How to Juggle High-Stakes Work and Elder Care?
Analysis reveals 5 key thematic connections.
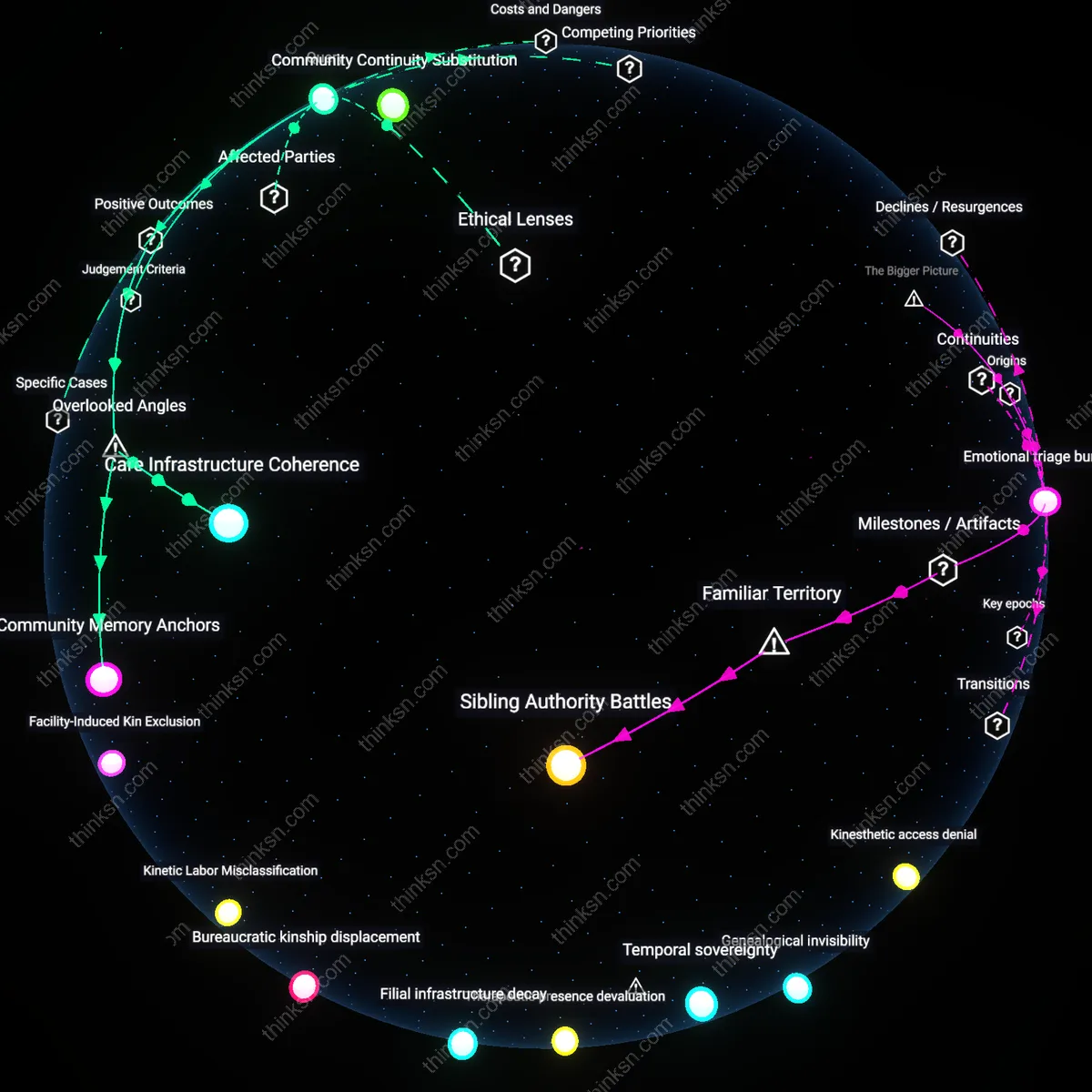
Key Findings
Care Penalty
Prioritize career deceleration over time-shifting strategies because high-status positions are structurally reinforced by punishing any deviation from linear advancement, making caregiving intervals destabilize long-term accumulation of influence and access; the system interprets even brief withdrawal as irrecoverable status loss, particularly in fields like corporate law or academia where visibility and network density are non-linearly tied to promotion; this reveals that caregiving doesn't compete with career demands—it collapses the trajectory, exposing how elite careers are maintained not by skill but by unbroken presence.
