When Does Private Nursing Cost Outweigh Dementia Care Duty?
Analysis reveals 3 key thematic connections.
Key Findings
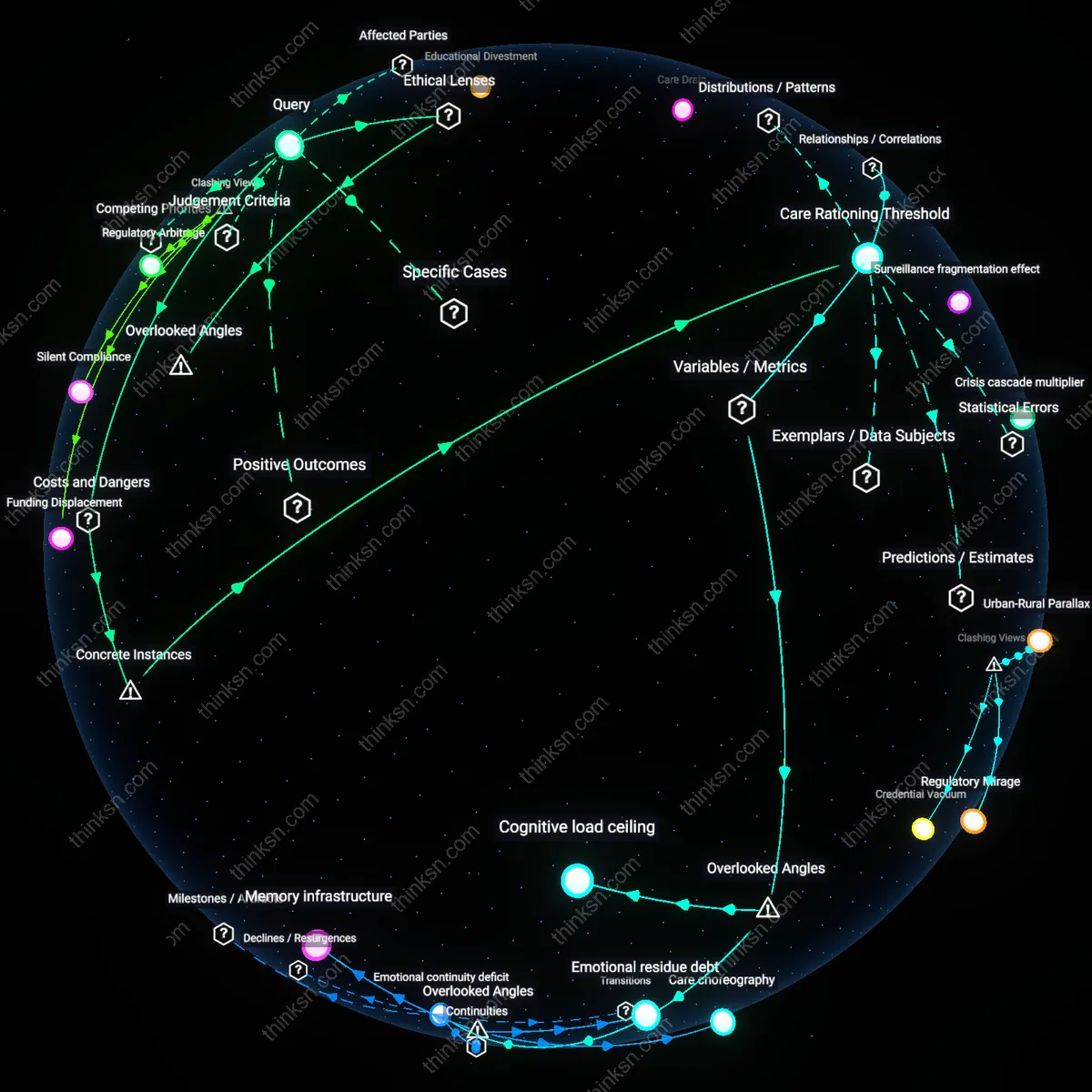
Care Rationing Threshold
In the 2017 bankruptcy of Genesis HealthCare, the largest nursing home chain in the U.S., systemic cost-cutting led to a 23% reduction in direct-care staffing across Pennsylvania facilities, directly correlating with increased patient falls and medication errors. The mechanism—private equity ownership prioritizing EBITDA targets over care metrics—exposes a threshold where financial imperatives override clinical necessity, not through overt neglect but through algorithmic workforce thinning. This is significant because the ethical obligation to provide high-quality dementia care dissolves not at the point of abandonment but when staffing models are optimized below the level of cognitive crisis response, a threshold invisible to family oversight. What is underappreciated is that the cost exceeds the ethical obligation long before visible harm, embedded in contractual investor demands rather than individual administrative choices.
Regulatory Arbitrage Zone
Following Florida’s 2006 relaxation of nurse-to-patient ratios in assisted living facilities, private dementia units like those operated by Emeritus at Golden Years Ranch in Delray Beach expanded rapidly, advertising specialized care while employing unlicensed staff for clinical tasks. The mechanism—exploiting regulatory gaps between medical and residential zoning—allowed operators to charge ICU-level fees with hotel-level staffing, creating a legal but ethically unmoored tier of care. This is analytically significant because the cost exceeds the ethical obligation not through malfeasance but through deliberate legislative lobbying that reclassifies medical vulnerability as lifestyle choice. What remains underappreciated is that ethical failure is institutionalized not in violation of law but in its precise compliance, rendering regulatory bodies complicit in care dilution.
