Cultural Co-Sleeping vs. AAP Infant Sleep Guidelines: A Rational Debate?
Analysis reveals 4 key thematic connections.
Key Findings
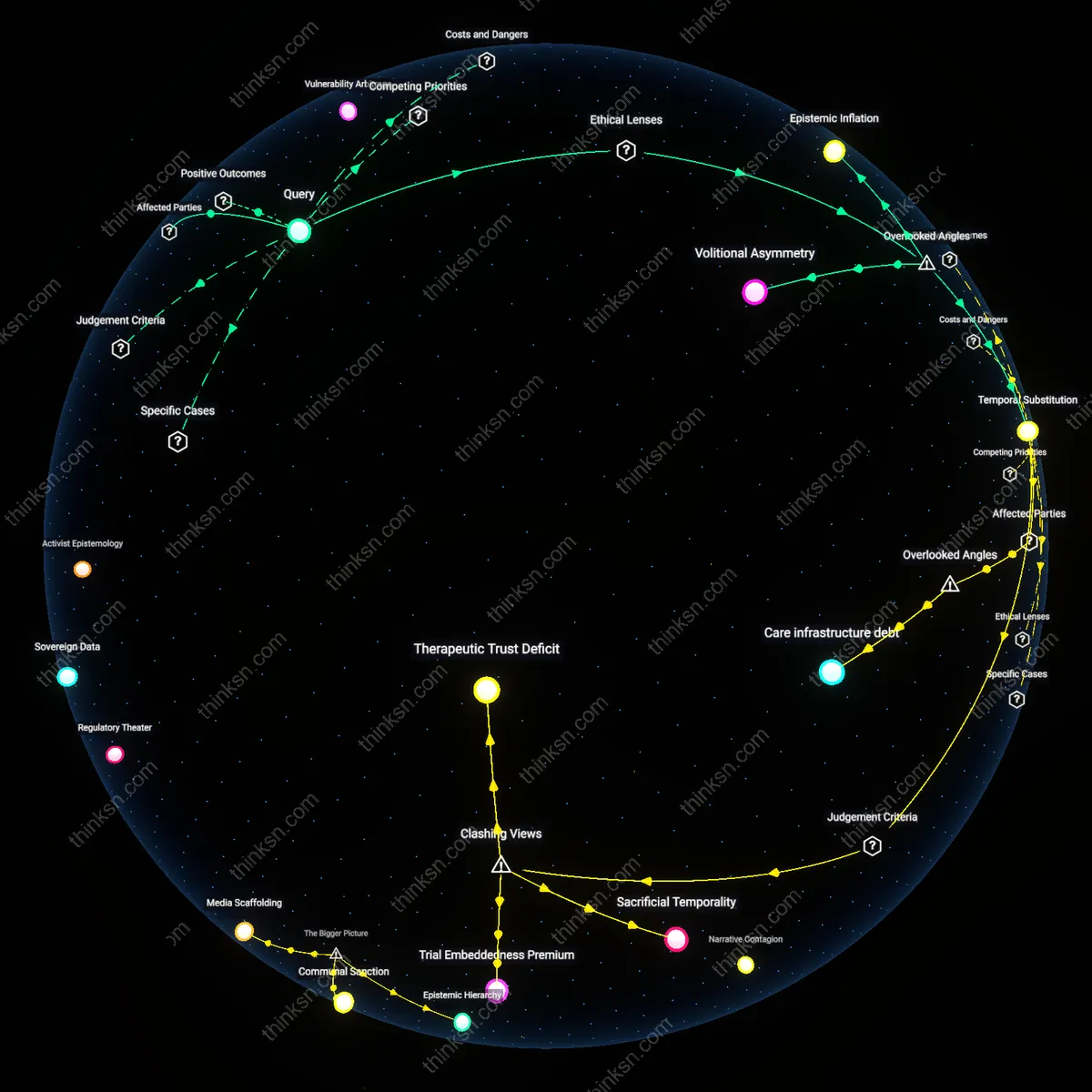
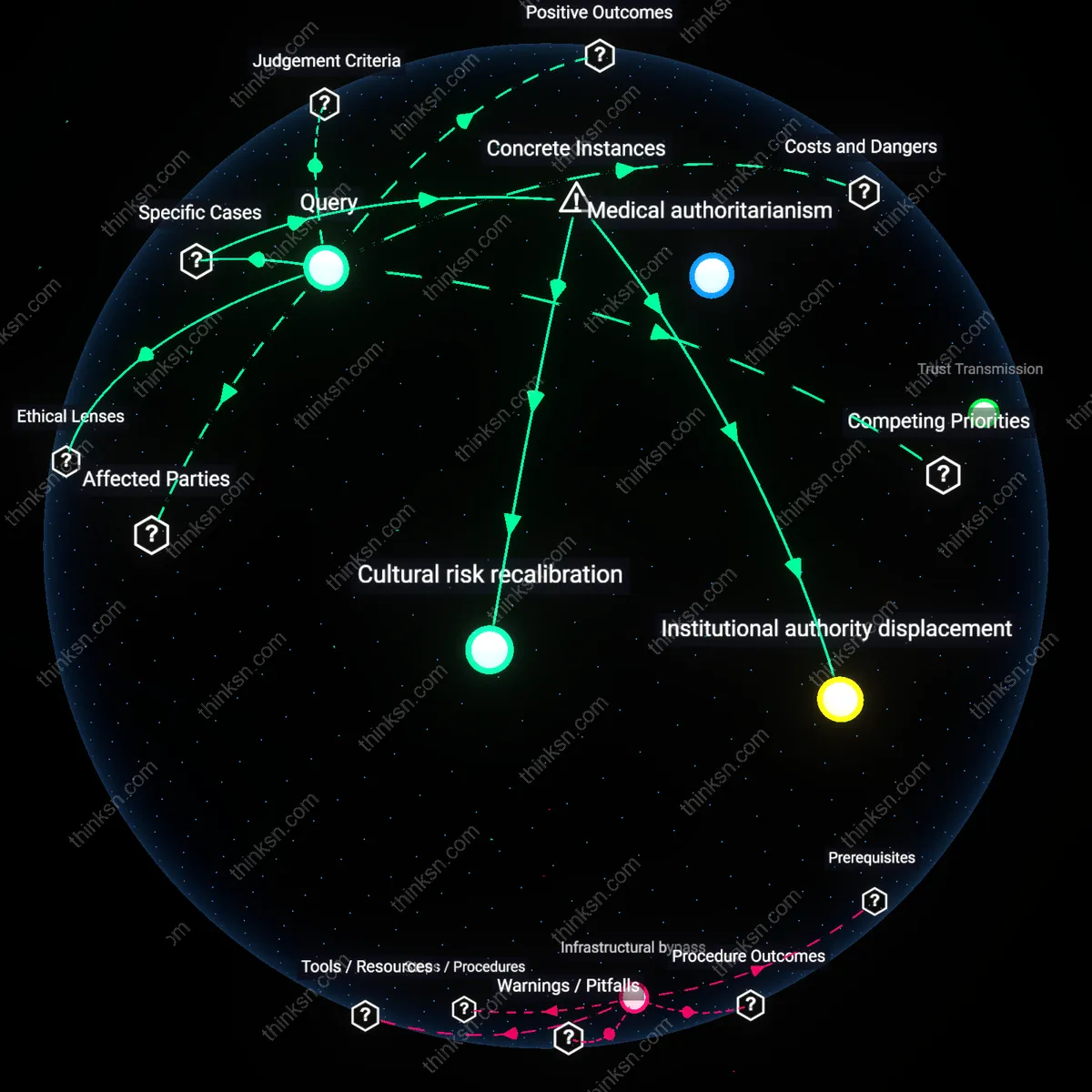
Medical authoritarianism
It is irrational to prioritize medical guidelines over cultural traditions regarding infant sleep practices when doing so erases epistemic sovereignty of marginalized communities. Public health institutions, operating through biomedical hegemony, position randomized clinical trials as the sole legitimate source of truth, dismissing centuries of embodied knowledge from Indigenous and diasporic care networks—such as co-sleeping practices among Māori or Hmong families—despite evidence of their efficacy in strengthening familial bonds and infant regulation. This erasure constitutes a form of structural violence that privileges white, Western scientific rationality over pluralistic ways of knowing, thereby reproducing colonial hierarchies under the guise of safety. The non-obvious consequence is not improved outcomes universally, but the pathologization of cultural continuity.
Risk anthropology
It is rational to prioritize medical guidelines when their recommendations reduce population-level infant mortality, regardless of cultural alignment. In high-income countries such as the United States, the Back to Sleep campaign—enforced through pediatric consensus and institutional accountability—drove a 40% decline in SIDS rates after 1994 by standardizing supine sleep positioning, directly challenging cultural norms favoring side or prone sleeping across Black, immigrant, and rural communities. The mechanism operates through evidence-based utilitarianism, where aggregate reduction in harm overrides individualized tradition, particularly when those traditions correlate with elevated risk. The non-obvious insight is that cultural resistance may reflect not principled epistemology, but entrenched social habits disproportionately maintained in the absence of effective interpersonal dissemination.
Institutional authority displacement
