Do HR Departments Prioritize Risk Over Rights in Healthcare?
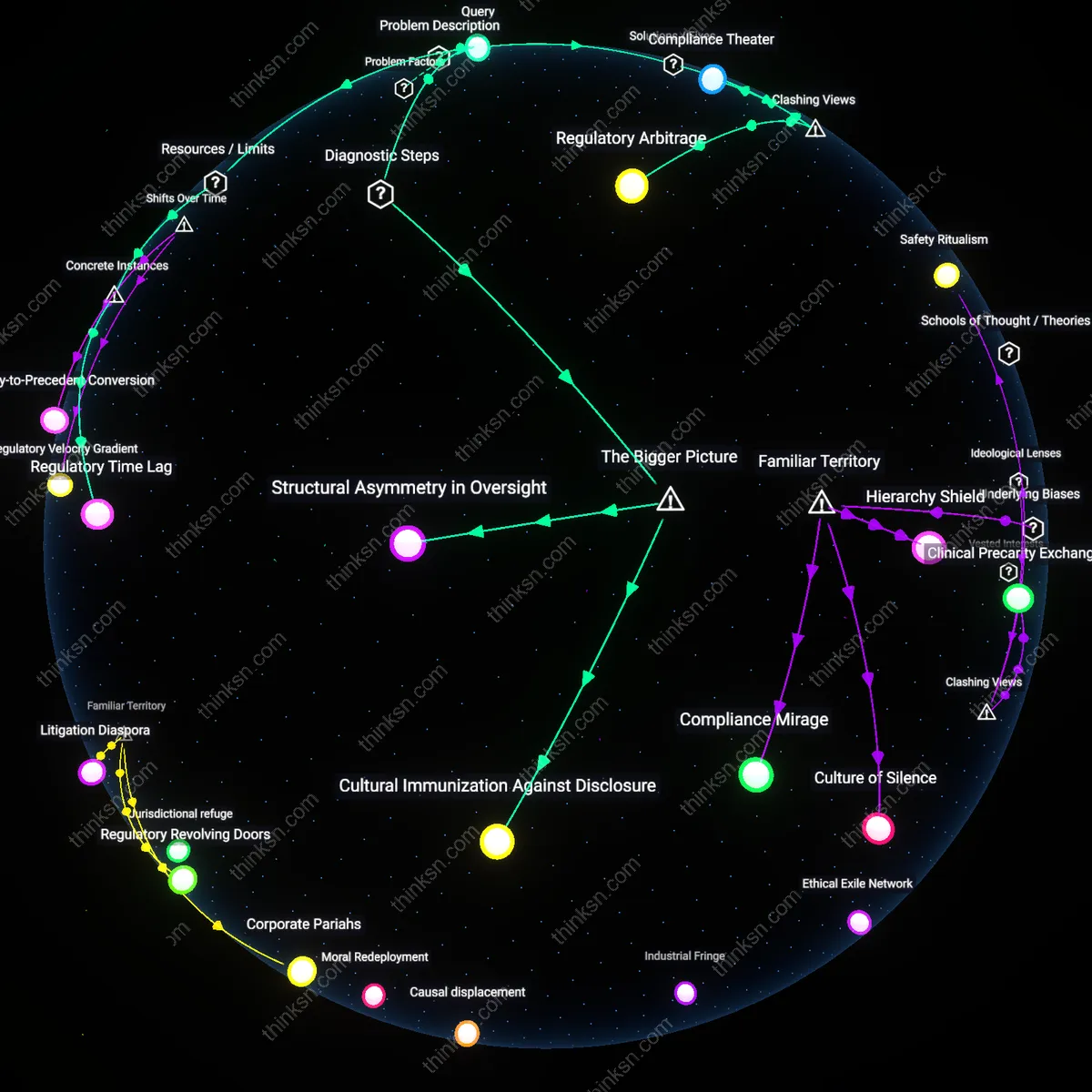
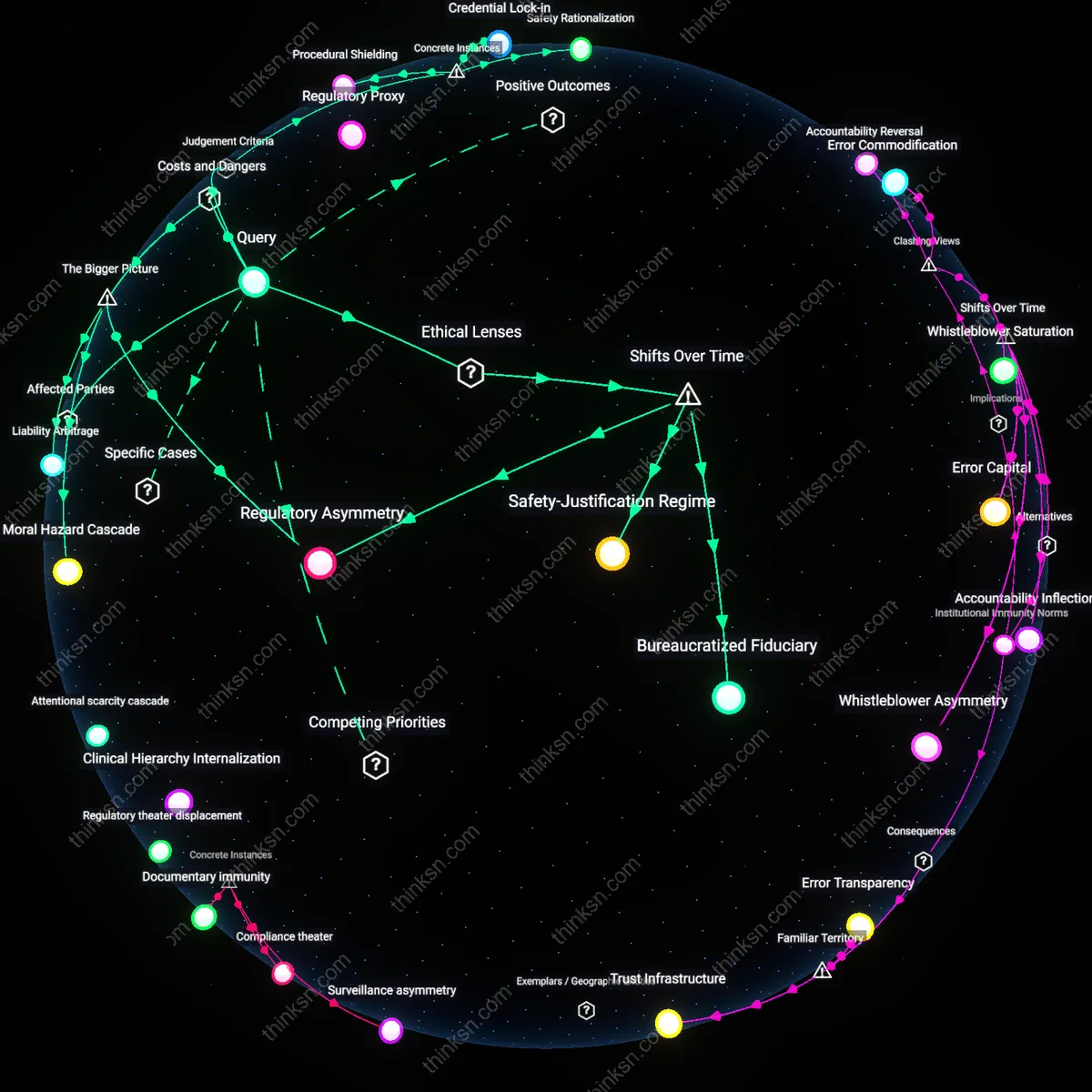
Analysis reveals 11 key thematic connections.
Key Findings
Moral Inversion
HR departments in healthcare settings prioritize employee rights only when they align with patient safety narratives, thereby weaponizing ethical discourse to suppress dissent. Compliance officers, clinical supervisors, and institutional risk managers exploit the sanctity of patient outcomes to reframe labor grievances—such as whistleblowing or workload complaints—as veiled threats to care quality, thus justifying punitive actions under the guise of protection. This mechanism operates through accreditation standards and incident reporting systems that formally require employee accountability while offering no reciprocal redress, revealing how moral imperatives can be inverted to consolidate administrative control. The non-obvious insight is that patient safety, rather than mitigating power imbalances, becomes the very logic through which employee subordination is ethically legitimized.
Regulatory Proxy
HR departments outsource ethical justification to external regulators, making Joint Commission audits and CMS compliance the de facto arbiters of employee treatment in hospitals. Hospital administrators, legal counsel, and chief compliance officers treat regulatory thresholds as upper bounds of moral obligation, constraining HR decisions within risk-minimization protocols that preemptively sacrifice employee advocacy to avoid citation or funding loss. This dynamic functions through a system where real-time labor conflicts are deferred to post-hoc audit readiness, revealing that organizational risk is not inherently prioritized over employee rights, but that both are subordinated to a performative alignment with external oversight. The dissonance lies in the fact that HR does not act from internal bias but as a procedural conduit for regulatory capture—employee rights erode not from malice but from administrative deflection.
Clinical Hierarchy Internalization
Frontline healthcare workers, especially nurses and support staff, internalize clinical hierarchies to the extent that they preemptively legitimize HR decisions that compromise their own rights, interpreting managerial actions as necessary to preserve team cohesion and patient trust. This self-policing is enforced through unit-level culture shaped by physicians, charge nurses, and clinical educators who equate loyalty with silence, transforming structural inequities into personal moral failures. The dynamic operates through informal sanction systems—such as peer reporting and schedule manipulation—that precede and substitute formal HR intervention, meaning that power imbalance is reproduced not by HR policy but by the workforce’s own disciplinary practices. The overlooked reality is that employee rights are constrained not by HR overreach, but by the deep socialization of healthcare labor into accepting subordination as professional virtue.