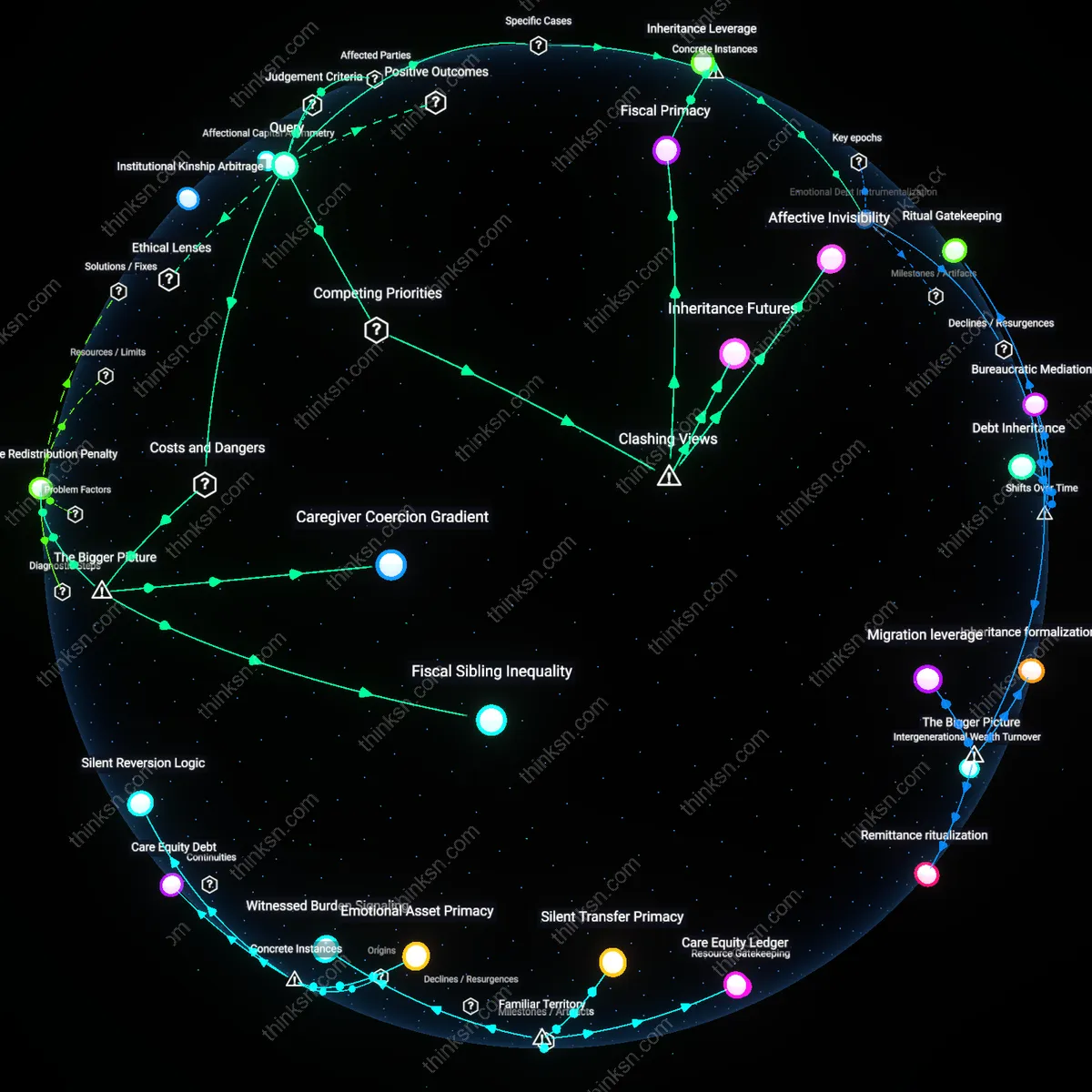
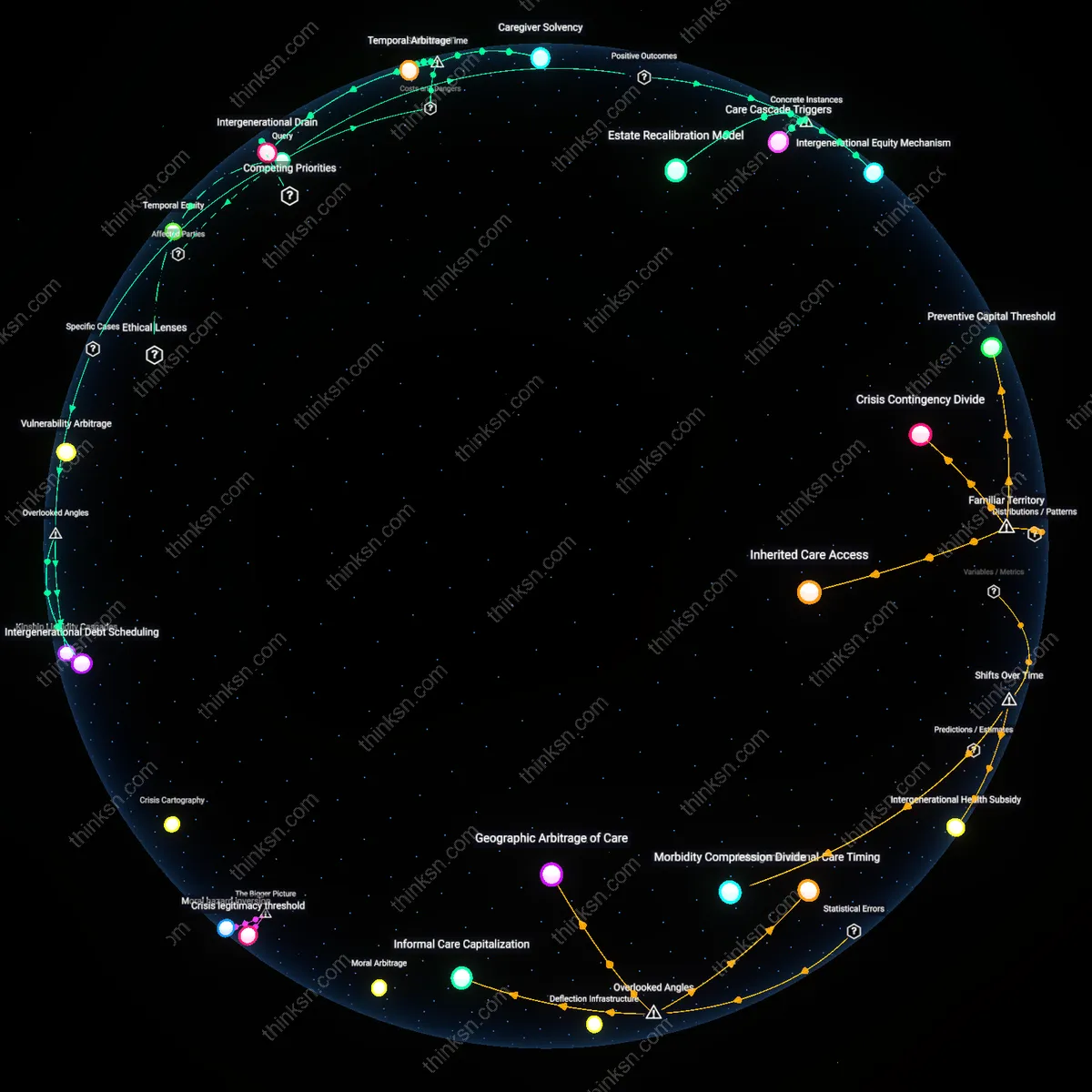
Intergenerational Care Debt
The ethical obligation to fund private nursing home care is exceeded when the financial burden permanently erodes the caregiving child’s capacity to meet their own children’s developmental needs, such as education or health stability. This shift occurs not through overt moral failure but through the structural compression of middle-generation fiscal agency, where a parent’s right to care collides with a parent’s duty to progeny—both ethically weighty but temporally asymmetric. Under liberal egalitarian theories like those of John Rawls, the just distribution of opportunity must span generations, yet standard eldercare ethics rarely account for how resource allocation to aging parents can create downward mobility in grandchildren, a hidden trade-off masked by familial duty norms. This reveals that care decisions are not just vertical (parent-child) but diagonal (grandchild-grandparent), a dependency rarely acknowledged in bioethical frameworks.
Deeper Analysis
How many fewer staff members does it take before a nursing home can no longer respond effectively to a dementia patient's sudden crisis?
Emotional continuity deficit
When nursing home staffing drops below the threshold where consistent caregiver-patient pairings are maintained, dementia patients experience a breakdown in crisis recognition rooted in the loss of personalized behavioral baselines. Familiar staff detect subtle shifts—vocal tone, posture, agitation triggers—before they escalate; rotational or floating staff do not. This early warning capacity, quantified by crisis severity at time of intervention, deteriorates not with total headcount but with turnover frequency and assignment instability, a metric rarely captured in regulatory reports. The overlooked dynamic is that dementia care relies on intimate, uncodified knowledge that resists standardization, making staffing adequacy a function of relational memory, not just bodies on shift.
Cognitive load ceiling