Nested Dependency
Outsource parent care to state-adjacent institutions rather than family networks because informal caregiving presumes emotional labor as infinite, creating a reinforcing loop where cultural expectations elevate sacrifice as virtue, thus masking systemic underfunding of elder support; in cities like Tokyo or Berlin, reliance on community-based elder programs reduces individual burden and reframes care as infrastructural, not moral; this disrupts the assumption that personal responsibility sustains elder wellbeing, revealing care as a governance failure disguised as family duty.
Status Arbitrage
Convert professional prestige into caregiving leverage by demanding institutional accommodations not as exceptions but as entitlements, leveraging reputation to reconfigure workplace norms—executives at firms like McKinsey or Google have successfully institutionalized part-time leadership roles, exposing that flexibility is granted not through policy but through perceived irreplaceability; this inverts the narrative of trade-offs, showing that status, when weaponized, can force systems to absorb caregiving into performance rather than oppose it.
Institutional Timebroker
Hiring a professional care coordinator enabled Dr. Atul Gawande, as detailed in his work *Being Mortal*, to delegate daily oversight of his aging father’s medical and residential needs, thereby preserving his surgical practice at Brigham and Women’s Hospital. This strategy functioned through Boston’s specialized geriatric case management networks, which operate as third-party arbiters of care quality, timing, and crisis response—freeing high-status professionals from constant direct management. The non-obvious insight is that such brokers do not merely offload labor but redistribute moral responsibility in ways that sustain both filial duty and professional identity.
Temporal Arbitrage
