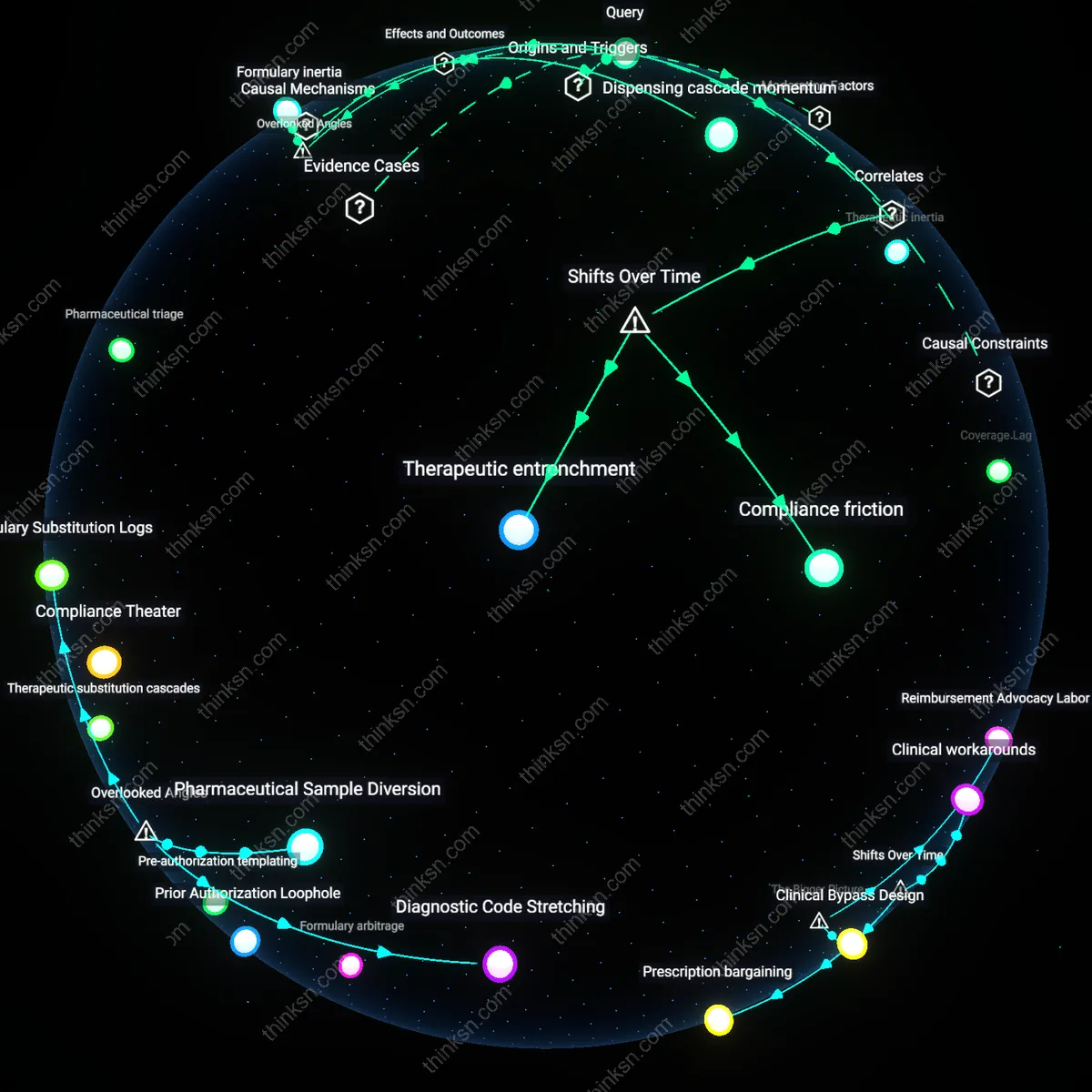
Reimbursement Advocacy Labor
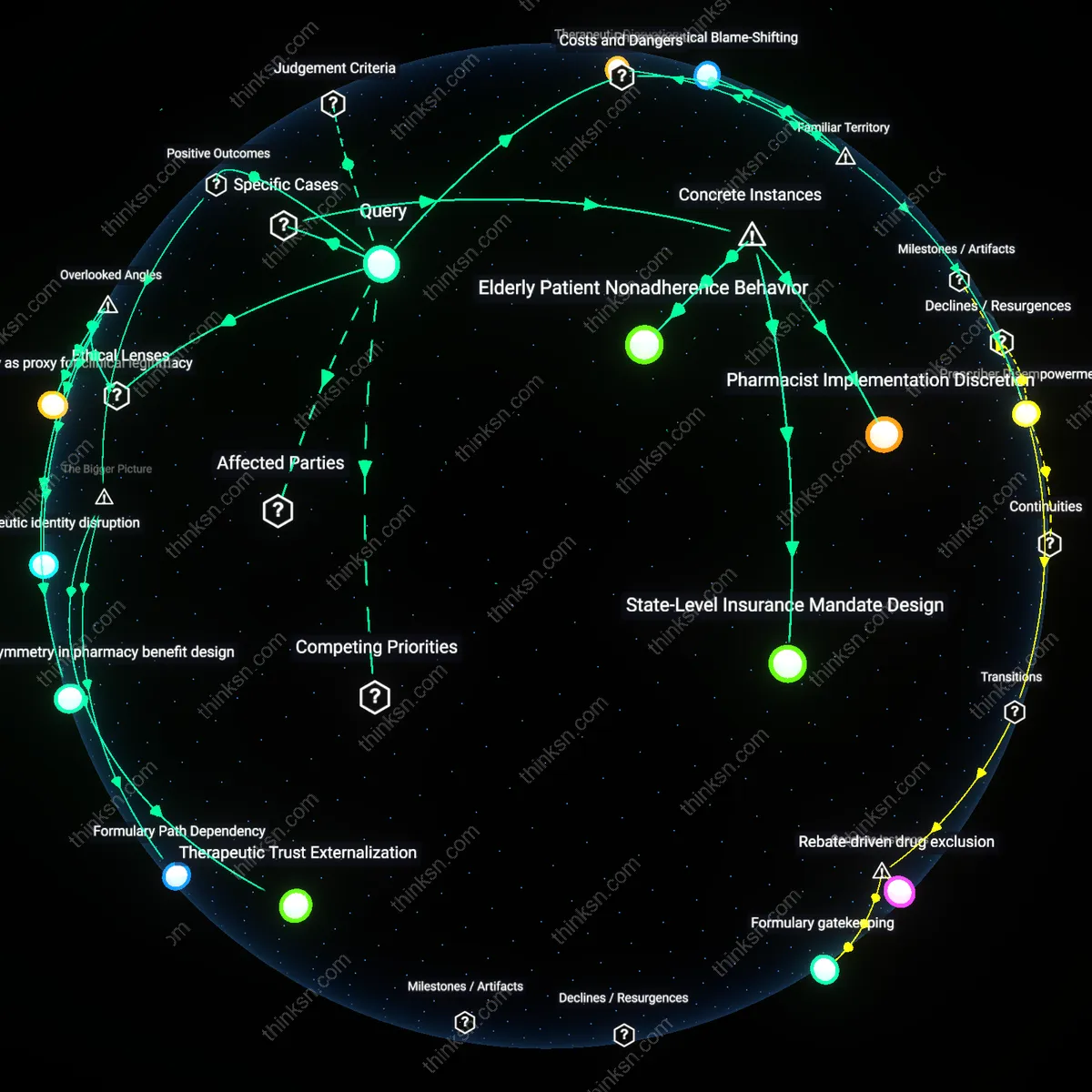
Doctors began developing workaround strategies to secure guideline-recommended treatments in the late 1990s, as managed care expansion in the U.S. introduced prior authorization and formulary restrictions that disrupted standard clinical pathways. This shift forced physicians—particularly in oncology and cardiology—to invest unseen administrative effort to contest insurance denials, appealing decisions through documentation, alternative coding, or off-label justification, labor that became embedded in clinical routines but was neither trained nor compensated. The non-obvious implication is that insurers’ cost-control mechanisms unintentionally redistributed clinical work from treatment delivery to bureaucratic advocacy, transforming physicians into de facto claims negotiators.