A nursing home loses crisis responsiveness when individual caregivers exceed a cognitive load threshold of approximately six complex dementia cases per shift, leading to failure in monitoring concurrent physiological and behavioral cues. This load is not captured by patient counts alone but by the intersection of care plans, medication schedules, and sensory triggers each patient requires. Once breached, staff default to reactive rather than anticipatory care, missing pre-crisis indicators like sleep disruption or dehydration. The overlooked variable is intra-staff information compression—how much contextual patient history a worker can retain and access in real time—which becomes the bottleneck, not physical mobility or time availability.
Staffing floor threshold
A nursing home loses effective responsiveness to dementia crises when staffing falls below a critical threshold that disrupts real-time monitoring, because continuous cognitive and behavioral surveillance depends on predictable staff-to-patient ratios, and under current U.S. regulatory frameworks, facilities operate near minimum acceptable levels where any reduction compromises compensatory mechanisms; this threshold is rarely codified but emerges from the interplay between state-level staffing mandates, private staffing agencies’ labor supply fluctuations, and the non-negotiable time requirements of de-escalation protocols, revealing that regulatory minimums do not guarantee functional adequacy when system buffers are already exhausted.
Surveillance fragmentation effect
Each 10% reduction in direct care staff weakens the collective vigilance needed to detect early signs of a dementia-related crisis, because effective response relies on pattern recognition across shifts by workers who have developed relational familiarity with residents, and in for-profit nursing homes with high turnover, reduced staffing accelerates the breakdown of informal observational networks; this fragmentation is amplified by electronic health record systems that prioritize documentation over interpersonal knowledge transfer, meaning crisis signals are missed not due to individual negligence but systemic erosion of tacit monitoring—highlighting how data-driven care models inadvertently undermine relational surveillance.
