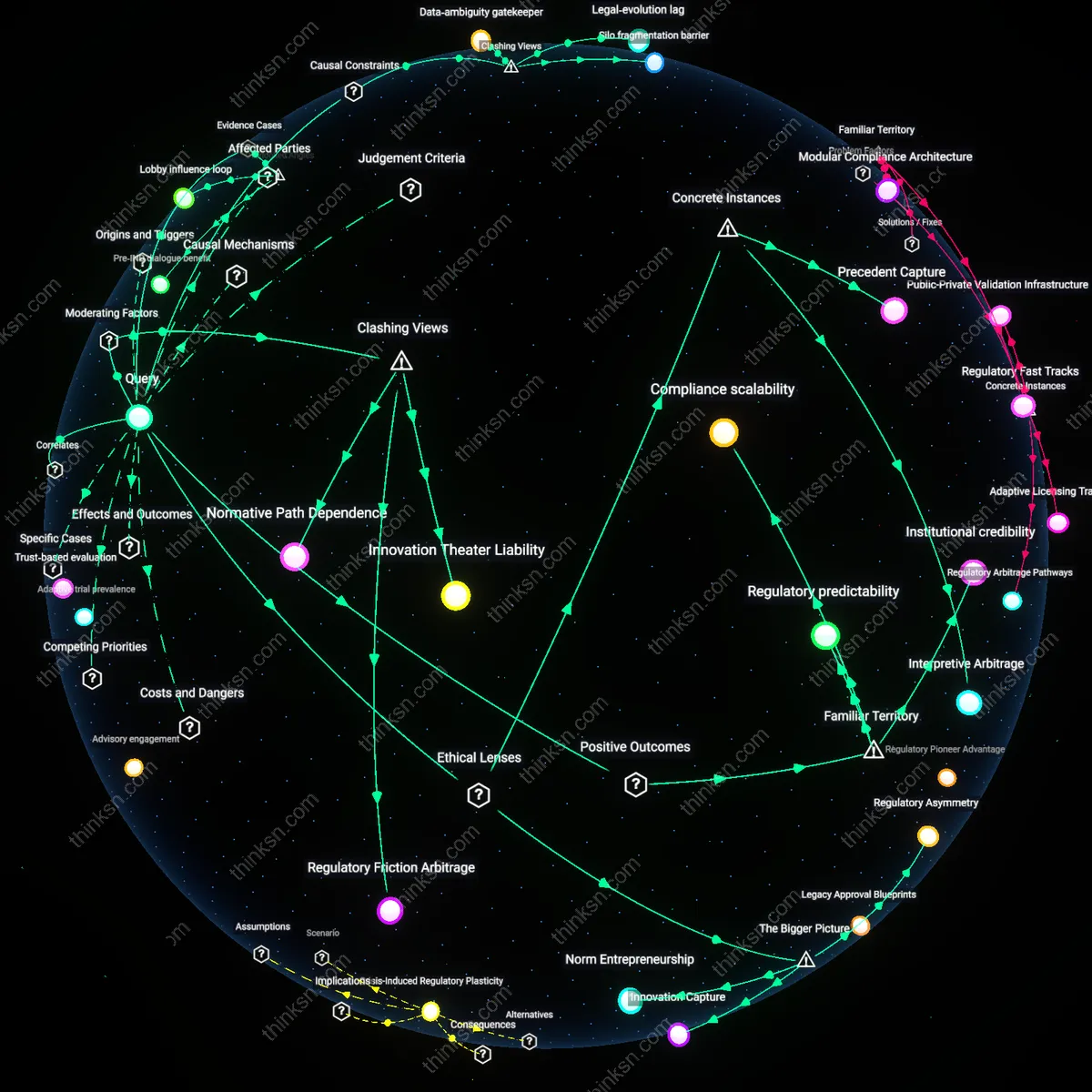
Citizens should prioritize transparent FDA review milestones to anchor public trust in drug safety despite lobbying pressures. When the FDA publicly stages its approval process—such as through advisory committee meetings, risk evaluation and mitigation strategies (REMS), and clinical trial data disclosures—patients, physicians, and advocacy groups gain observable checkpoints that signal rigorous evaluation, even when fast-tracked pathways like Breakthrough Therapy designation are used. This visibility counterbalances concerns about pharmaceutical influence by making safety protocols legible and accountable, reinforcing the perception that speed does not compromise scrutiny—thus stabilizing confidence in both innovation and oversight.