When former U.S. Secretary of State Condoleezza Rice structured her foreign policy engagements around weekend visits to her ailing mother in Birmingham, she exploited asynchronous commitments—using short, high-intensity family presence during diplomatic lulls to meet emotional and practical caregiving benchmarks. This pattern relied on the State Department’s rigid meeting cycles and the predictability of international summits, which allowed her to compress caregiving into non-negotiable personal windows without triggering institutional penalties. The underappreciated dynamic here is that temporal arbitrage converts bureaucratic inflexibility into personal opportunity, turning rigid schedules into reliable caregiving anchors.
Deeper Analysis
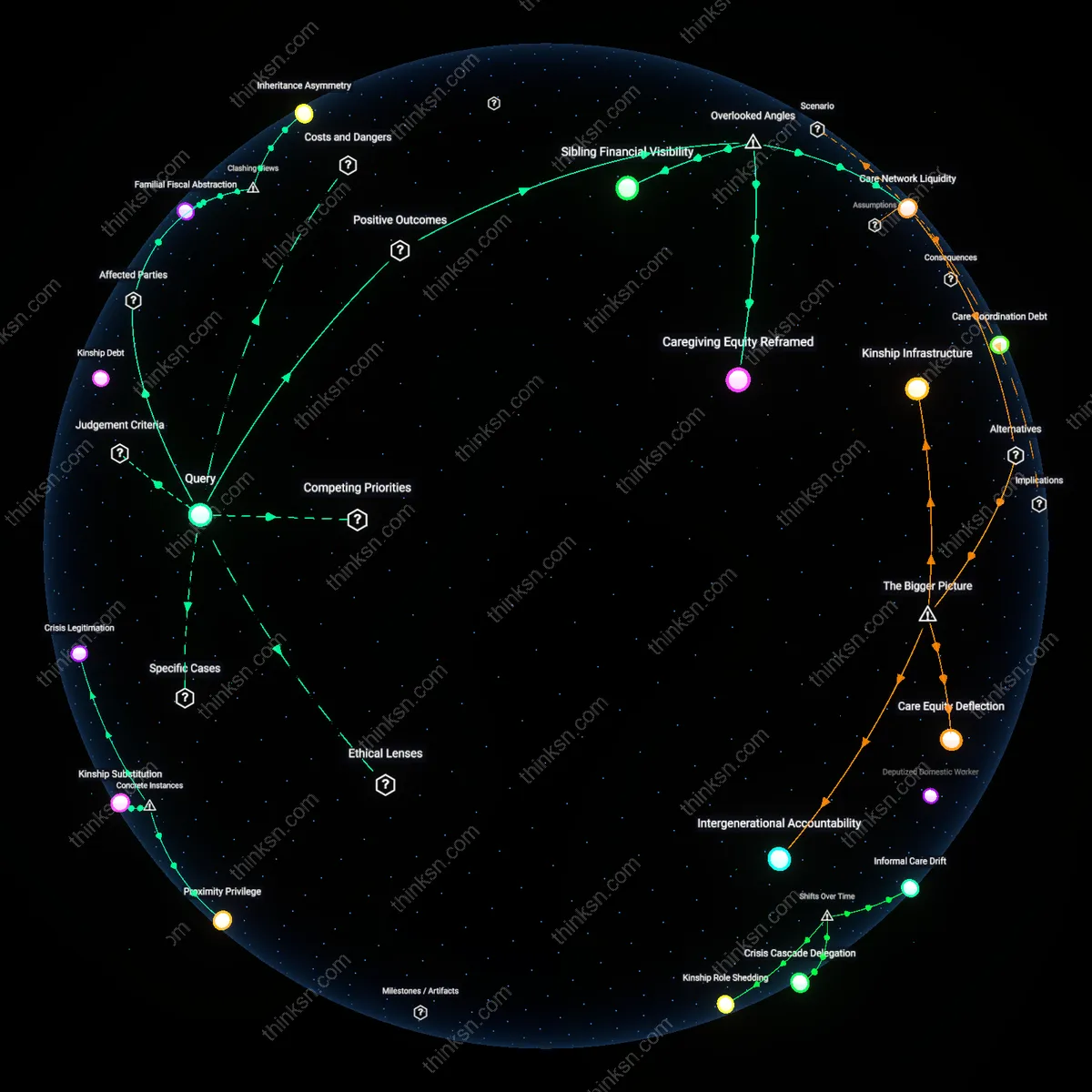
Where do the careers that demand constant presence overlap with the systems that support aging parents, and how does that shape who can actually manage both?
Urban Care Deserts
High-density metropolitan areas concentrate high-skill, in-person careers like finance, law, and healthcare in centralized business districts, while aging parents disproportionately reside in lower-density suburbs or rural regions where healthcare and assisted living infrastructure is sparse. This spatial mismatch forces adult children in cities to navigate long-distance caregiving without proximity-based support systems, making sustained professional presence incompatible with responsive elder care. The non-obvious consequence is that even high-income professionals are constrained not by time or money, but by geographic dislocation—a structural barrier that persists despite technological connectivity.
Shift Work Penalty
Industries requiring rigid, non-negotiable physical presence—such as manufacturing, emergency services, and retail—cluster in mid-density industrial or commercial zones where flexible scheduling is rare and substitute labor is limited. Workers in these roles, often from lower-education or immigrant backgrounds, face inflexible shifts that conflict with unpredictable elder care needs like medical appointments or emergencies. The underappreciated reality is that spatial fixity of both job and caregiving role amplifies vulnerability, not due to lack of willingness, but because the spatial rhythm of work leaves no room for care coordination beyond scheduled hours.
