Who Wins as Mental Health Diagnoses Shape Workplace Roles?
Analysis reveals 17 key thematic connections.
Key Findings
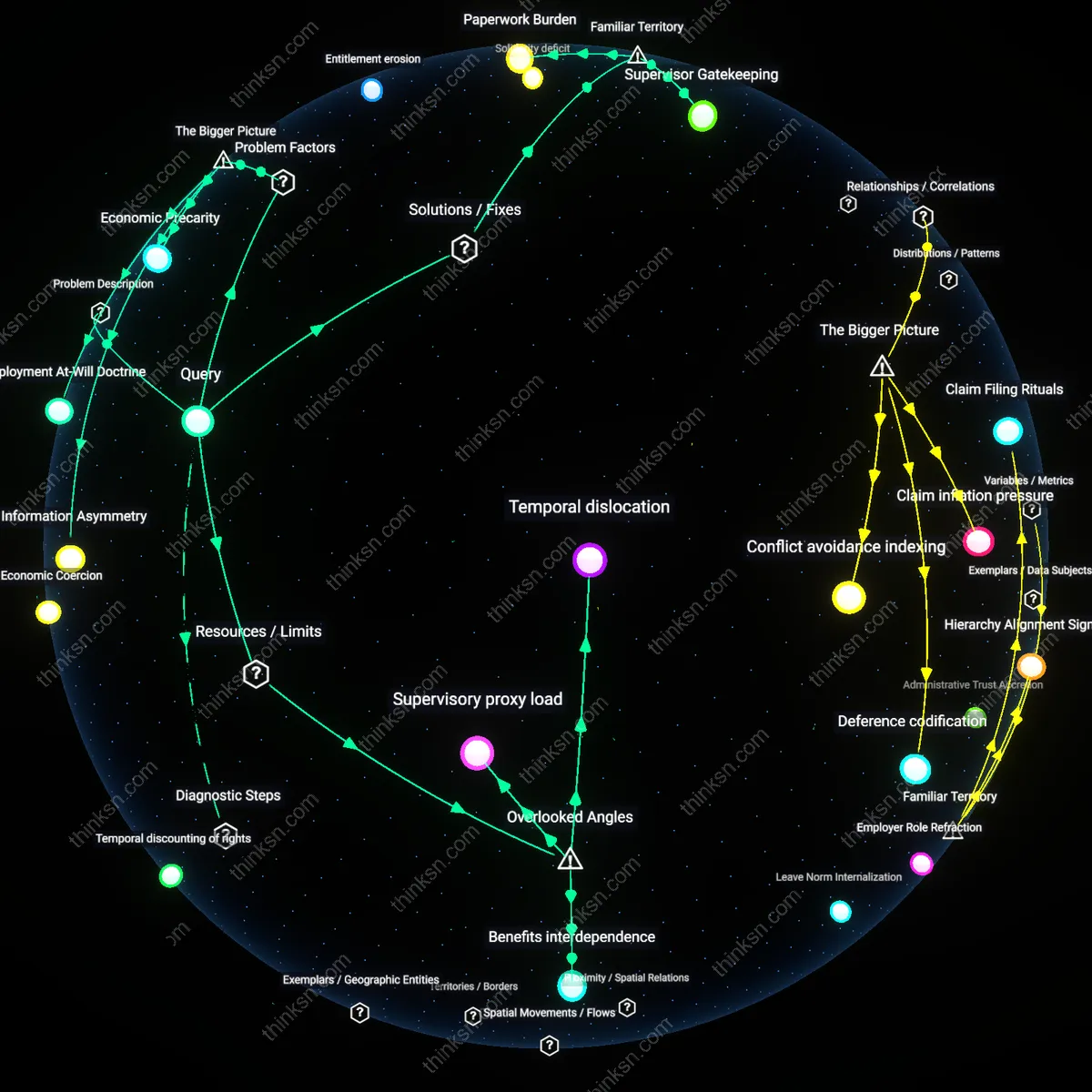
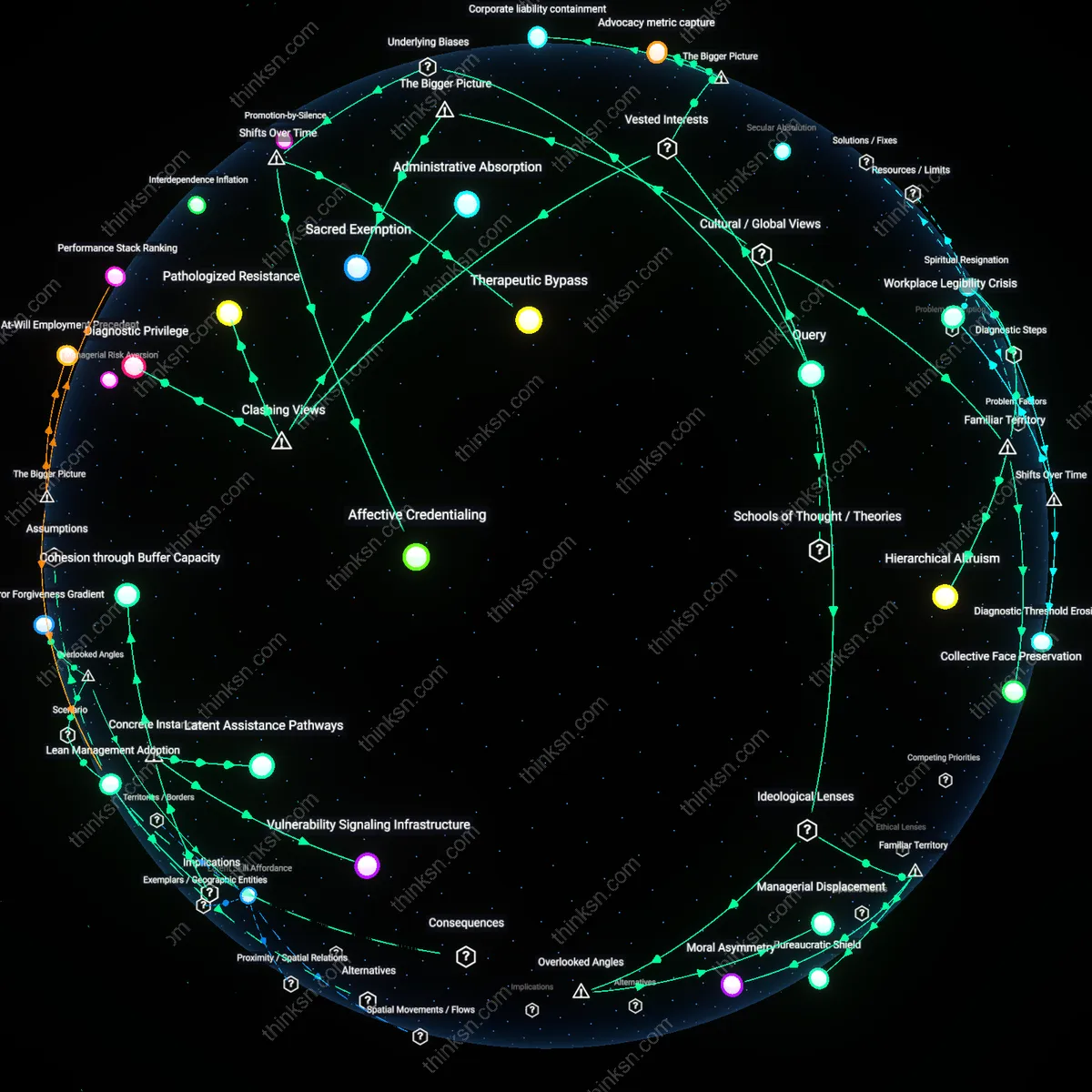
Managerial Displacement
From a conservative ideological standpoint, when diagnosed employees are reassigned or relieved of responsibilities, supervisors absorb displaced obligations or delegate them informally to non-diagnosed subordinates, creating a hidden workload sink that preserves organizational output without official restructuring; this occurs through the informal authority of team leads to redistribute tasks quietly, avoiding bureaucratic scrutiny. The overlooked dynamic is that this silent redistribution reinforces paternalistic supervision—where loyalty is rewarded with lighter loads and discretion—undermining meritocratic performance models and entrenching informal power networks that are rarely visible in HR audits or equity assessments.