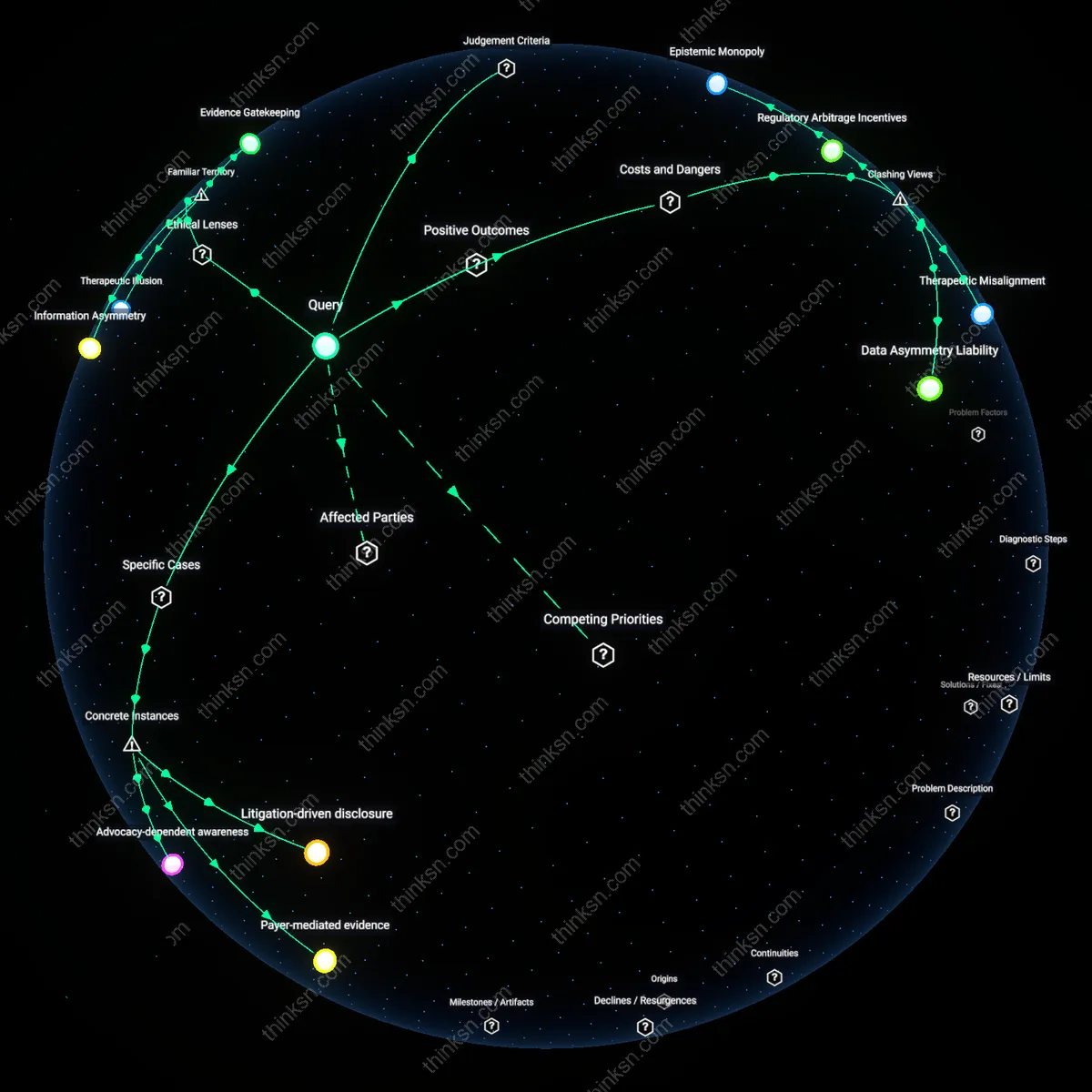
Lobbying Transparency Leverage
Citizens should use public lobbying disclosures, such as those logged in the FDA’s External Information System and Open Payments database, to map influence and reward pharmaceutical firms that align speed with demonstrated safety rigor. When companies advocate for expedited approvals but also voluntarily publish full trial data or fund post-market surveillance, they convert lobbying from a perceived threat into a transparency tool, enabling watchdogs and investors to distinguish between responsible acceleration and undue pressure. This reframes lobbying not as a hidden force but as a trackable investment in regulatory dialogue, where public accountability becomes a competitive advantage.