The American Academy of Pediatrics' 'Back to Sleep' campaign rationalized shifting infant sleep positioning by overriding widespread parental customs through clinical epidemiology—specifically, its 1992 recommendation that infants sleep supine dramatically reduced SIDS rates across diverse cultural groups in the U.S., including African American and rural white communities where prone sleeping was entrenched, demonstrating that medically validated protocols can ethically displace tradition when institutional credibility and mortality data converge. This shift succeeded not merely through education, but by leveraging pediatricians as trusted gatekeepers in a decentralized healthcare system, where guideline adherence depended on localized clinician authority rather than state mandate. The underappreciated mechanism here is not resistance or compliance, but the reconfiguration of parental trust from kinship networks to medical institutions as the primary source of infant-care legitimacy.
Cultural risk recalibration
In Japan, co-sleeping has long been the normative infant care practice rooted in familial interdependence and space constraints, yet despite initially low SIDS rates, rising pediatric surveillance revealed increases in accidental suffocation linked to adult bedding—this prompted the Japanese Ministry of Health to adapt Western crib-based guidelines without outright rejection of bed-sharing, instead promoting 'room-sharing without bed-sharing' as a hybrid practice, effectively recalibrating traditional behavior through selective integration of medical advice. The key mechanism was not imposition but reinterpretation, where public health officials collaborated with community midwives to preserve cultural continuity while reducing risk, revealing that rational prioritization occurs most effectively when medical guidelines are not universalized but contextually translated. The overlooked insight is that rationality in this domain depends not on superiority of science over tradition, but on the capacity of health systems to perform cultural syntaxing—retaining symbolic forms while altering dangerous substrates.