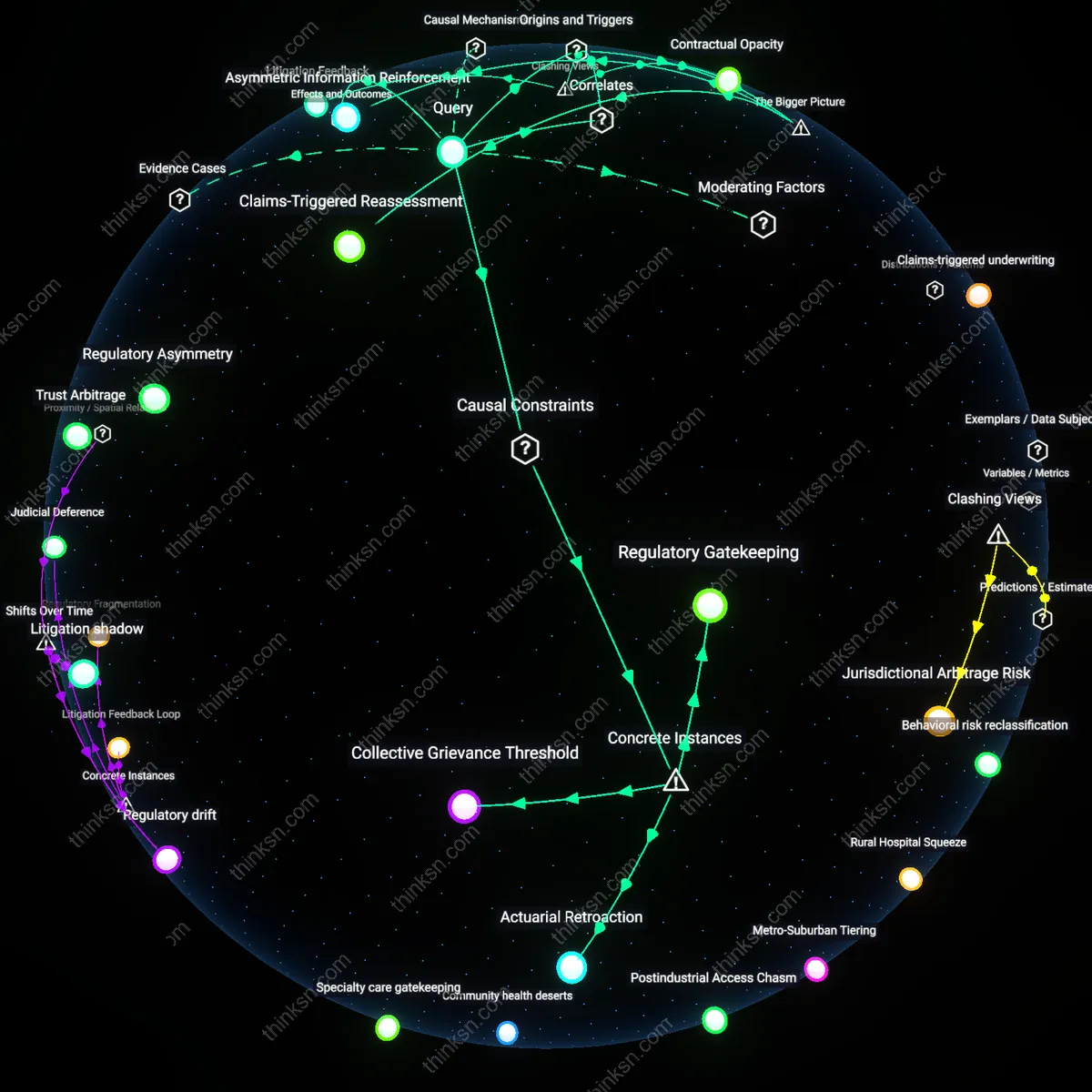
Precedent Cascades
Workaround strategies evolved from isolated improvisations in the early 2000s into standardized institutional protocols as repeated denials created patterned responses across peer networks, especially in academic medical centers facing similar payer pushback. Physicians began sharing successful appeal templates, diagnostic recodings, and timing tactics through informal departmental briefings and provider-only forums, turning individual ingenuity into collective procedural knowledge. This diffusion was sustained not by policy change but by repetition under predictable constraints—revealing how systemic friction, rather than innovation mandates, canalizes adaptive behavior across decentralized actors.
