When Is External Review Worth It for a Stressed Patient?
Analysis reveals 6 key thematic connections.
Key Findings
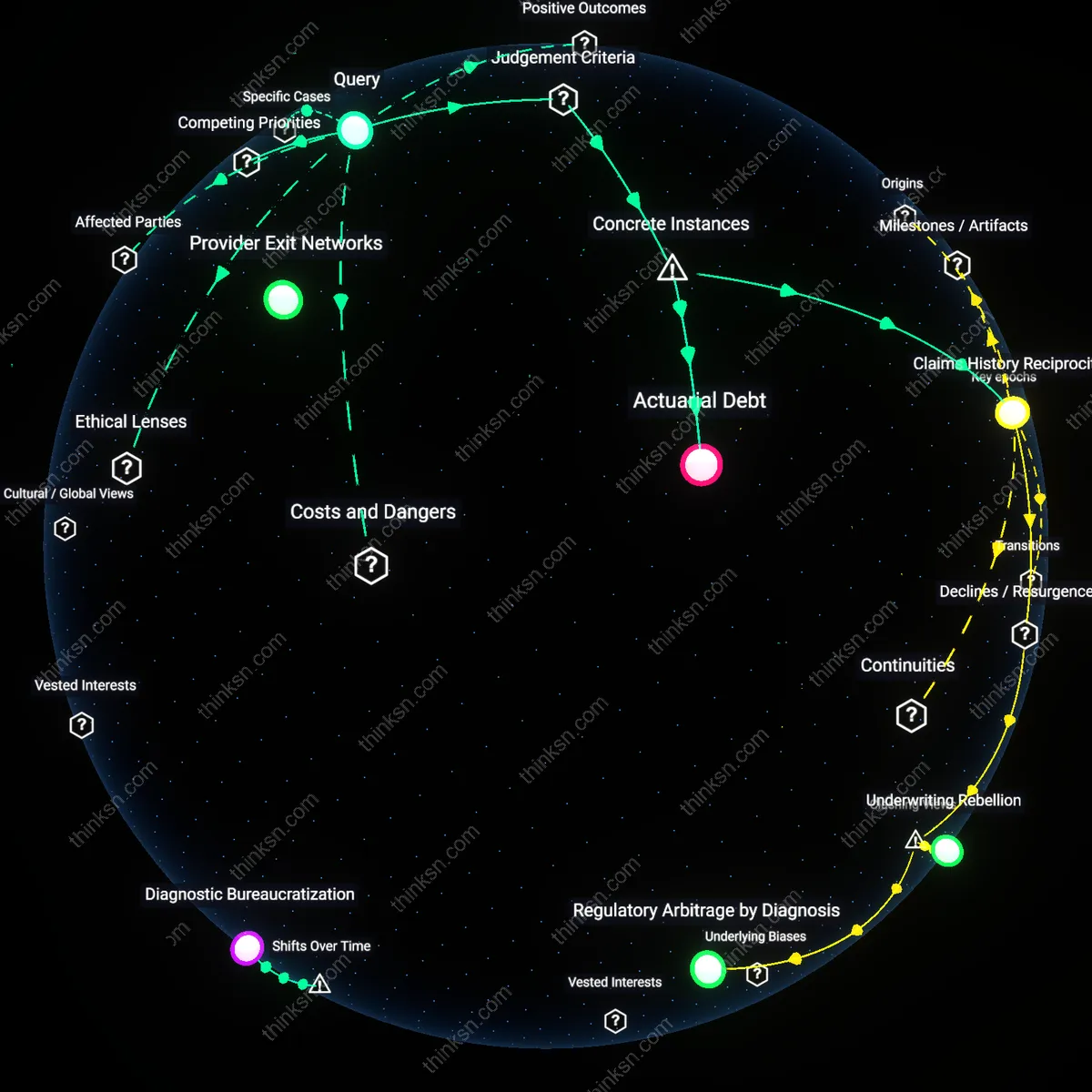
Administrative violence
Pursuing external review becomes cost-effective only when the patient’s deterioration due to untreated mental health conditions risks more expensive emergency interventions, because the U.S. healthcare system financially incentivizes reactive care over preventive access. Insurers limit pre-authorization approvals knowing that patients facing time poverty and cognitive load from chronic illness are unlikely to endure the multi-layered appeals process, which requires coordination across providers, employers, and plan administrators. This deflection of care responsibility onto overburdened individuals sustains a hidden economy of delayed treatment, where systemic underfunding of mental health infrastructure is offloaded as personal crisis. The non-obvious consequence is that cost-effectiveness isn’t tied to resolution of the denial but to the point at which the patient’s breakdown generates higher-billed acute care events that insurers and hospitals can monetize.
