Should You Reject Moderate-Risk BRCA Mastectomy Advice?
Analysis reveals 6 key thematic connections.
Key Findings
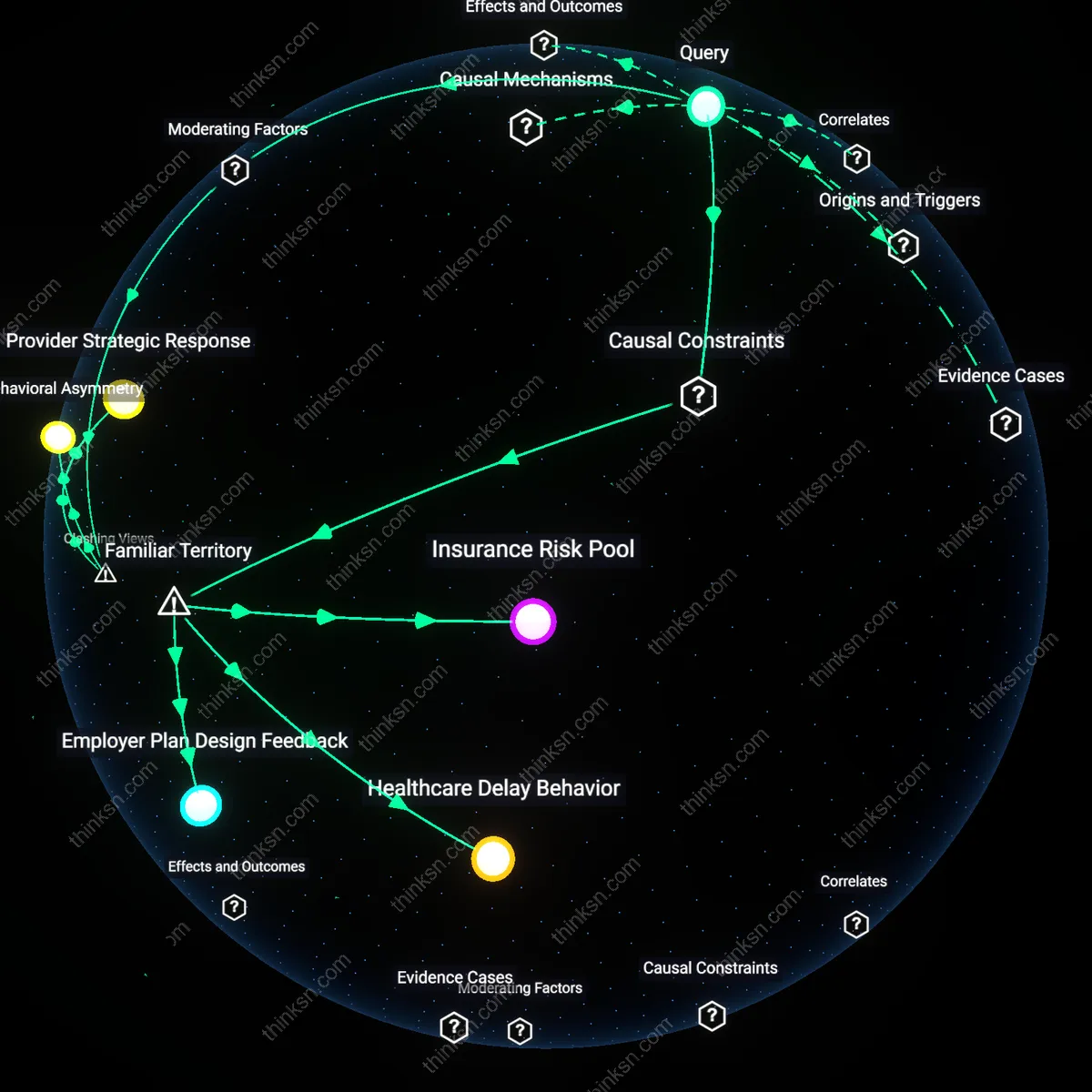
Clinical Ambiguity Exploitation
It is reasonable to refuse a prophylactic mastectomy because healthcare systems incentivize risk-averse interventions even when evidence is equivocal, pressuring patients toward irreversible procedures to hedge against malpractice liability. Hospitals and providers in high-income countries often emphasize interventionist protocols to mitigate litigation risks, particularly in oncology, where under-treatment is more scrutinized than over-treatment. This creates a structural bias where moderate-risk variants are managed as high-risk conditions, not solely due to medical urgency but due to systemic risk displacement—patients bear the physical and psychological costs of overtreatment while institutions reduce legal exposure. The non-obvious consequence is that medical uncertainty becomes a lever for institutional self-protection, not patient protection.