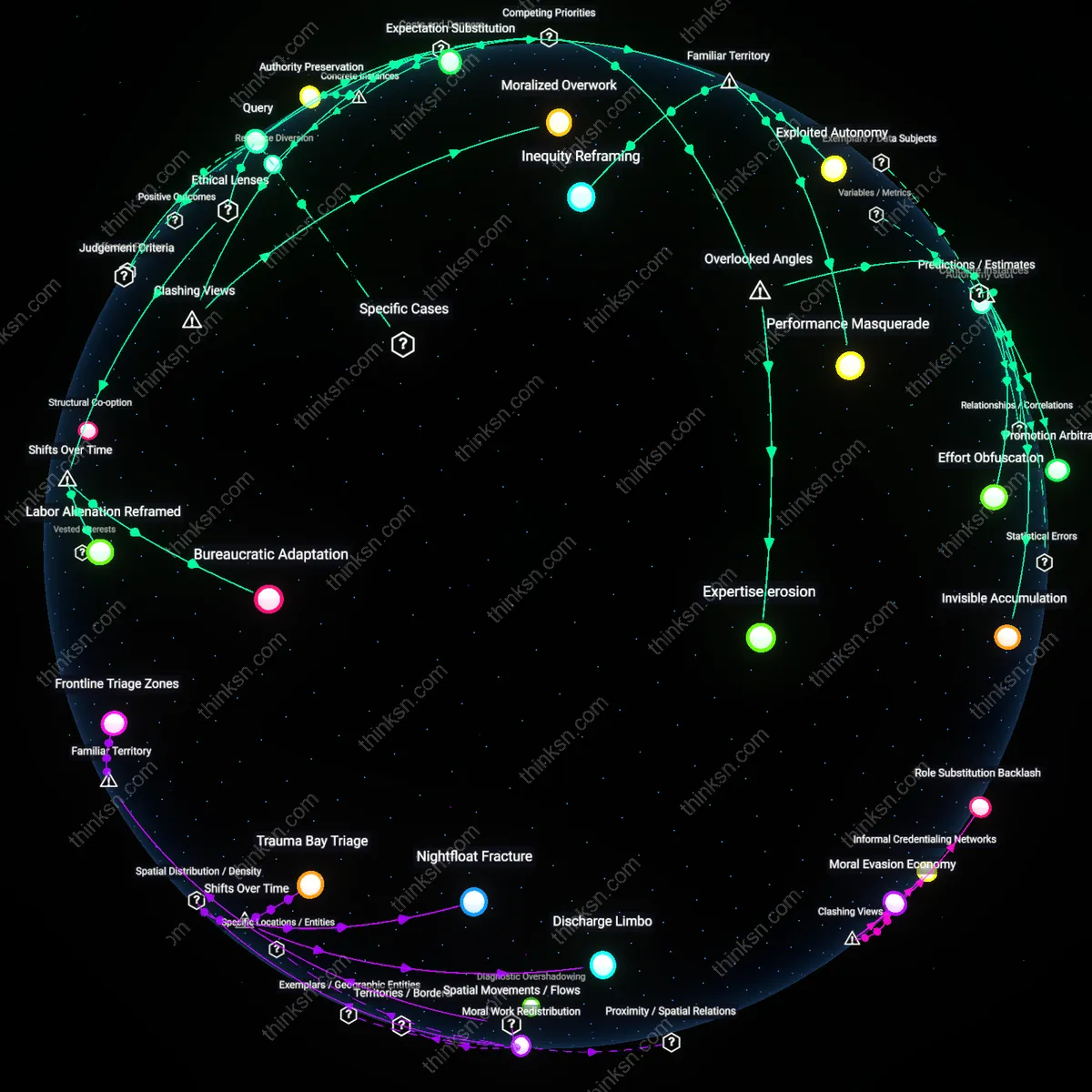
Affective Debt
Through a Marxist lens, when diagnostic accommodations reduce an individual’s labor output, the shortfall is socially absorbed by the labor collective through intensified effort from others, generating affective debt—an unpaid emotional and energetic surplus extracted from coworkers who compensate without recognition or compensation; this operates via workplace solidarity norms that stigmatize complaint when a colleague is 'suffering,' thus masking exploitation within care-oriented discourse. The critical but invisible aspect is that mental-health accommodations, while individually just, can function as mechanisms of labor extraction from the undiagnosed proletariat, reproducing capitalist efficiency through moralized overwork rather than direct coercion.