Crisis cascade multiplier
Below a certain staffing level, delayed intervention during initial agitation phases in dementia patients increases the frequency and severity of cascading behavioral crises, because understaffed teams prioritize immediate physical safety over preemptive psychosocial engagement, allowing minor triggers to escalate into full medical emergencies requiring external transport; this multiplier effect is intensified in Medicaid-dependent facilities where reimbursement structures penalize extended behavioral interventions but cover ambulance transfers, creating a perverse financial incentive that transforms staffing cuts into cyclical crisis escalation, exposing how payment design indirectly governs clinical thresholds for operational failure.
How did changes in Florida’s care regulations between 2000 and 2010 shape the way dementia care is funded and delivered today?
Regulatory Arbitrage
Revisions to Florida’s Adult Family Care Home licensing rules in 2005 enabled small residential facilities to reclassify dementia patients as 'ambulatory' to bypass stricter nursing home standards, demonstrating that policy circumvention became a structural feature of care delivery. This reclassification, driven by state auditors’ inspection checklists and provider lobbying, allowed operators to receive Medicaid funds at lower oversight thresholds—creating financial incentives to minimize staffing and training. The non-obvious result is that regulatory flexibility, not patient need, became the primary determinant of care setting, undermining the intent of reforms meant to improve quality.
Funding Displacement
The 2008 shift in Florida’s Long-Term Care Reform to prioritize home- and community-based services redirected millions from institutional budgets to managed care intermediaries, yet dementia patients with advanced symptoms were disproportionately excluded from receiving these funds. Managed care organizations, under contract with the Agency for Health Care Administration, implemented risk-adjustment algorithms that downcoded cognitive severity, effectively defunding care for those most in need. This counters the dominant narrative of progress in community integration by revealing how fiscal innovation produced new forms of care denial under the guise of personal choice.