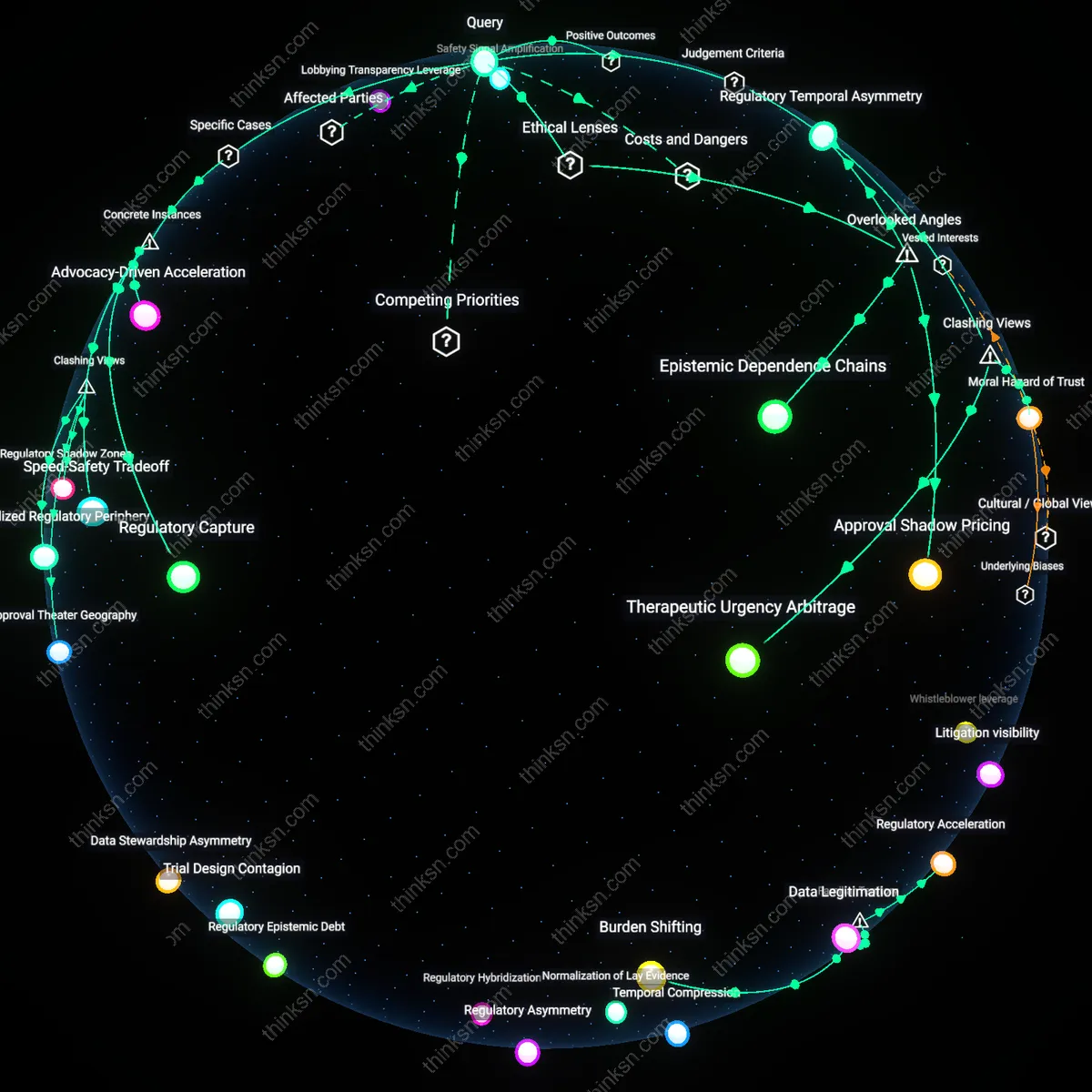
Safety Signal Amplification
Citizens should treat patient-reported adverse events through established channels like MedWatch as a democratic counterweight to pharmaceutical lobbying, directly feeding real-world data into FDA risk assessment loops. When individuals and clinicians consistently report side effects post-approval, they activate a distributed early-warning system that sustains safety vigilance beyond the pre-approval phase, effectively extending the FDA’s sensory reach. This grassroots surveillance becomes especially potent during accelerated approvals, turning the public from passive beneficiaries into active stewards of drug safety and tempering the downstream risks that lobbying-driven speed might otherwise amplify.