Clinical Bypass Design
As pharmaceutical benefit managers intensified step therapy requirements post-2010, doctors in specialties like rheumatology and dermatology began proactively structuring treatment plans to preempt insurance barriers—such as prescribing higher-cost biologics immediately with preemptive letters of medical necessity or exploiting diagnostic loopholes to qualify patients for faster approval tracks. These strategies reflect a shift from reactive appeals to anticipatory system evasion, where clinical decisions are calibrated not to disease progression alone but to the logic of payer algorithms. The underappreciated insight is that clinicians have become stealth system designers, reverse-engineering insurance rules to build treatment pathways that appear compliant while subverting their intent.
Formulary arbitrage
In the early 2000s, oncologists at MD Anderson Cancer Center systematically prescribed off-label, non-formulary drugs with similar efficacy profiles to guideline-recommended treatments to bypass prior authorization hurdles imposed by private insurers, exploiting a loophole in reimbursement rules that covered off-label use for cancer therapies; this demonstrated a shift from direct adherence to clinical guidelines toward strategic navigation of insurance formularies, revealing that therapeutic equivalence could be leveraged not for clinical but administrative advantage.
Pre-authorization templating
By 2010, primary care physicians in community health clinics in Cook County, Illinois, had developed standardized, evidence-heavy referral templates—co-created with social workers and pharmacy staff—to preemptively satisfy common insurer requirements for statin or diabetes medication approvals, significantly reducing appeal wait times; this institutionalization of bureaucratic labor into clinical workflows illustrates how decentralized providers collectively innovated reproducible administrative tools to compress the delay between diagnosis and treatment access.
Therapeutic substitution cascades
In 2016, cardiologists at the Cleveland Clinic began adopting a tiered prescribing sequence for PCSK9 inhibitors, starting with lower-cost biosimilars and escalating only after structured denials were documented, thereby using repeated, predictable insurance rejections to trigger automatic step therapy exemptions; this deliberate sequencing transformed payer resistance into a procedural asset, showing how systematic failure could be weaponized to accelerate access to high-barrier therapies within rigid coverage frameworks.
Prescription bargaining
Doctors began negotiating treatment approvals through informal letter-writing campaigns with insurers in the 1990s, using clinical justifications tailored to individual patients to bypass preauthorization barriers. This practice emerged as HMOs expanded and formularies restricted access, compelling physicians—especially in oncology and psychiatry—to act as advocates who mastered bureaucratic language rather than simply applying clinical guidelines. The non-obvious significance is that this did not erode professional authority but instead relocated it into the administrative domain, where medical legitimacy became a tool for procedural override rather than clinical decision-making.
Clinical workarounds
From 2010 onward, especially in chronic disease management, physicians increasingly leveraged diagnostic coding flexibility—such as upcoding severity or comorbidities—to justify guideline-recommended drugs under restrictive plans, effectively gaming risk-adjustment systems to gain formulary exceptions. This adaptation emerged alongside value-based care models that tied reimbursement to outcomes, pressuring providers to achieve results while constrained by access barriers. The significance lies in the quiet normalization of strategic misrepresentation not as fraud but as a tacitly accepted clinical survival tactic, revealing a structural misalignment between quality metrics and access mechanisms.