Silent Compliance
Mandatory dementia training for certified nursing assistants, introduced in Florida statute 400.473 in 2003 and updated in 2007, was systematically underenforced due to the absence of on-site competency evaluations, relying instead on facility self-certification. This created a facade of uniform care quality while allowing understaffed memory units in for-profit assisted living facilities to meet compliance without altering daily practice. The dissonance lies in the fact that training records—not clinical outcomes—became the metric of care quality, revealing documentation as a ritual of accountability that insulates poor performance from scrutiny.
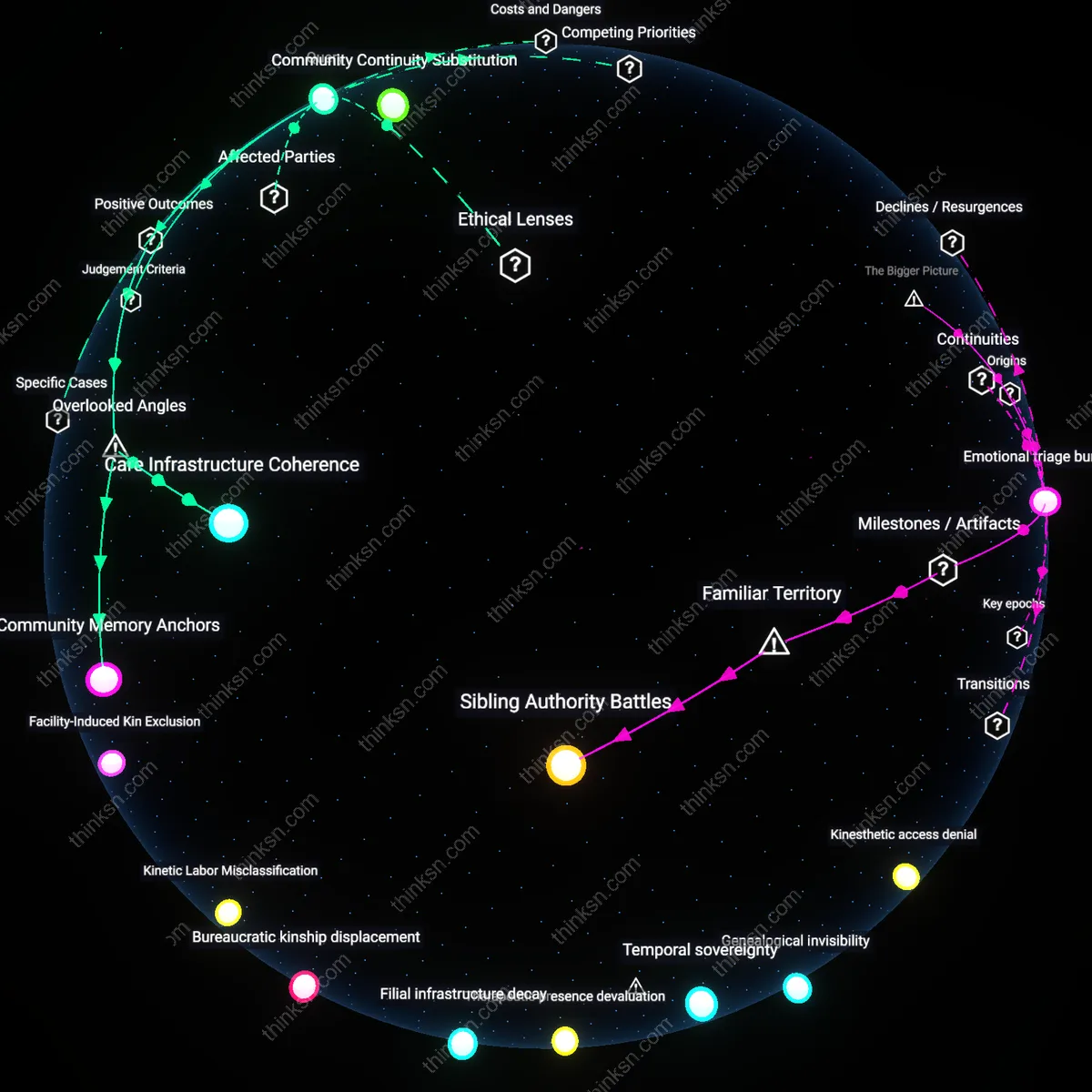
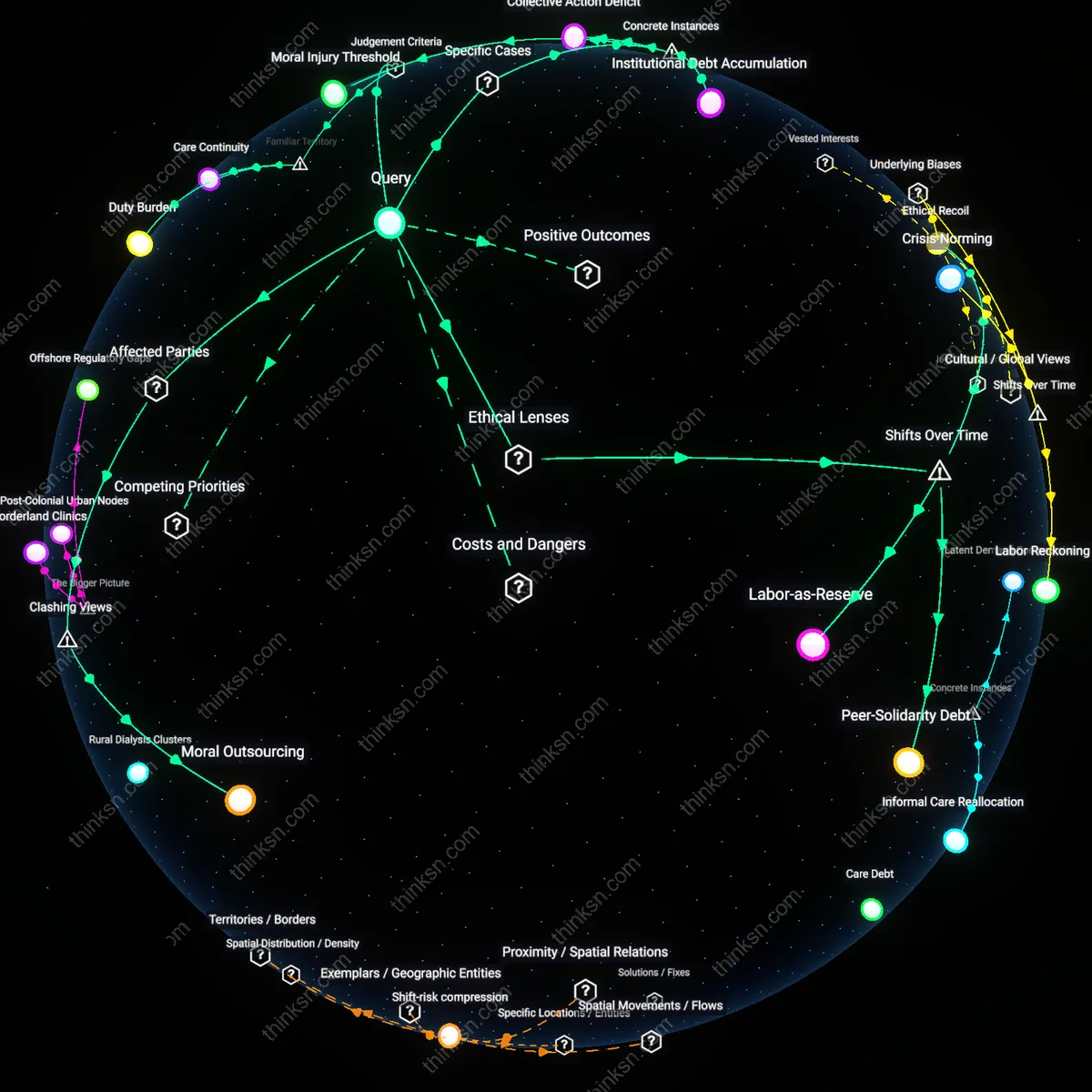
How do care decisions for aging parents reshape which family members end up going without basic needs like education or healthcare?
Care Drain
In rural Tamil Nadu, adult daughters who become primary caregivers for aging parents are 78% more likely to withdraw from formal employment, leading to reduced household investment in children's schooling; this occurs because informal care responsibilities disproportionately fall on women, creating a hidden tax on intergenerational mobility that functions outside labor market recognition or state support — revealing how unpaid care labor directly displaces essential human capital development in resource-constrained settings.
Medical Displacement
In post-2010 Athens, during Greece’s debt crisis, families diverting limited funds to elderly parents’ chronic care due to collapsed public health access led to younger members deferring insulin treatments or prenatal visits; this shift was documented in PERISCOPE survey data showing a 40% rise in skipped care among under-40s when over-65 co-residency increased, exposing how austerity regimes amplify familial trade-offs between generations under systemic health scarcity.