Procedural Shielding
HR departments at King's College Hospital NHS Foundation Trust prioritized organizational liability mitigation over whistleblower protections after the 2017 Letby scandal, deploying formal grievance procedures to defer and contain internal complaints about nurse Lucy Letby despite repeated clinical staff warnings, thereby activating bureaucratic protocol as a mechanism to insulate institutional authority; this reveals how procedural compliance becomes a tool not for fairness but for deflection, where adherence to process substitutes for substantive justice, masking power asymmetries under the guise of due process.
Safety Rationalization
In the aftermath of the 2010 Virginia Mason Medical Center patient safety initiative, HR institutionalized mandatory incident reporting with punitive review boards that recast employee errors as systemic risks, shifting focus from support for frontline workers to data-driven risk profiling; this redefinition of 'safety' enabled management to justify disciplinary actions under the moral principle of patient paramountcy, illustrating how a legitimate ethical imperative—patient safety—can be functionally transmuted into a justification for surveillance and control, suppressing appeals to professional autonomy.
Credential Lock-in
During the 2021 staffing crisis at Ochsner Health System in Louisiana, HR enforced rigid privileging requirements that disqualified experienced nurses from adjacent specialties despite emergency staffing needs, citing regulatory compliance and malpractice exposure; by privileging formal credentials over demonstrated competence, HR protected the organization from legal risk but undermined employee mobility and professional discretion, exposing how the fixation on licensure as a legal safeguard creates a structural dependency on institutional validation, turning professional identity into a revocable franchise rather than an inherent right.
Regulatory Asymmetry
HR departments in healthcare settings prioritize organizational risk over employee rights because compliance with external regulators like The Joint Commission or CMS creates binding mandates that penalize institutions for patient safety failures but not for employee grievances. This regulatory asymmetry concentrates enforcement power on clinical outcomes, incentivizing HR to align policies with audit-ready risk mitigation rather than equitable labor practices. As a result, employee rights become discretionary in high-pressure environments like emergency departments, where the specter of decertification outweighs internal appeals. The non-obvious consequence is that HR functions not as a neutral mediator but as an institutional firewall, calibrated to absorb regulatory shocks while shielding clinical operations from labor challenges.
Moral Hazard Cascade
HR departments systematically deprioritize employee rights because patient safety concerns generate a moral hazard cascade in which clinical leaders implicitly tolerate overworked or under-supported staff, assuming worst-case outcomes are preventable through individual vigilance rather than structural reform. When adverse events occur, HR is pressured to contain reputational and legal fallout by managing staff behavior rather than addressing systemic flaws—such as nurse-to-patient ratios or trauma-informed supervision—thereby reinforcing a cycle where risk is individualized and punished. The underappreciated dynamic is that HR’s alignment with patient safety metrics inadvertently incentivizes the scapegoating of frontline workers, especially in public hospitals facing budget constraints and high litigation exposure, transforming employee protections into expendable costs.
Liability Arbitrage
HR departments in healthcare settings favor organizational risk containment because liability arbitrage allows institutions to shift legal and financial burdens onto employees when patient harm occurs, especially in malpractice-prone specialties like obstetrics or psychiatry. By enforcing strict conduct policies and using employment contracts to limit recourse, HR enables organizations to present a unified front to insurers and courts, where disciplinary records and prior counseling are used to demonstrate 'due oversight' even when systemic failures are evident. This creates a downstream consequence in which HR’s role evolves into preemptive documentation of employee deficiencies—not to support development, but to build defensible legal archives—thus embedding power imbalance into routine administrative practice in ways invisible to accreditation bodies.
Bureaucratized Fiduciary
Beginning in the 1980s, the expansion of managed care under neoliberal health policy recast hospital administrators as fiduciaries of shareholder-like efficiency, embedding HR within cost-containment logics that subsume employee advocacy to financial and legal risk mitigation. As Medicare’s prospective payment system incentivized shorter stays and higher throughput, patient safety became entangled with staffing ratios and rapid disciplinary processes, positioning HR not as a mediator of rights but as an enforcer of operational continuity. This reconfiguration reveals that the erosion of employee rights is not a failure of ethics but a designed feature of a system where fiduciary duty has been transferred from care providers to institutional balance sheets.
Safety-Justification Regime
The post-9/11 securitization of public institutions, including hospitals, introduced emergency preparedness protocols that normalized surveillance and hierarchical control under the banner of public safety, a shift HR integrated into internal disciplinary cultures by the mid-2000s. Drawing on Carl Schmitt’s state-of-exception logic now embedded in hospital continuity-of-operations plans, HR departments gained discretionary power to suspend standard labor procedures during declared crises—powers retained during non-crisis periods through doctrines like ‘imminent risk’ under OSHA and CMS guidelines. What remains underappreciated is that patient safety is no longer merely a clinical standard but a sovereign justification enabling permanent exceptionality in employment relations.