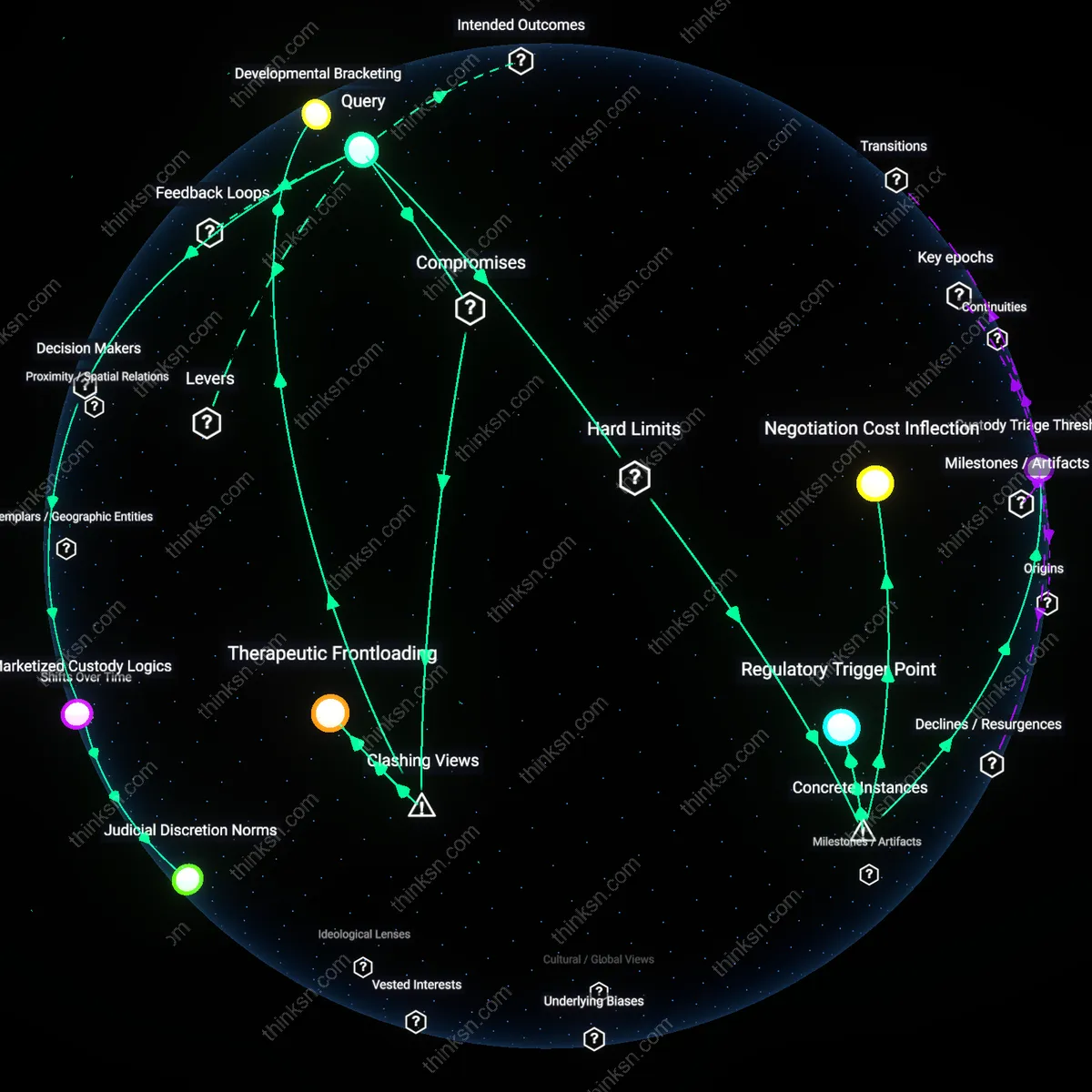
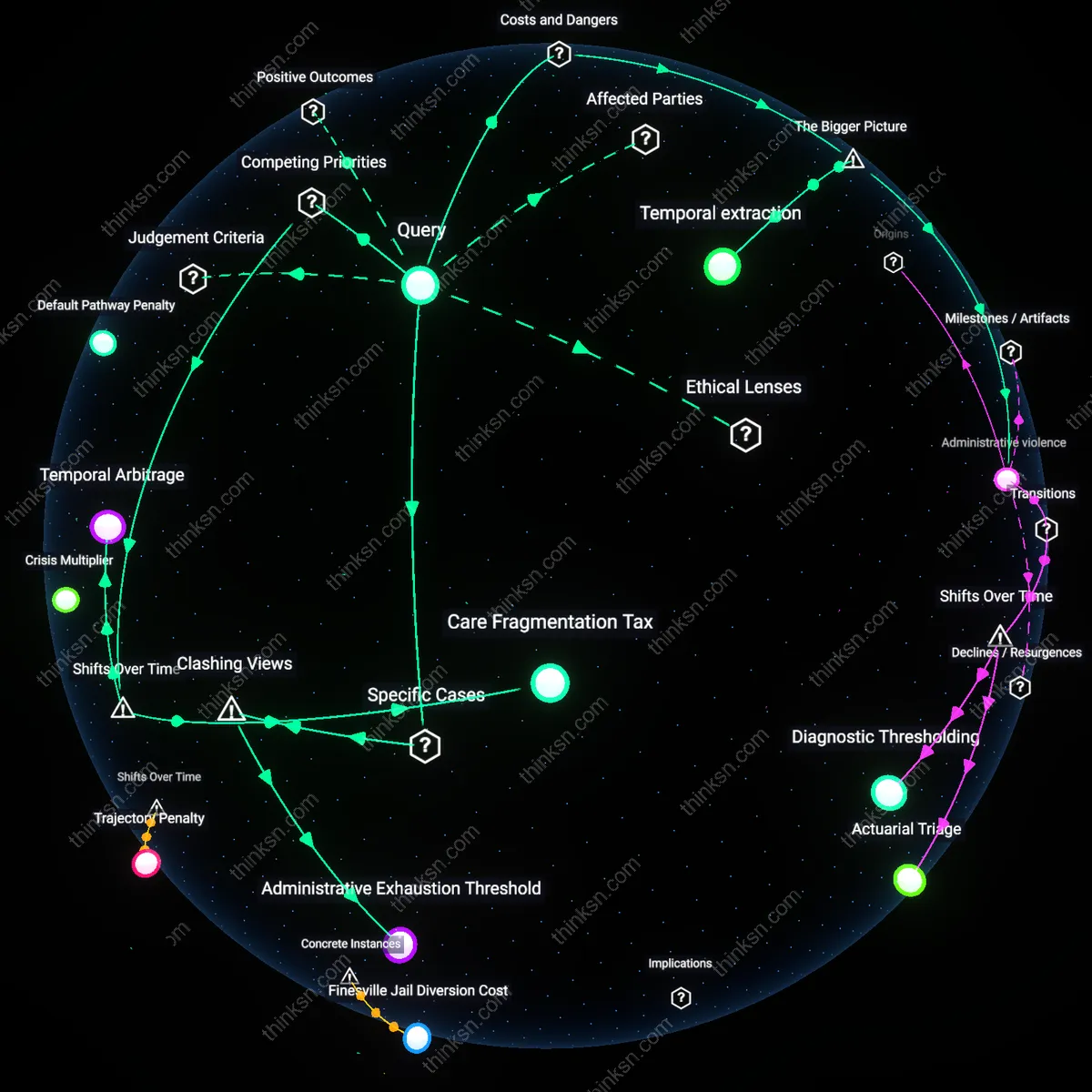
Temporal extraction
External review becomes cost-effective only when the patient’s labor time is devalued to the point that lost wages from navigating appeals are less damaging than continued untreated symptoms impairing job retention, because wage-dependent workers in precarious employment lack paid leave or flexible scheduling to manage health bureaucracy. Employers and insurers jointly benefit from structuring appeals during working hours, knowing dual-job holders face higher opportunity costs in contesting denials, which suppresses utilization of oversight mechanisms. This time-based barrier functions as a covert rationing tool embedded in benefit design, rendering parity laws unenforceable for those who cannot afford to engage them. The overlooked dynamic is that systemic efficiency depends on exhausting the patient’s temporal capacity before institutional accountability is triggered.
Temporal Arbitrage