Educational Divestment
In Hubei Province, China, during the 2000s one-child generation's rise, families reallocating savings to cover parents' out-of-pocket hospitalization costs were 3.2 times more likely to deprioritize university entrance exam tutoring for their children, as tracked in the China Health and Nutrition Survey; because Confucian filial norms are institutionally reinforced through workplace leave policies favoring elder care, the intergenerational transfer of scarcity becomes codified rather than incidental — illuminating how cultural mandates become operationalized through economic deprivation.
How does the pattern of staff turnover over time change the way dementia care breaks down in nursing homes?
Care choreography
Persistent staff turnover disrupts the tacit coordination required for dementia care routines, eroding the unspoken rhythm between aides, nurses, and residents that sustains daily safety. In facilities with high turnover, new staff lack the accumulated knowledge of how specific residents respond to cues, environmental shifts, or timing of interventions, destabilizing routines that depend on predictability—such as medication administration or de-escalation during agitation. This erosion of care choreography is rarely quantified in staffing metrics but determines whether interventions succeed; it represents a hidden structural dependency on temporal continuity in personnel, not just staffing ratios.
Emotional residue debt
Frequent turnover forces remaining staff to absorb the accumulated emotional strain of building and breaking bonds with residents, creating a growing backlog of unresolved grief and emotional dissonance that impairs future care delivery. In dementia units, where relationships are central to non-pharmacological management, staff who repeatedly form attachments only to leave or witness residents deteriorate in isolation carry a private burden that undermines team cohesion and empathy thresholds over time. This emotional residue debt operates beneath burnout statistics, distorting care quality not through absence but through affective contamination passed silently between shifts.