Medicalized Legitimacy
Workers who disclose mental-health diagnoses gain temporary protection from performance expectations by converting personal distress into clinically recognized conditions. This shift allows individuals to claim accommodations under disability frameworks like the ADA, which institutions are legally bound to honor, thereby reducing their exposure to disciplinary management practices. What’s underappreciated is that this legitimacy depends not on suffering per se, but on the ability to narrate it within medical idiom—privileging those with access to diagnosis and fluency in clinical discourse.
Bureaucratic Shield
Middle managers benefit from employees using mental-health diagnoses because it provides a depoliticized rationale to remove underperformers from high-pressure roles without triggering conflict or accusations of bias. By deferring to medical authority, supervisors can offload difficult personnel decisions to HR and occupational health systems, preserving team morale and managerial neutrality. The non-obvious consequence is that mental-health designations become administrative tools for smoothing labor friction, not just supports for recovery.
Moral Asymmetry
Conservative cultural institutions often frame mental-health accommodations as unjust advantages that reward weakness, thereby reinforcing hierarchies where endurance and self-reliance define worth. In such environments, those who invoke diagnoses are seen as undermining meritocratic ideals, which strengthens the moral authority of leaders who demand resilience. The overlooked effect is that the stigma around diagnosis becomes a power mechanism—used less to exclude individuals than to validate a particular ideology of discipline and control.
Hierarchical Altruism
Western corporate environments benefit managers when mental-health diagnoses lead to reduced job responsibilities, because structural flexibility is selectively granted to maintain team output while preserving positional authority; this operates through performance management systems that reassign tasks quietly rather than restructure formally, reinforcing the manager’s role as both gatekeeper and caretaker — a duality rarely questioned despite visibly unequal access to accommodation, which reveals how familiar narratives of workplace empathy serve hierarchical stability more than individual wellbeing.
Collective Face Preservation
In East Asian workplaces, family members and senior colleagues benefit when diagnoses reduce responsibilities because they avoid public stigma associated with individual underperformance, operating through implicit social contracts that prioritize group harmony over personal disclosure; this reliance on unspoken adjustment — such as redistributing work without formal recognition — underscores how widely recognized compassion for mental health still defers to ancestral norms of shame avoidance, making invisible labor the default cost of maintaining collective face.
Spiritual Resignation
In regions influenced by South Asian religious traditions like karma-based Hindu or Buddhist worldviews, employers benefit indirectly when diminished responsibilities follow mental-health labels because such outcomes align with culturally familiar notions of fate or personal duty, operating through passive acceptance rather than systemic change; this resonance between medical diagnosis and spiritual narrative allows organizations to retain control without active intervention, exposing how deeply intuitive beliefs in predestination can suppress demands for workplace equity under the guise of inner healing.
Sacred Exemption
In predominantly Muslim societies where religious duty shapes conceptions of productivity and obligation, invoking clinical mental illness to reduce work responsibilities risks moral disapproval unless reframed through spiritual frameworks such as *kafaāh* (personal capacity) or divine will, allowing religious authorities—and not medical professionals—to arbitrate legitimacy; this redirects power from occupational health departments to imams and family elders, transforming psychiatric claims into theological discernment. The condition enabling this shift is the institutionalized role of Islam in public life, particularly in countries like Indonesia or Egypt, where state-recognized fatwa councils influence labor norms, making mental distress legible only when consistent with religiously sanctioned vulnerability. As a result, Western-style diagnosis becomes a liability unless filtered through communal ethics of endurance and submission to God’s plan, which re-centers organizational authority in religious lineage rather than HR compliance protocols. The overlooked consequence is that secular mental-health advocacy can inadvertently marginalize believers by forcing them to choose between medical credibility and spiritual integrity—thus strengthening clerical gatekeeping. What makes this hold is the competition between transnational psychiatric discourse and localized religious epistemologies for defining human limits.