Professional Proximity Premium
In major hub cities like New York, San Francisco, and Boston, elite professional careers in consulting, law, and tech demand face-time cultures concentrated in central offices, while high-cost assisted living and private home health services are also concentrated in the same districts. This co-location creates a rare spatial alignment where affluent professionals can outsource or proximity-manage elder care, turning geographic density into a dual advantage. The overlooked insight is that this overlap doesn’t ease the burden of care—it commodifies proximity, making successful dual management a function of purchasing power rather than systemic support.
Bureaucratic Kinship
The expansion of formal eldercare infrastructure in postwar Western Europe created a jurisdictional divide where state-managed nursing systems externalized care labor onto families just as industrial work regimes demanded geographic immobility, forcing middle-class women into state-adjacent roles as care coordinators across generational borders. This arrangement emerged most clearly in the 1970s, when deindustrialization shifted employment toward white-collar sectors with rigid workplace presence requirements, even as publicly funded eldercare remained fragmented and localized—producing a residual dependency on kin that was neither informal nor private but functionally bureaucratized. The underappreciated effect of this shift is that care coordination became a second job governed by institutional timelines and documentation practices, not just emotional labor, revealing how the state, through absence, delegated administrative responsibility without granting authority.
Temporal Ghettos
In the U.S., the 1980s transition from manufacturing to service-based economies restructured time itself as a border, confining low-wage workers—especially women of color—to inflexible, hourly jobs that overlapped spatially and temporally with rapidly privatizing home healthcare zones, where aging parents were increasingly managed outside institutional reach. As Medicaid retrenched and for-profit home care agencies expanded in the 1990s, the only people able to fulfill both wage labor and care duties were those compressed into the same 24-hour cycle without temporal buffer, exposing a temporal jurisdiction where labor and care jointly discipline bodies. This compression, naturalized today as 'busyness,' actually emerged from a specific policy-driven severance of care from labor protections, making visible how time—more than space—now governs who can exist within both systems simultaneously.
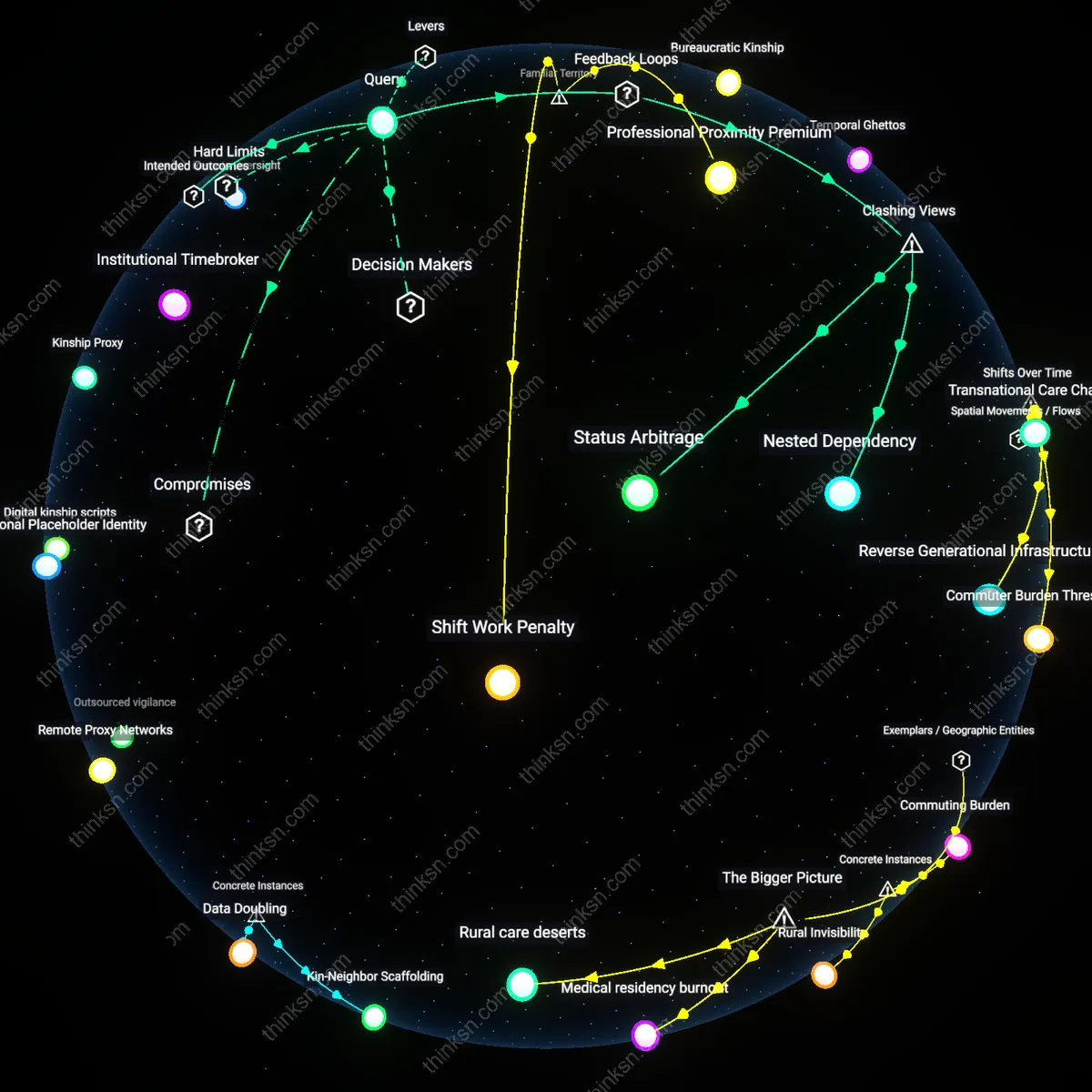
Commuting Burden