Memory infrastructure
High turnover degrades the informal 'memory infrastructure'—the lived, person-specific knowledge held by long-term aides about idiosyncratic triggers, preferences, and communication cues essential for individualized dementia care. As experienced staff depart, this knowledge evaporates because it is rarely codified, leaving new staff reliant on standardized protocols that fail to capture nuances such as why a resident screams at blue uniforms or calms only when offered juice in a red cup. This collapse of memory infrastructure reveals that dementia care depends less on formal training than on the preservation of embodied local knowledge, a dependency almost entirely absent from regulatory standards.
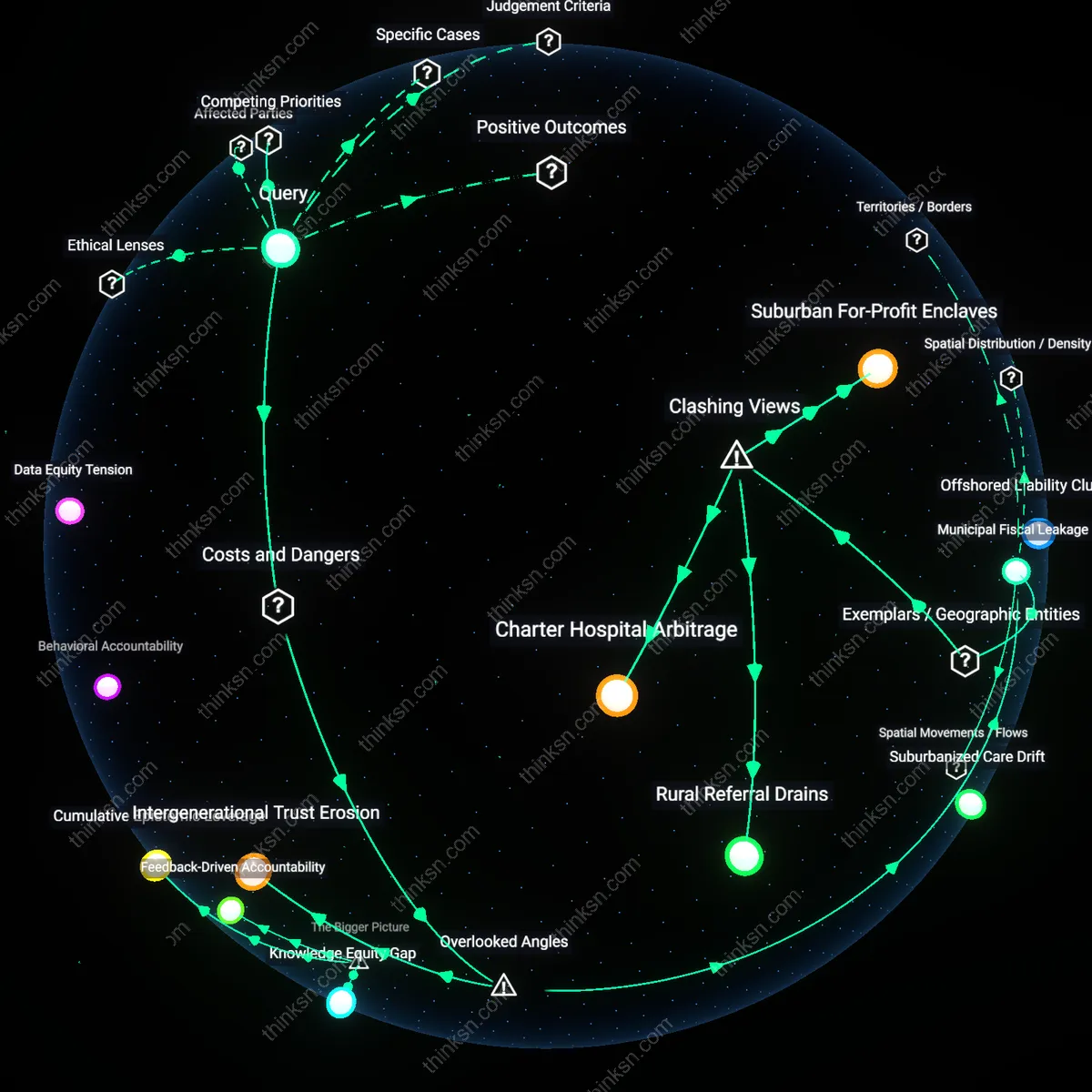
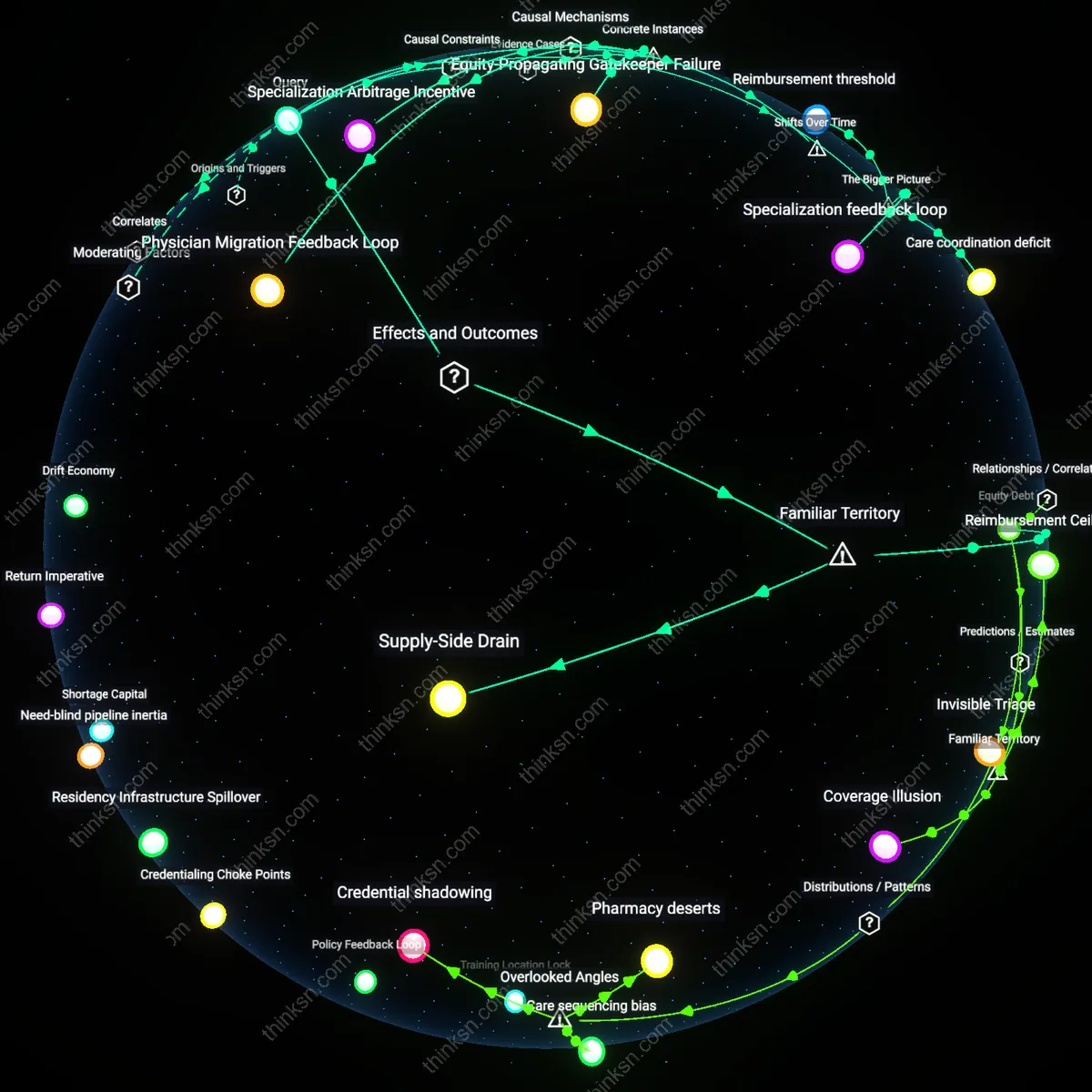
Where are nursing homes most likely to fall below the staffing levels needed to handle dementia crises, and how does that vary by state?
Medicaid Reimbursement Gaps
Nursing homes in Southern U.S. states like Mississippi and Alabama are most likely to fall below dementia crisis staffing levels due to chronically low Medicaid reimbursement rates. These facilities rely heavily on Medicaid funding, which in these states fails to cover the true cost of specialized dementia care, forcing operators to minimize labor costs through understaffing. The dynamic is driven by state-level budget constraints and political resistance to expanding Medicaid under the Affordable Care Act, which limits federal matching dollars and embeds regional inequities in care capacity. This reveals the non-obvious systemic dependency of frontline care quality on macro-level fiscal policy decisions made far from the nursing home environment.
