How to Balance Care for Adult Child and Spouse with Limited Time?
Analysis reveals 7 key thematic connections.
Key Findings
Shared Care Rhythm
Establish overlapping care routines between the parent and disabled spouse to institutionalize interdependence. This synchronization—such as coordinating therapy schedules or meal prep—creates a shared temporal structure that both dependents adapt to, shifting the system from reactive crisis management to a predictable cycle. The non-obvious insight is that consistency, not equal time, becomes the fairness metric, reducing guilt by making constraints visible and collectively managed rather than subjectively imposed, thus stabilizing expectations through a balancing loop.
Delegated Proxy Resilience
Designate trusted third parties—like siblings or home health aides—to serve as primary care proxies for the parent, thereby redirecting the adult child’s finite time to the disabled spouse without moral failure. This activates a feedback loop where reduced parental contact doesn’t mean neglect, because clear monitoring by others maintains stability; guilt diminishes as verification replaces presence. The insight is that in public imagination, 'care' means personal action, but resilience actually emerges from distributed responsibility—a shift that redefines duty as coordination rather than performance.
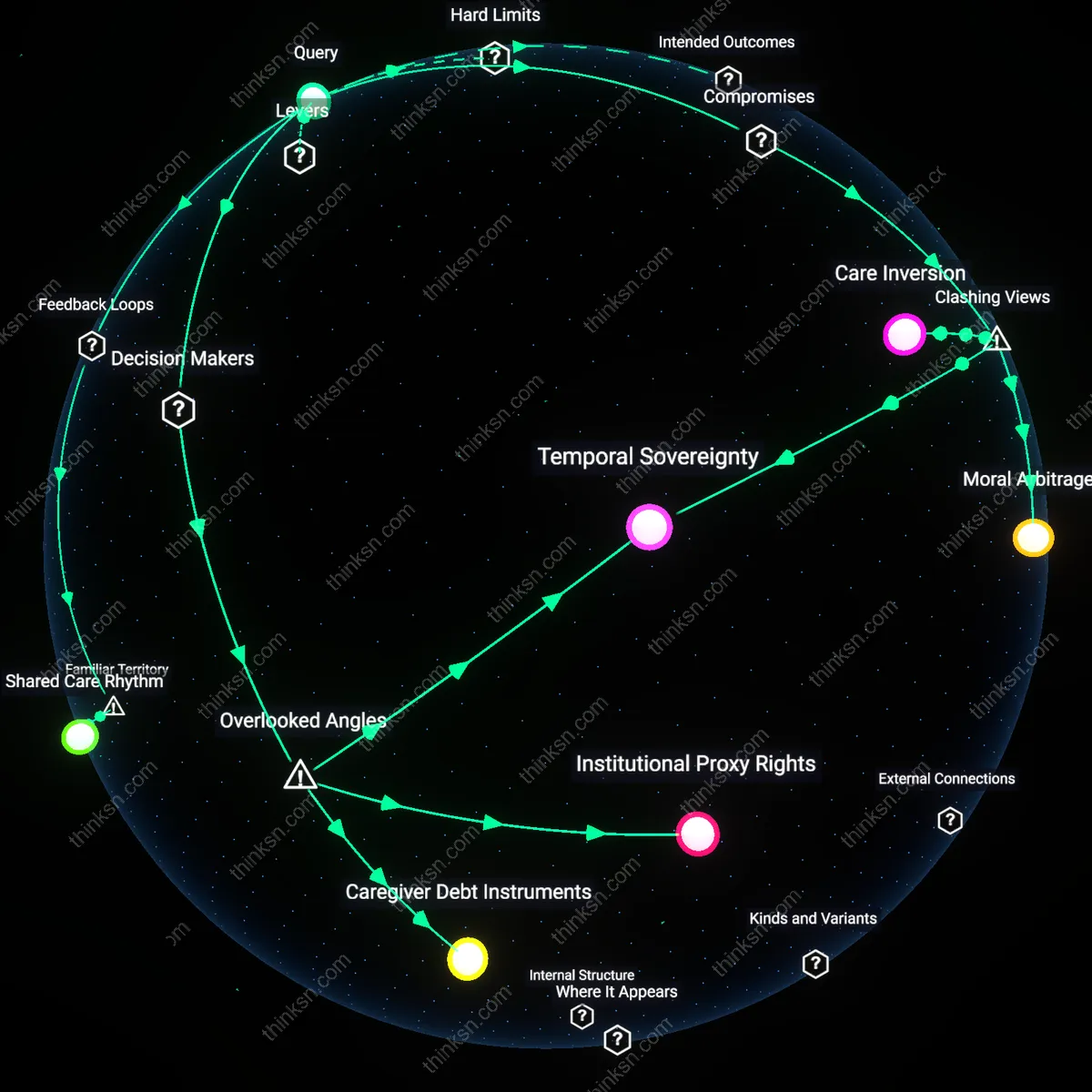
Institutional Proxy Rights
An adult child should pressure mid-level care coordinators in regional health districts to invoke underused inter-agency transfer protocols that formally shift portions of caregiving responsibility to state-licensed residential aides, thereby freeing personal time without family abandonment. Middle managers in public elder and disability services—rarely seen as decision-makers—hold de facto authority to reassign supervised care duties through existing but seldom-used clauses in home-care contracts, which permit partial delegation when dual dependency is documented; this mechanism is non-obvious because families assume total responsibility is mandatory, yet the system quietly allows distributed accountability when bureaucratic thresholds are met, revealing latent flexibility in supposedly rigid public care frameworks. Institutional Proxy Rights
Temporal Sovereignty