In Tokyo, Japan, software engineers working in central business districts like Shinjuku face inflexible 9-to-6 office mandates, requiring 1.5-hour commutes each way, which directly conflicts with assisting elderly parents who typically reside in outlying prefectures like Saitama or Chiba due to lower housing costs—this geographic dispersion enforced by economic necessity means daily care coordination is logistically unfeasible, exposing how corporate proximity norms in high-value sectors systematically exclude those with caregiving responsibilities. The mechanism hinges on Tokyo’s centralized employment hubs and decentralized elder housing, where transit dependency limits real-time responsiveness, revealing that the spatial disconnection is not incidental but structurally reproduced by urban economic design. This case demonstrates a hidden toll of geographic separation masked as individual time-management failure. Thus the core revelation is the physical strain imposed by mandatory centralization of prestige work in relation to caregiving peripheries.
Rural Invisibility
In rural Appalachia, home health aides employed by federally funded Medicare programs must travel across multiple counties—such as from Pike County, Kentucky, to neighboring Letcher County—to provide daily assistance to aging patients, while their own elderly relatives remain unattended at home due to lack of public transit and clustered service zones. The spatial logic of government-funded care delivery clusters routes for efficiency but ignores the dispersed kinship networks of the workers themselves, who cannot deviate from assigned circuits to assist family. This system, designed under a logistical model prioritizing route optimization over personal care needs, renders the aides’ familial obligations invisible. The underappreciated insight is that mobility-based care systems can exploit the very geography they claim to serve. Thus the core revelation is that geographic routing efficiency institutionalizes the neglect of care workers’ private kin.
Transnational Care Chains
Starting in the 1980s, women from the Philippines migrated to urban hubs in Hong Kong, Singapore, and Los Angeles to work as live-in eldercare workers, physically vacating their home communities while enabling middle-class families in destination cities to manage aging parents—this spatial displacement created a globalized circuit of deferred care, where the careers requiring constant bodily presence in wealthy regions are filled by those who cannot personally attend to their own aging kin back home. This reconfiguration emerged alongside the rollback of state-supported long-term care in developed economies and the expansion of remittance-dependent development policies in Southeast Asia, rendering care labor both hyper-local in practice and transnationally coordinated in structure. The underappreciated consequence of this shift is that the viability of elder care in one location is now systematically dependent on the absence of caregivers from another, revealing how intimate, place-bound needs are met through long-distance familial sacrifice.