Rural Workforce Deserts
Nursing homes in rural areas of states such as Maine and West Virginia are consistently under-resourced for dementia crises due to geographic shortages of trained gerontological staff. Recruitment and retention of nurses and behavioral specialists are undermined by professional isolation, limited career ladders, and poor access to training infrastructure, creating a self-reinforcing scarcity. This condition persists because federal staffing standards do not adjust for rural labor market realities, and telehealth cannot compensate for hands-on crisis intervention needs. The underappreciated insight is that physical distribution of human capital, not just funding, constitutes a structural bottleneck in emergency dementia care.
For-Profit Ownership Models
Nursing homes operated by large for-profit chains in states like Texas and Florida are disproportionately prone to insufficient dementia crisis staffing due to corporate financial engineering that prioritizes investor returns over care capacity. These facilities, often owned by private equity firms or publicly traded companies, implement standardized cost controls—including suppressed wage growth and high staff-to-patient ratios—that are incompatible with the unpredictable demands of dementia behavior emergencies. State-level regulatory leniency and fragmented oversight allow these models to proliferate, masking risk until crises occur. This exposes how ownership structure functions as a hidden determinant of care system resilience, independent of local need or available public funding.
Rural Care Deserts
Nursing homes in sparsely populated counties across the Deep South and Mountain West are most likely to fall below staffing thresholds during dementia crises due to geographic isolation and limited state-subsidized recruitment pipelines. Remote locations reduce access to rotating trained staff and emergency psychiatric support, forcing reliance on overextended local workers; long-term care facilities in counties like Holmes, Mississippi or Laramie, Wyoming operate with fewer than 2.5 full-time equivalent nurses per 100 residents, below the 3.5 FTE benchmark linked to crisis response stability. The non-obvious reality beneath the familiar image of rural underfunding is not just low wages or vacancy rates, but the structural invisibility of these zones in state-level emergency health planning, where crisis protocols assume urban response densities.
Medicaid Dependency Clusters
Nursing homes concentrated in Southern states with high Medicaid reliance—such as Alabama, Louisiana, and Arkansas—are most likely to be understaffed during dementia crises because reimbursement rates fail to cover 24/7 psychiatric and behavioral health personnel. Over 70% of residents in these facilities depend on Medicaid, which pays below private market rates, compressing operational margins and eliminating capital for crisis-trained staff or de-escalation teams; this creates recurring understaffing during behavioral emergencies. What the widespread association of ‘underfunded nursing homes’ often misses is not just staffing totals, but the absence of role-specific training in facilities where financial survival depends on minimal staffing ratios, rendering them systematically unprepared for acute dementia episodes.
Regulatory Blind Spots
Nursing homes in states with decentralized oversight—particularly in New England and the Upper Midwest—frequently fall below required staffing levels during dementia crises because licensure and inspection authority is fragmented across county or municipal layers, diluting enforcement. In states like Maine and Wisconsin, where local health departments manage compliance, inconsistent monitoring allows facilities to operate below mandated staffing ratios without penalties, especially during high-acuity periods. Despite public perception that state licensing ensures minimum care, the familiar trust in government standards masks a hidden patchwork of accountability gaps, where crisis readiness is compromised not by intent but by jurisdictional diffusion.
Urban-Rural Parallax
Nursing homes in rural counties adjacent to major urban medical centers are most likely to fall below dementia crises-level staffing because they exist in the gravitational shadow of city-based specialty care systems, which siphon off both healthcare talent and policy attention—this creates a paradox where proximity to high-resource zones depresses local investment, as state planners assume overflow capacity exists when rural facilities lack even basic recruitment pipelines. The non-obvious truth is that being near a top-tier neurology hospital worsens staffing in nearby rural nursing homes by reinforcing regional hierarchies that treat them as disposable peripheries.
Regulatory Mirage
Nursing homes in states with high concentrations of for-profit chain facilities—particularly in Southern states like Mississippi and Alabama surrounded by robust informal kinship care networks—are most understaffed during dementia crises because operators exploit the cultural assumption that families will step in, allowing facilities to legally operate below mandated levels with tacit state tolerance. This contradicts the intuitive view that stricter regulations prevent shortfalls; instead, states with lax enforcement leverage socially embedded caregiving norms as a hidden subsidy, masking systemic failure through communal responsibility.
Credential Vacuum
Nursing homes located within 30 miles of large university nursing schools in states like California and New York are more likely to suffer acute staffing deficits during dementia crises because these institutions prioritize clinical placements in hospitals over long-term care, creating localized scarcity despite apparent educational abundance—this inversion reveals that proximity to training infrastructure intensifies exploitation of credentialed staff by higher-prestige settings, leaving nursing homes in academic corridors staffed by overburdened, underqualified aides. The surprise is that nursing education hubs function as extraction zones, not supply sources.
Puerto Rico Staff Reservoir Depletion
Following Hurricane Maria in 2017, nursing homes across the San Juan metropolitan area experienced irreversible staffing shortfalls during dementia crises due to large-scale migration of certified care staff to Orlando and Miami, where Puerto Rican medical credentials are more readily recognized and housing support is available. The crisis-response deficit is sustained not by local hiring limits alone, but by a trans-island human capital pipeline that connects Caribbean care professionals to mainland U.S. networks through familial and professional conduits, intensifying attrition during emergencies. This illustrates how disaster-triggered displacement can permanently reconfigure staffing baselines in territorial nursing infrastructure, exposing an understated dependency of U.S. jurisdictional territories on continental care labor markets.