Regulatory Temporal Asymmetry
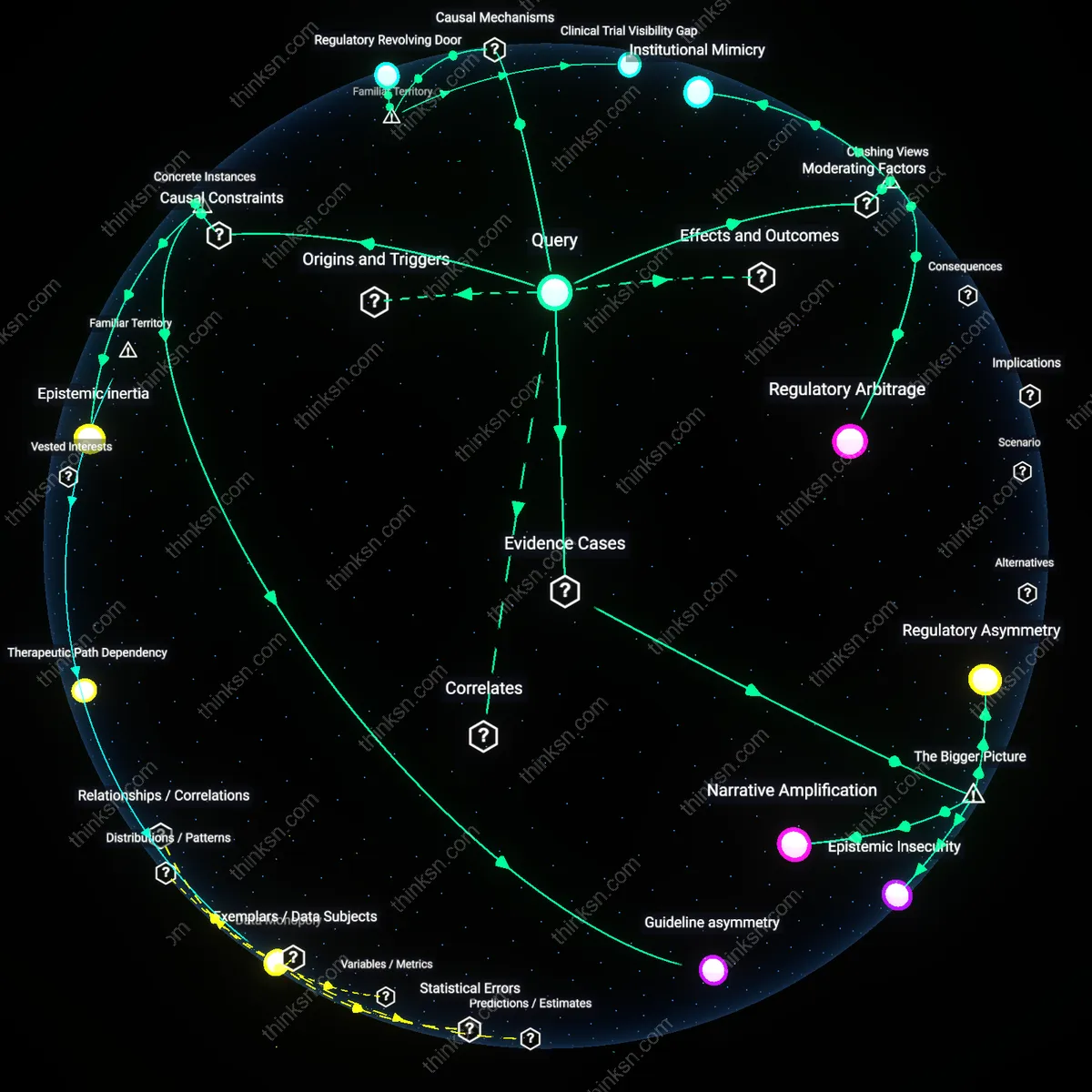
Citizens should prioritize monitoring the differential speed of FDA review cycles for novel biologics versus generic equivalents because pharmaceutical lobbying disproportionately compresses approval timelines for innovative drugs while generic reviews face unpublicized delays, exploiting the ethical asymmetry between innovation incentives and equitable access. This occurs through the Prescription Drug User Fee Act (PDUFA) performance metrics, which create binding review deadlines for new molecular entities but no equivalent pressure for generics, allowing political energy and lobbying to skew time allocation under the guise of safety—yet this temporal imbalance quietly erodes public trust in regulatory neutrality. The overlooked mechanism is not lobbying per se, but how legally codified time pressures serve as a covert channel for influence, reframing safety delays as bureaucratic inefficiency rather than strategic prioritization.
Epistemic Dependence Chains
Citizens must interrogate how the FDA’s reliance on industry-generated clinical trial data creates an epistemic dependency that constrains its safety commitment independently of lobbying pressure, because internal agency reviewers lack independent datasets or replicative infrastructure to challenge sponsor conclusions, making rejection politically and scientifically costly. This dependence is institutionalized through 21st Century Cures Act provisions that incentivize use of real-world evidence