Commuter Burden Threshold
Beginning in the late 1990s, the suburbanization of senior housing and the centralization of high-presence professions like healthcare and tech in dense urban cores intensified spatial mismatches, forcing adult children in cities like Atlanta or Denver to undertake long-distance weekly commutes to aging parents in outlying counties—an exhausting rhythm that became untenable as job expectations around physical availability increased during the shift to just-in-time workforce models. This growing tension between proximity to parent and proximity to workplace crystallized during the 2008 recession, when job insecurity amplified pressure to demonstrate constant workplace visibility, disproportionately excluding lower- and middle-income workers from sustaining both filial presence and career continuity. What remains overlooked is how this spatial squeeze did not merely reveal time poverty but made visible a material threshold—where geographic distance, when combined with inflexible job demands, functionally severs care capacity even when emotional and financial will exists.
Reverse Generational Infrastructures
Since the 2010s, adult children in countries like Japan and South Korea have increasingly relocated aging parents from rural hometowns to high-density apartment complexes adjacent to their urban workplaces, reversing historical patterns of youth out-migration and repositioning elderly households as satellite nodes within the professional child’s daily movement circuit—this spatial reorientation is facilitated by state-subsidized elder housing near transit corridors and enabled by the intensification of face-time-driven corporate cultures that punish remote engagement. The significance of this shift lies in how it repurposes urban infrastructure not for economic productivity alone but as a scaffold for compressed caregiving, where proximity is engineered to fit within narrow time windows between work shifts, meetings, or commutes. The overlooked transformation is that care is no longer sustained through extended cohabitation or village-based networks but through precision-calibrated spatial proximity, revealing a new infrastructural logic in which cities are retrofitted to host fleeting, high-pressure intergenerational encounters.
Medical residency burnout
U.S. hospital training programs require 80-hour workweeks for medical residents, directly conflicting with consistent physical availability needed to support aging parents, particularly in regions like New York or California where both housing costs and elder care shortages intensify dependency on family. This structural imposition—where professional advancement hinges on in-person grueling shifts—disproportionately excludes trainees from immigrant or low-income families who lack access to private eldercare alternatives, making career progression contingent on the concealment or outsourcing of caregiving. The non-obvious force here is not merely time scarcity but the institutional legitimization of overwork as professional commitment, which redefines familial responsibility as a private burden rather than a shared societal obligation.
Rural care deserts
In Appalachian Kentucky, coal-industry decline has left many mid-career workers in extractive or logistics jobs—such as trucking or surface mining—that demand long absences and unpredictable schedules, while simultaneously dismantling local health systems that once supported elderly residents, forcing family members into impossible trade-offs between income and in-person elder supervision. Here, economic precarity and geographic isolation compound, as the closure of rural clinics and transit gaps eliminate third-party support options, making individual availability the only viable care mechanism—yet the very jobs that sustain households structurally negate that availability. The overlooked reality is that labor markets in deindustrialized regions function as active care disruptors, not neutral backdrops, by designating certain bodies as simultaneously indispensable at work and irreplaceable at home.
How often do high-pressure jobs actually break down when someone tries to insert fixed caregiving times, and what falls apart first?
Care architecture mismatch
High-pressure jobs fail not because caregiving time exists, but because their operational rhythms assume uninterrupted cognitive continuity, and when fixed caregiving intervals disrupt flow-dependent tasks like surgical procedures or financial trading, the first system to collapse is situational awareness—specifically the ability to maintain real-time mental models under partial information. This breakdown reveals that the structural incompatibility lies not in time scarcity but in the misalignment between distributed attention (required for caregiving) and sustained attention (required for high-stakes performance), a conflict rarely acknowledged in workplace flexibility policies that treat time as fungible. The non-obvious insight is that it’s not the duration of absence but the fracturing of attentional threads that triggers systemic failure.