Prior Authorization Loophole
Doctors increasingly submitted modified diagnoses to bypass insurance denials for guideline-backed treatments. This workaround emerged directly from the rise of prior authorization requirements, where physicians—under pressure to adhere to clinical guidelines while navigating formulary restrictions—routinely adapted patient documentation to align with covered indications. The mechanism relies on systematic diagnostic recoding within electronic health records, often coordinated by clinic staff trained in payer-specific approval patterns, turning clinical narratives into negotiable assets rather than factual reports. What’s underappreciated is that this practice became normalized not as rogue behavior but as a de facto standard of care, revealing how insurance barriers reshaped medical documentation ethics in routine practice.
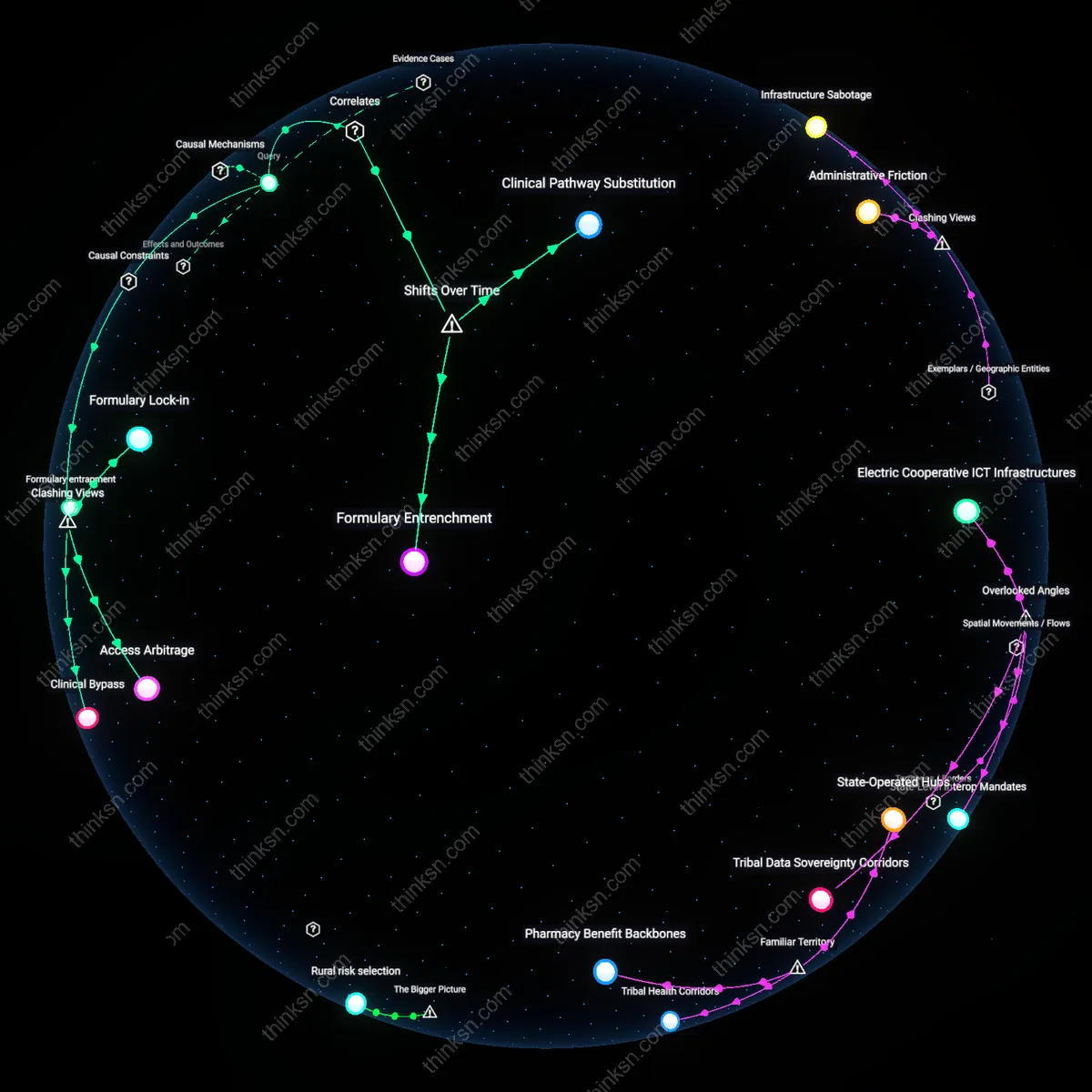
Guideline Arbitrage
Physicians began selectively citing different clinical guidelines depending on which ones aligned with insurer-approved treatment pathways. As insurance companies began referencing specific guideline versions to justify coverage decisions, medical teams learned to match their treatment justifications to the insurer’s preferred sources, regardless of emerging evidence. This operates through institutional formulary committees and prescribing protocols that privilege regulatory compliance over real-time guideline updates, creating a split between locally accepted standards and national recommendations. The non-obvious insight is that doctors didn’t abandon guidelines—they weaponized pluralism in guideline existence to exploit inconsistencies across systems, turning evidentiary consensus into a negotiable currency.
Compliance Theater
Medical teams started designing treatment initiation rituals that mimicked adherence to step therapy mandates, even when bypassing them through appeals or drug samples. As insurers enforced step therapy—requiring patients to fail cheaper, non-preferred drugs before approving guideline-endorsed ones—clinicians developed choreographed sequences where patients briefly started disfavored drugs, often with prewritten appeal letters ready before the first dose. This functions through coordinated timing between pharmacies, nurses, and billing staff, transforming treatment journeys into performative sequences that satisfy audit trails without altering outcomes. The underappreciated reality is that this theatrical compliance became a shared, unspoken norm, where legitimacy matters more than authenticity in proving medical necessity.