supplied directly by manufacturers, effectively outsourcing evidentiary validation to the same entities seeking approval. The underappreciated risk is that lobbying doesn’t need to corrupt individuals—it embeds persuasive advantage in the very structure of knowledge production, making safety evaluations structurally deferential even in the absence of overt influence.
Approval Shadow Pricing
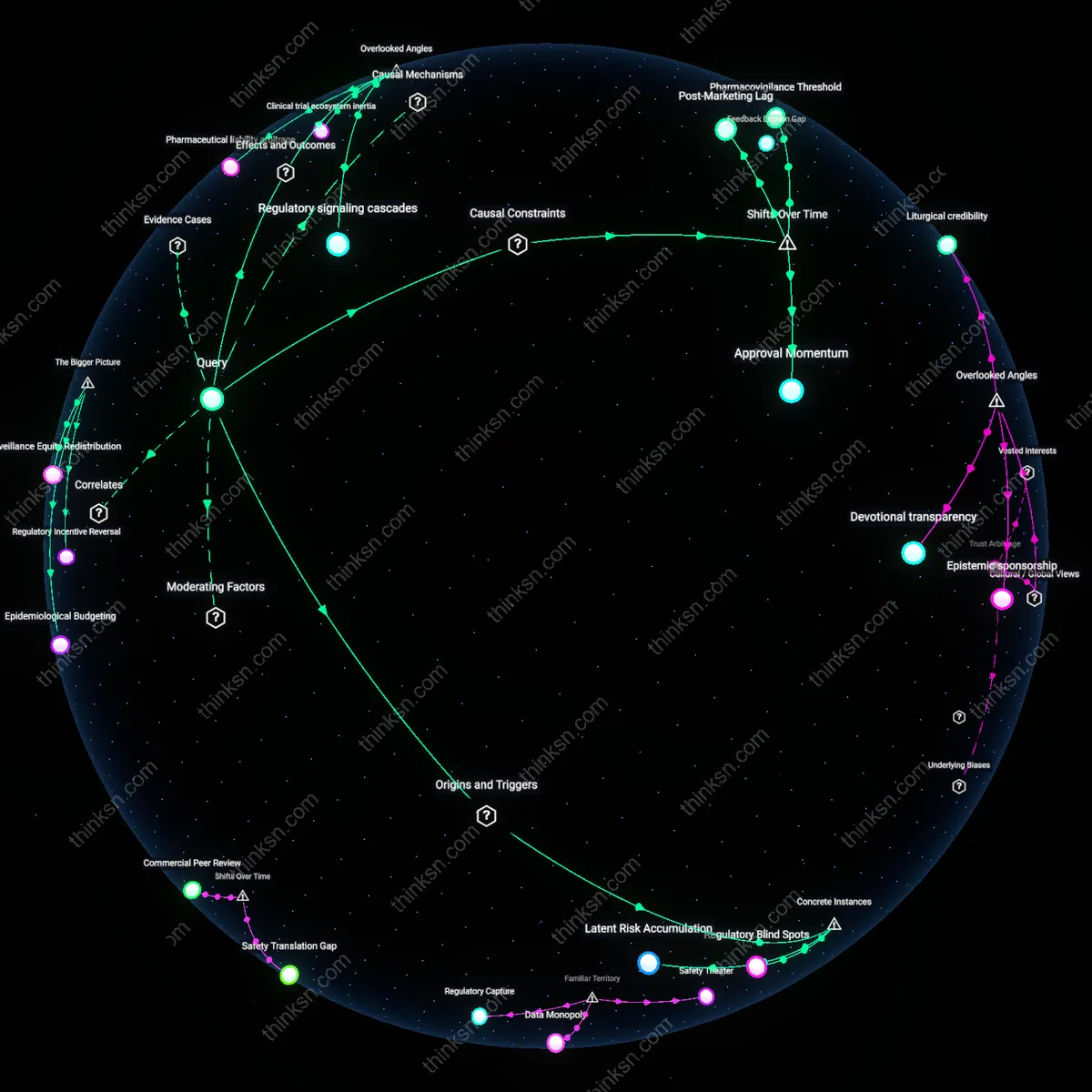
Citizens should treat accelerated FDA approvals as generating shadow prices for future regulatory leniency, where each fast-tracked drug establishes an implicit benchmark that lobbying groups later invoke to challenge more rigorous reviews, leveraging precedent as a quasi-legal doctrine within informal agency deliberations. This occurs through internal FDA reliance on ‘consistency’ in decision-making, wherein past concessions—often made under political pressure or public health emergency—are retroactively framed as standards of reasonable scrutiny, thereby narrowing the agency’s ethical discretion over time. The overlooked dynamic is that lobbying gains are not only secured in real-time approvals but are capitalized across a portfolio of future decisions, turning isolated compromises into systemic erosion of safety thresholds through intertemporal precedent arbitrage.
Regulatory Capture