Pursuing external review becomes cost-effective when the cumulative wage loss from reduced work capacity—due to untreated symptoms during appeal delays—exceeds out-of-pocket legal and administrative costs, a threshold that only emerged after the 2010 Mental Health Parity and Addiction Equity Act’s full enforcement lag allowed insurers to refine delay tactics, embedding systemic inertia into claims processing; this mechanism transforms time itself into a allocative resource, where patients with dual employment must strategically forfeit immediate income security to preserve long-term treatment access, revealing how parity enforcement shifted from a benefits issue to a temporal bargaining regime in which health outcomes are priced in delayed labor participation.
Diagnostic Precarity
External review turns cost-effective not at a fixed financial tipping point but when a patient’s chronic condition enters a destabilization phase—post-2013, when DSM-5 reclassification merged several anxiety and mood disorders into broader diagnostic clusters—triggering higher claims denial rates due to ambiguous symptom thresholds, which in turn increases the marginal benefit of external validation; this shift reframes clinical documentation as a contested record subject to interpretive drift, forcing patients to balance the risk of diagnostic erasure against privacy loss in evidence submission, thereby exposing how evolving diagnostic taxonomies have amplified the personal cost of insurance scrutiny.
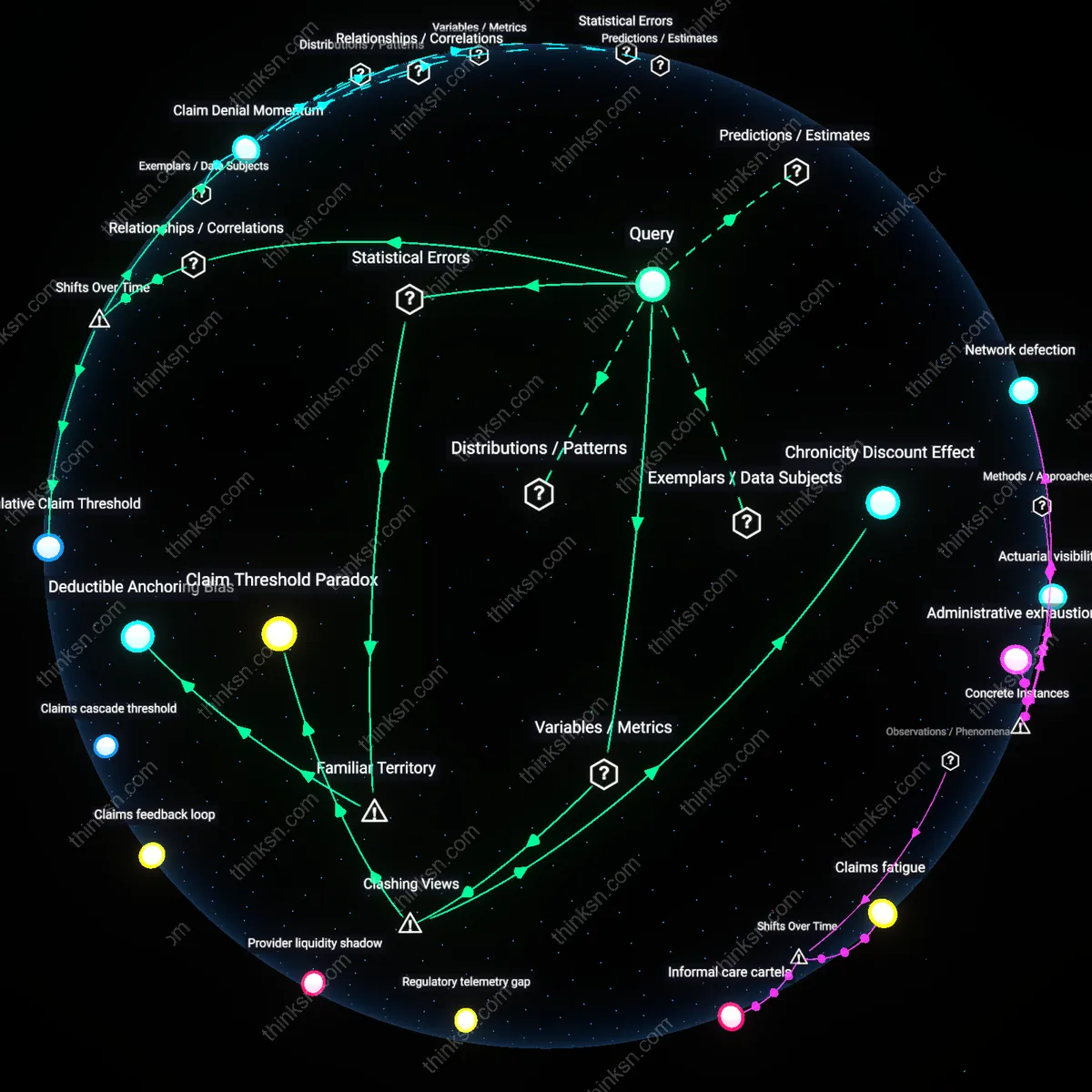
Care Fragmentation Tax
The pursuit of external review becomes economically rational only after a patient has cycled through at least two provider discontinuities caused by in-network limitations, a threshold that crystallized post-2017 as high-deductible health plans proliferated under ACA marketplace adjustments, transforming fragmented care into a de facto pre-condition for appeals; this pathway forces patients to accumulate clinical and financial dislocations as proof of medical necessity, effectively imposing a hidden cost—measured in deteriorated health and missed wages—that functions as a gatekeeping mechanism, revealing how the integration of consumer-driven health plan design has redefined treatment continuity as a premium-class privilege rather than a parity guarantee.
Administrative Exhaustion Threshold
Pursuing external review becomes cost-effective only after a patient's accumulated wage loss from denied treatment exceeds the time-adjusted burden of navigating insurer appeal protocols. In Medicaid expansion states like Michigan, where the Healthy Michigan Plan outsources behavioral health management to entities such as Magellan Health, patients with chronic depression working hourly jobs at multiple storefronts (e.g., retail and gig delivery) find that the inflection point occurs not when care is denied, but when the administrative delays directly erode scheduled shifts—documented in wage records from employers like DoorDash and Meijer. This mechanism reveals that cost-effectiveness is not driven by medical urgency but by the wage penalty of bureaucratic engagement, a dynamic obscured by parity laws that assume timely internal appeal processes.