Formulary Substitution Logs
Hospital pharmacy departments began maintaining informal logs of insurance-denied medications and their approved alternatives starting in the late 1990s, enabling doctors to rapidly match patients with pre-vetted, insurer-accepted substitutes that mimicked guideline protocols. These internal records, often handwritten or embedded in local EHR templates, functioned as covert knowledge repositories that bypassed formal prior authorization systems by anticipating payer restrictions before prescriptions were written. The non-obvious significance lies in how these mundane administrative artifacts — overlooked in policy analyses focused on clinical guidelines or appeals processes — became institutional memory for workaround strategies, effectively decentralizing treatment adaptation into the pharmacy workflow rather than the physician’s decision point.
Pharmaceutical Sample Diversion
As insurance gatekeeping tightened in the early 2000s, clinics in underserved areas increasingly repurposed drug manufacturers’ free sample programs to deliver guideline-recommended biologics and specialty medications to patients who otherwise could not afford out-of-pocket costs or navigate prior authorization. Sales representatives, clinic staff, and even patient navigators colluded informally to allocate samples based on clinical need rather than promotional intent, transforming a marketing mechanism into a de facto safety net. This shadow distribution system is rarely acknowledged in health services research because it operates outside billing and prescribing records, yet it sustained access to high-cost therapies where insurance barriers were most severe, revealing how commercial supply chains were co-opted for equity-driven workarounds.
Diagnostic Code Stretching
Primary care physicians in private practices began subtly altering diagnostic coding — such as listing hypertension with 'acute end-organ damage' or depression with 'psychotic features' — to meet insurance criteria for faster approval of guideline-recommended drugs that required stricter indications. This tacit escalation, documented in internal billing training memos and informal provider huddles from the mid-2000s onward, exploited payer rulebooks’ hierarchical prioritization of certain diagnoses without overt fraud. The overlooked dimension is that clinical documentation itself became a strategic medium for resistance, where semantic precision was weaponized not for billing maximization but to reverse-engineer access — shifting the locus of workaround from treatment selection to pre-submission narrative framing.