The 1992 Prescription Drug User Fee Act (PDUFA) created a direct financial dependency of the FDA on pharmaceutical companies by allowing drug sponsors to pay fees that fund the agency’s review process, which shortened approval times but embedded industry priorities into the review timeline structure; this mechanism, evidenced by the rapid rise in approved drugs post-1992—even for marginal therapies like Wyeth’s Torisel—reveals how public agencies can internalize sponsor incentives under resourced scarcity, an effect rarely acknowledged in public discourse about drug safety.
Speed-Safety Tradeoff
The accelerated approval of Pfizer’s COVID-19 vaccine in December 2020, while a public health necessity, relied on truncated real-world safety data due to political and corporate pressure amplified by Operation Warp Speed; this instance, centered at the FDA’s White Oak campus and involving emergency use authorization decisions by career biostatisticians under public scrutiny, exposes how temporal compression in regulatory review can shift risk assessment from pre-market verification to post-market surveillance—normalizing reactive over proactive safety governance.
Advocacy-Driven Acceleration
In 2016, the FDA’s approval of Exondys 51 (eteplirsen) for Duchenne muscular dystrophy, despite rejected efficacy data and internal scientist dissent, was directly influenced by sustained lobbying and patient advocacy led by Parent Project Muscular Dystrophy and Sarepta Therapeutics; this decision, originating from political testimony and media campaigns centered in Washington, D.C., reveals how moral urgency framed by disease advocacy groups can override technical consensus within regulatory bodies, reframing safety delays as ethical failures.