How do adult children in big cities actually manage day-to-day caregiving when they can't be physically present for their aging parents?
Distributed Surveillance
Adult children in cities manage caregiving by outsourcing their observational labor to informal local networks—like grocery delivery workers, neighbors, or temple volunteers—who report back on parents’ daily behaviors, effectively turning peripheral community members into unintended sentinels. This system relies not on technology-mediated oversight but on socially embedded monitoring, where fragmented urban routines are stitched together through quiet, non-institutionalized observation that eludes formal care models. The non-obvious insight is that physical absence does not collapse vigilance; instead, it redistributes it into existing social fissures, challenging the assumption that remote care is primarily digital or bureaucratic.
Temporal Arbitrage
Urban caregivers exert influence by manipulating off-peak time windows—such as early morning calls before work or arranging medical appointments during municipal twilight hours—to create the illusion of continuous presence with minimal time investment. This leverages asynchronous rhythms in bureaucratic and familial systems, exploiting the gap between official service hours and elders’ slower temporal cycles to schedule and verify care tasks. The friction here is that consistency in care is not achieved through proximity or volume of interaction, but via precision timing that simulates attentiveness, exposing how emotional accountability is often met through procedural mimicry rather than sustained engagement.
Proxy Accountability
Middle-class urban families outsource moral oversight to public-facing service providers—pharmacists, utility meter readers, even Didi drivers—who are quietly expected to notice and report anomalies in parents’ condition as part of uncontracted micro-duties. These workers become accidental fiduciaries, absorbing ethical risk when silence could be interpreted as negligence, thus shielding adult children from direct failure. This reveals a hidden redistribution of moral labor, where caregiving responsibility is not just logistically delegated but ethically displaced onto those whose proximity is circumstantial, undermining the narrative that technological connectivity enables responsible long-distance care.
Remote Oversight
Adult children in big cities manage caregiving by coordinating third-party in-home services through digital platforms and local agencies. They rely on verified networks of private caregivers, scheduled visits, and real-time reporting tools—often paid for through pooled family funds or insurance—to monitor parents’ health routines from a distance. This system thrives not on physical presence but on procedural surveillance, where responsibility is outsourced to measurable tasks and documented care, making trust contingent on transparency. What’s underappreciated is how this shifts the emotional labor of caregiving from hands-on interaction to administrative coordination—a role few adult children anticipate but must master.
Kinship Proxy
When physical distance prevents direct care, adult children depend on local relatives or long-standing family friends who act as their sensory extensions in parents’ daily lives. These proxies—often siblings who stayed in the hometown or cousins with nearby housing—provide observational updates, intervene during emergencies, and maintain social rituals that preserve familial continuity. Unlike formal services, these relationships operate through shared cultural expectations, reducing friction in judgment and action. The non-obvious insight is that emotional fidelity in caregiving is preserved not through technology but through preexisting kinship debts, which quietly underwrite urban children’s peace of mind.
Infrastructure Scaffolding
Urban-originating caregiving is sustained by a quietly integrated public and commercial infrastructure—pharmacies with home delivery, telehealth networks tied to provincial medical systems, and neighborhood committees in smaller cities or villages that monitor elder isolation. These systems do not frame themselves as intergenerational support networks, yet they function as such when activated by remote family coordination. The critical mechanism is not individual effort but the ambient responsiveness of localized institutions repurposed for filial duty. What goes unnoticed is how this arrangement reframes state and market systems as extensions of personal moral obligation, blurring the line between public service and private responsibility.
Outsourced vigilance
Adult children in big cities manage caregiving remotely by contracting local services to conduct in-person wellness checks and medication supervision. This shift depends on an emerging ecosystem of gig-economy elder-care intermediaries—such as Beijing-based Home24 and India’s Elders4U—that connect urban professionals with trained neighborhood monitors, transforming filial responsibility into a geographically disaggregated service chain. The realignment is driven not by technological capacity alone, but by the interplay of urban migration pressures, weak public elder infrastructure, and middle-class anxiety over moral accountability—making physical absence ethically navigable only through institutionalized presence substitution. What is underappreciated is that this system does not reduce caregiving labor but displaces it onto semi-formal workers who lack labor protections, effectively outsourcing both the task and the moral burden.