Genomic Identity Formation
It is reasonable to refuse a prophylactic mastectomy because individuals from hereditary cancer communities often reject surgical intervention as incompatible with their lived identity, particularly when genetic risk lacks phenotypic expression. Women with moderate-risk BRCA variants but no family history of aggressive cancer may perceive their bodies as healthy, not pre-pathological, and thus resist medical framing that equates genetic potential with disease inevitability. This reflects a bottom-up redefinition of genomic risk as a probabilistic narrative rather than a deterministic sentence, shaped by peer networks, online advocacy groups like FORCE, and reproductive autonomy movements. The underappreciated dynamic is that medical resistance becomes an act of identity preservation, not denial, within emerging cultures of genetic self-determination.
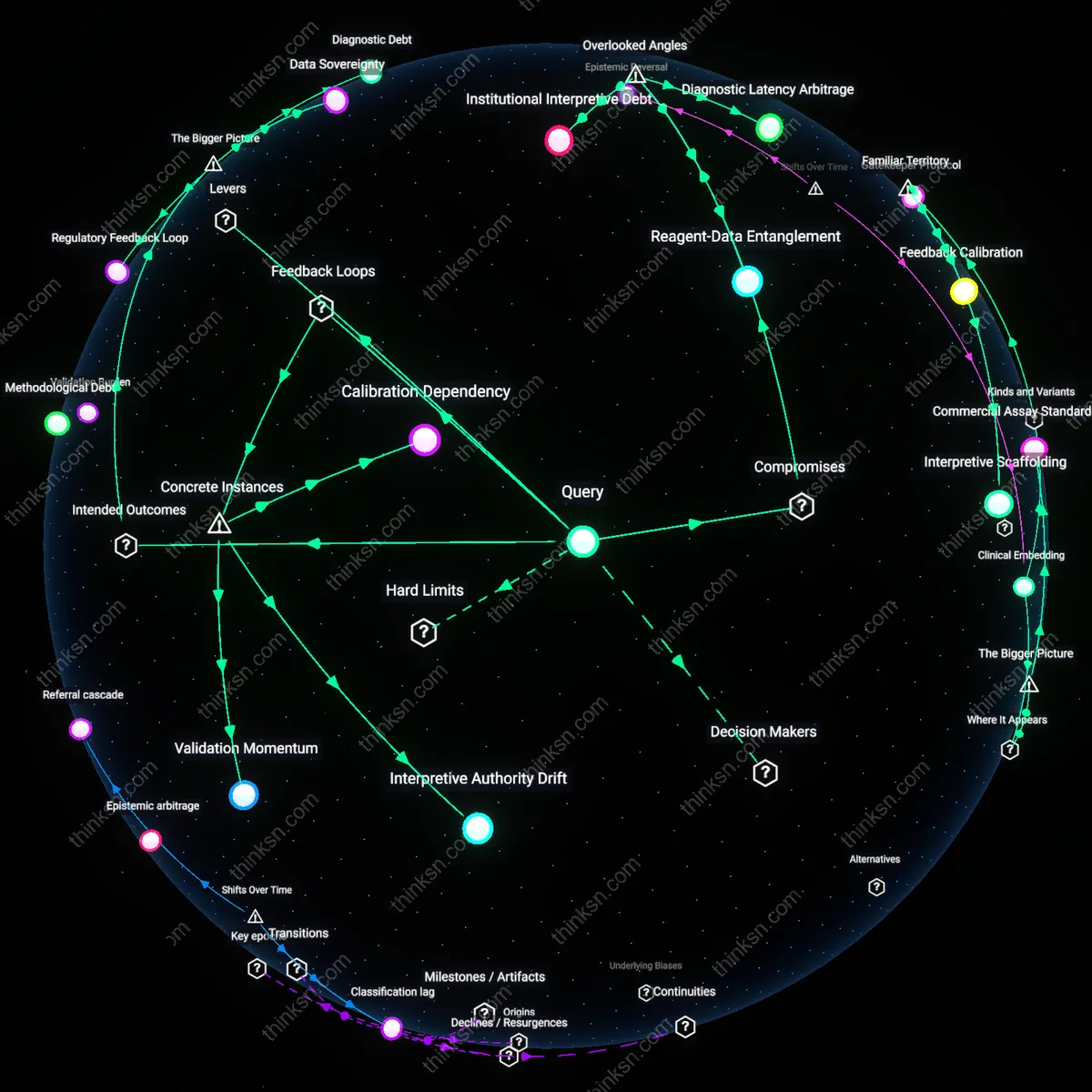
Evidence Asymmetry Regime
It is reasonable to refuse a prophylactic mastectomy because clinical guidelines rely on data generated from high-penetrance BRCA mutations, creating an evidentiary gap that systematically misrepresents moderate-risk variants as clinically equivalent. Regulatory bodies like the FDA and advisory panels such as NCCN extrapolate intervention thresholds from populations with 60–80% lifetime cancer risk, applying them to variants with 20–30% penetrance due to insufficient