Designate unmediated time blocks—tracked through shared digital calendars controlled by the disabled spouse, not the adult child—because equal visibility and enforcement of personal time by the disabled spouse recalibrates moral asymmetry in care allocation. Most analyses ignore that guilt stems less from time distribution than from unilateral time adjudication; when the disabled spouse actively schedules and enforces non-care hours, it disrupts the implicit assumption that their needs suspend the caregiver’s autonomy, making fairness a jointly administered practice rather than a unilateral sacrifice. Temporal Sovereignty
Caregiver Debt Instruments
Enlist vocational rehab officers to issue skill-certification credits to the adult child that count toward future respite care entitlements, turning informal hours into transferrable claims within public care ledgers. This works through state-supported caregiver equity programs in jurisdictions like Oregon and Quebec, where documented family care time accrues toward professional respite benefits—an overlooked circuit in which moral labor becomes fungible through administrative accounting, challenging the idea that time lost to care cannot be stored or redistributed. Caregiver Debt Instruments
Care Inversion
Transfer decision-making authority for parental care to the parent’s formal healthcare providers and elder case managers, effectively demoting the adult child from primary care arbiter to logistical executor. By institutionalizing the parent’s care plan, the adult child disrupts the cultural expectation that familial love must be proven through personal sacrifice, thereby freeing time for the disabled spouse without moral penalty. This shift exposes how guilt is structurally maintained by conflating emotional responsibility with operational control—dissolving that link enables ethical redistribution. The dissonance lies in treating one’s own family role as bureaucratically optional, which contradicts the myth of the devoted, omnipresent child.
Moral Arbitrage
Intentionally accept unequal time allocation by framing the disabled spouse as the primary dependents due to the irreplaceability of spousal legal and functional interdependence, while redefining filial duty as financial and logistical support managed through third parties. This reallocation leverages the fact that spouses are legally recognized as interdependent units in healthcare, housing, and taxation, whereas parent-child obligations are culturally enforced but legally non-binding. By operating within institutional definitions of dependency, the adult child exploits a systemic bias that prioritizes marital bonds in policy, turning legal asymmetry into ethical justification. The friction is that fairness is not derived from effort but from strategic alignment with state-recognized obligations.