Digital kinship scripts
Urban adult children coordinate care through ritualized digital communication platforms that simulate physical co-presence and reinforce familial duty, even when geographic distance prevents direct intervention. Daily WeChat voice notes, shared Google Calendar medication alerts, and livestreamed family meals constitute a performative layer of caregiving that reassures both parent and child that relational obligations are being met—despite the absence of tactile care. This mechanism functions within a broader cultural economy of Confucian filiality, where demonstration of care is as critical as its material execution, especially in societies where state elder support remains minimal. The non-obvious insight is that these digital rituals do not compensate for lack of presence—they redefine what counts as presence, converting affective labor into measurable, monitorable digital outputs.
Remote Proxy Networks
Adult children in metropolitan hubs like Tokyo or Toronto delegate day-to-day caregiving decisions not just to formal services but to informal networks of local intermediaries—shopkeepers, neighbors, or community workers—who act as their sensory extensions in distant hometowns. These proxy figures provide unstructured observational feedback (e.g., changes in mobility or appetite) that formal medical reports often miss, enabling preemptive interventions despite physical absence. This system operates through sustained micro-trust relations rather than contractual oversight, a dynamic overlooked in policy discussions that prioritize technology or institutional care. The non-obvious insight is that geographic distance is bridged not by video calls or health apps, but by socially embedded civilians who become de facto care agents without titles or training.
Institutional Placeholder Identity
When adult children cannot be present, they often register themselves symbolically within rural healthcare and administrative systems not to perform tasks, but to occupy decision-making roles legally, ensuring that no ad-hoc local authority steps into the caregiving vacuum. In regions like rural Sichuan or Upstate New York, families enroll absent offspring as the 'authorized contact' in clinics and pension offices, even when communication is infrequent, transforming bureaucratic forms into sites of representational presence. This placeholder function prevents relatives or local officials from making unilateral choices, but depends on institutions recognizing urban absence as distinct from abandonment—an unremarked administrative fiction that sustains parental autonomy through procedural inertia. The overlooked reality is that mere nominal inclusion in a database can be a core caregiving act, altering power dynamics without direct interaction.
Proxy Witnessing
In Beijing, adult children of rural parents hospitalized during the 2020 pandemic relied on paid temporary workers from 'Dinghao' service agencies to stand in for them at bedside medical consultations, a practice that made these strangers legally non-kin surrogates who observed diagnoses and transmitted real-time audio summaries—revealing that physical absence is mitigated not by technology alone but by the insertion of informal human proxies into clinically intimate spaces, a mechanism largely unaccounted for in eldercare policy and absent from telehealth ethics frameworks.
Kin-Neighbor Scaffolding
In Detroit’s Brightmoor neighborhood, a 2018 study documented how adult daughters in Chicago coordinated care for their mothers through a trusted next-door neighbor who collected medications, checked for gas leaks, and performed daily welfare checks—activating a semi-formalized but unwritten social contract where neighborly presence functioned as a structural care extension, exposing how long-distance caregiving often depends on unmonetized, geographically tethered third parties whose role escapes formal eldercare infrastructure and remains invisible in urban policy models.
Data Doubling
A 2021 case in Tokyo showed that a son in Yokohama managed his mother’s hypertension by subscribing to a Rakuten-powered smart toilet that transmitted daily urobilinogen and protein levels to an app he monitored remotely, while also cross-referencing garbage collection logs from the city’s IoT-enabled bins to infer food consumption patterns—demonstrating how caregiving is increasingly displaced onto indirect data streams not originally designed for health surveillance, revealing a hidden dependency on ambient urban sensor networks that generate ‘care shadows’ beyond consent or regulation.