cohort studies and commercial pressure to deploy genetic testing at scale. This produces a regime where medical authority is maintained through generalization rather than precision, privileging actionable signals over contextual validity. The overlooked mechanism is that knowledge production lags behind technological application, making refusal a rational response to institutional epistemic debt.
Biological citizenship debt
It is damaging to refuse prophylactic mastectomy when a moderate-risk BRCA variant is detected because the refusal becomes encoded as a liability within insurance and biobank governance systems, which retroactively reclassify non-intervention as behavioral noncompliance, not medical equipoise. Population genomics databases operated by entities like the UK Biobank or Kaiser Permanente attribute variant penetrance in part from real-world clinical decisions, and when patients decline surgery, their subsequent outcomes are increasingly used to calibrate risk algorithms that then penalize future patients with similar variants who face higher premium costs or denied coverage—effectively punishing medical uncertainty as negligence. This mechanism remains hidden because risk modeling is treated as statistically neutral, while in fact it embeds normative assumptions about intervention thresholds, converting personal medical ambivalence into systemic financial and diagnostic penalties across generations. The non-obvious shift is that patient choice becomes data that retroactively alters disease definitions and entitlements, a form of long-term biological citizenship debt.
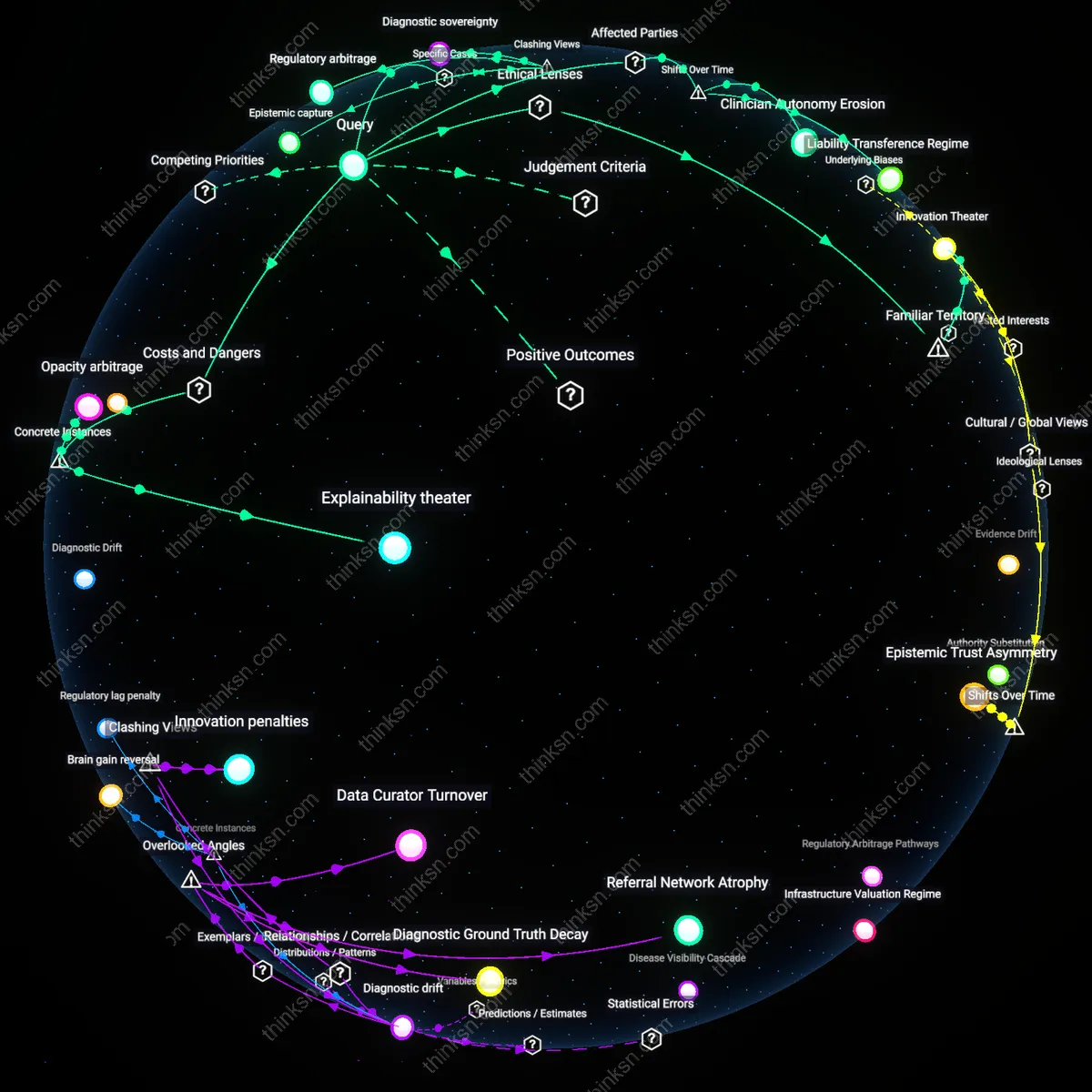
Somatic surveillance drag
Refusing prophylactic mastectomy under conditions of inconclusive evidence generates unintended systemic risk by increasing reliance on high-frequency MRI and ultrasound surveillance, which in turn amplifies radiological workload and image interpretation backlog across public health systems like the NHS or Canada’s provincial networks. This creates a hidden performance tax on radiologists, who must now distinguish subtle, recurrent artifacts in dense breast tissue across serial scans, elevating false-positive callbacks and downstream biopsy rates—procedures that collectively expose patients to greater cumulative radiation and procedural trauma than the surgery would have entailed. The overlooked dynamic is that surveillance is not a passive alternative but an active generator of clinical friction and iatrogenic burden, producing a phenomenon of somatic surveillance drag that erodes long-term adherence and increases systemic diagnostic error rates even for non-carriers. Most risk discussions assume surveillance is risk-free monitoring, but it actually redistributes danger into the temporal domain, where cumulative exposure and interpretive fatigue degrade safety over time.