Therapeutic Bypass
Mental-health diagnoses have increasingly served clinicians and HR departments as tools to depoliticize workplace conflict by recasting structural grievances—over pay, autonomy, or exploitation—as individual psychological conditions requiring adjustment rather than systemic change, a transition that accelerated in the 2010s with the corporate adoption of wellness programs. This shift reframed employee resistance or burnout as symptoms to be managed medically, displacing union organizing or collective bargaining with therapy referrals and mindfulness apps. The underappreciated consequence is that professionals in psychology and human resources now act as intermediaries who stabilize hierarchies by redirecting dissent into private treatment, effectively using diagnosis to neutralize challenges to authority under the guise of support.
Affective Credentialing
Workers in knowledge-intensive sectors such as tech and academia benefit temporarily from using mental-health diagnoses to negotiate flexibility in performance expectations, a practice that emerged prominently in the late 2010s as burnout became widespread among highly educated, overtasked employees. This shift reflects a broader transition from industrial-era discipline—based on physical presence and time—to post-Fordist productivity regimes where output is measured through cognitive and emotional labor, making legitimacy for reduced responsibility contingent on possessing a medically recognized 'right to withdraw.' The overlooked dynamic is that only those with cultural capital and access to healthcare can successfully deploy diagnoses as credentials, thus converting psychological vulnerability into a rarefied form of leverage that reproduces inequality among workers while appearing to democratize care.
Corporate liability containment
Corporations benefit from power shifts when mental-health diagnoses reduce employee responsibilities because such diagnoses legally reframe diminished performance as a medical issue rather than managerial failure, shielding firms from accountability under employment law. This mechanism operates through the alignment of clinical categorization with risk management protocols in human resources, where documented diagnoses activate accommodations that limit grounds for disciplinary action. The non-obvious consequence is that companies gain a preemptive legal buffer by accepting reduced productivity, transforming psychological vulnerability into institutional insulation.
Therapeutic governance expansion
Governments benefit from power shifts tied to mental-health-based work adjustments because medicalized explanations for altered labor participation enable the delegation of social welfare functions to healthcare systems, reducing direct fiscal and administrative burdens on state programs. This occurs through the integration of psychiatric evaluation into workplace compliance frameworks, such as disability accommodations, which shifts responsibility from public policy solutions to individual treatment pathways. The underappreciated systemic effect is that state capacity is preserved not by intervention but by offloading governance onto clinical institutions.
Advocacy metric capture
Mental health advocacy groups benefit when diagnoses lead to reduced job duties because measurable workplace accommodations serve as quantifiable evidence of policy impact, enhancing their credibility with funders and legislators. This dynamic functions through the translation of personal outcomes into institutional metrics—such as accommodation rates or employer compliance—used to justify continued advocacy and resource allocation. The overlooked implication is that success becomes defined by individualized concessions rather than structural labor reform, reinforcing a system where visibility depends on managed impairment.
Diagnostic Privilege
Corporations benefit from mental-health diagnoses reducing employee responsibilities by using clinical justifications to depoliticize workforce attrition and suppress systemic critique, thereby preserving productivity norms without addressing structural workplace harm; this mechanism operates through HR departments and occupational health gatekeepers who validate medicalized exits over collective bargaining, revealing that corporate tolerance for diagnosis serves as a containment strategy rather than compassion—an underappreciated function where mental health labels become tools of labor neutralization rather than accommodation.
Pathologized Resistance
Activists who advocate for mental-health accommodations inadvertently reinforce employer power by legitimizing individualized, biomedical explanations for burnout, thereby displacing organizing around exploitative conditions into private therapeutic domains; this shift occurs through institutional funding channels that favor treatment-based advocacy over labor radicalism, exposing how well-intentioned support can erode collective agency—an overlooked consequence where therapy discourse becomes a silent partner in weakening workplace dissent.
Administrative Absorption
Government agencies benefit from diagnosing workers with mental health conditions because it relocates economic inactivity from the sphere of labor policy failure to individual health management, reducing pressure to reform precarious employment or expand social protections; this occurs through welfare systems that require clinical documentation before granting work exemptions, making state institutions complicit in medicalizing structural disengagement—a concealed dynamic where public policy uses diagnosis to absorb political risk under the guise of care.