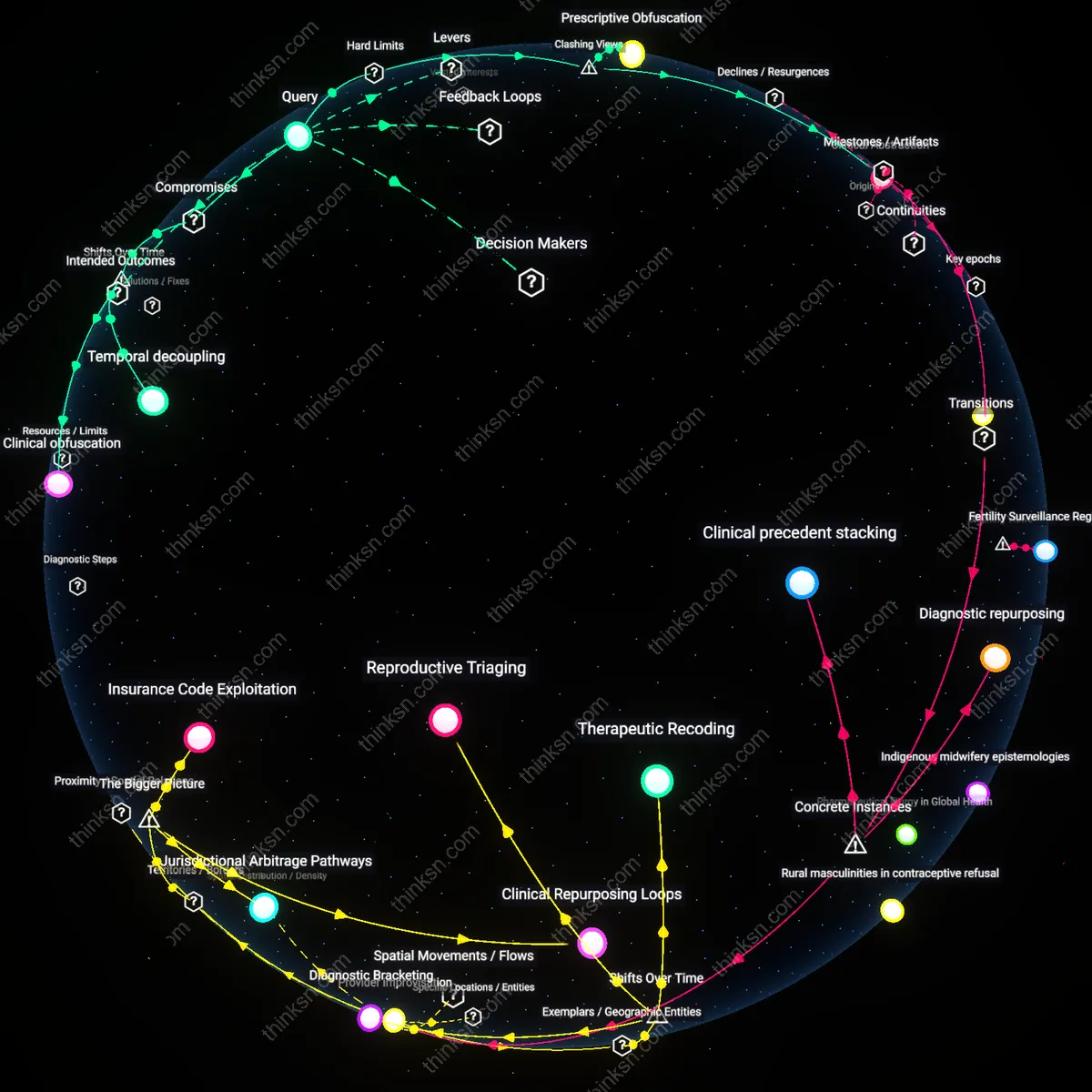
Variant moralization cascade
Declining mastectomy in the face of ambiguous BRCA data risks triggering a variant moralization cascade, wherein the medical and peer communities implicitly recode the genetic variant from a probabilistic marker into a moral litmus test for responsible health behavior. In clinical networks such as those governed by NCI-designated cancer centers, repeated patient refusals begin to shift institutional discourse, leading providers to unconsciously assign greater suspicion to patients with the same variant—interpreting anxiety, ambivalence, or cultural hesitation as negligence—which then filters into electronic health record narrative tags and referral patterns, ultimately affecting access to fertility services, clinical trials, or mental health support. The underappreciated mechanism is that uncertain genotypes become socially weaponized not through policy but through clinical micro-judgments, creating a hidden pathway where genetic ambiguity is resolved not by evidence but by normative enforcement. This alters the standard understanding of patient autonomy, revealing it as contingent on conformity with emerging therapeutic orthodoxies.