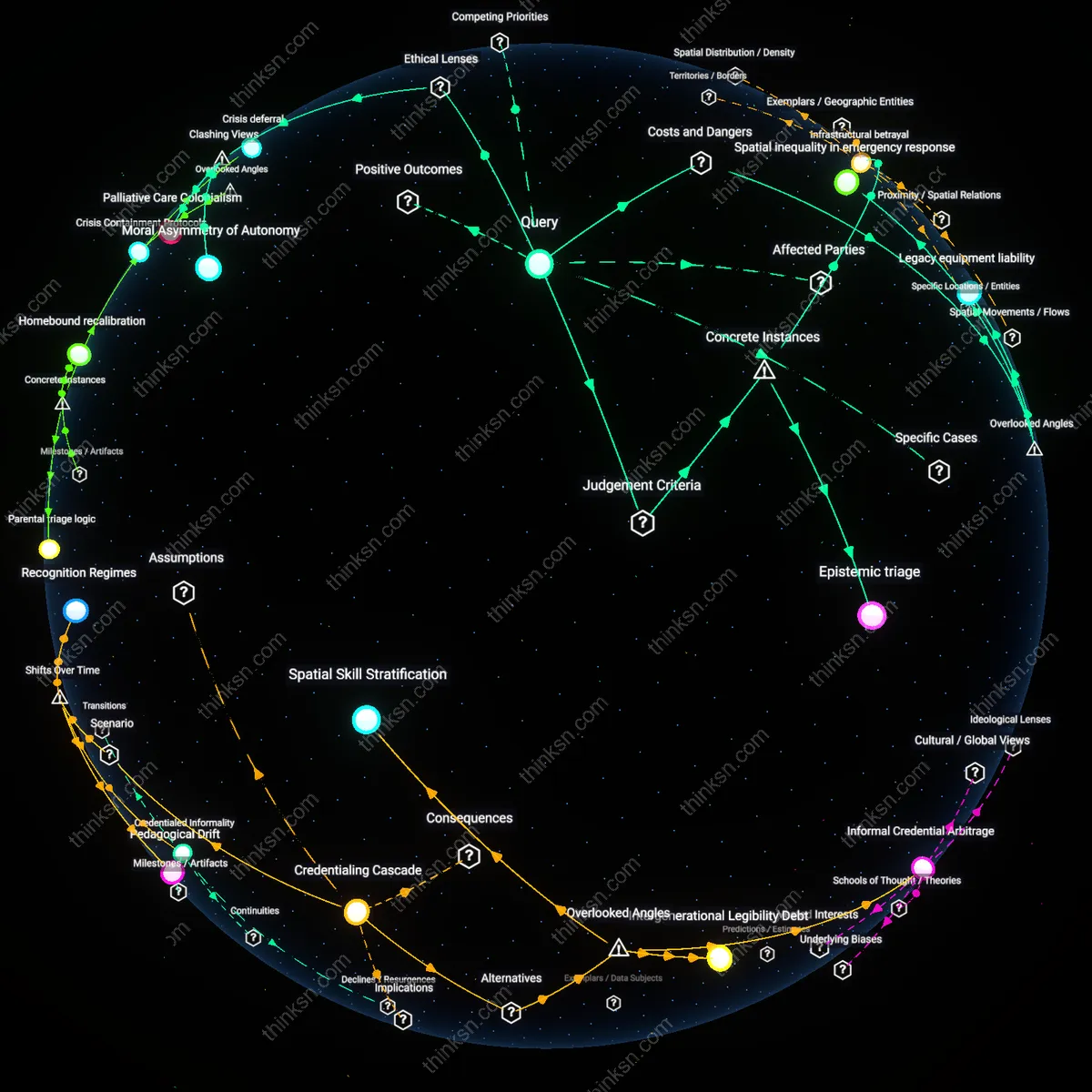
Is Taking Family Leave Rational When Patient Care Suffers?
Analysis reveals 11 key thematic connections.
Key Findings
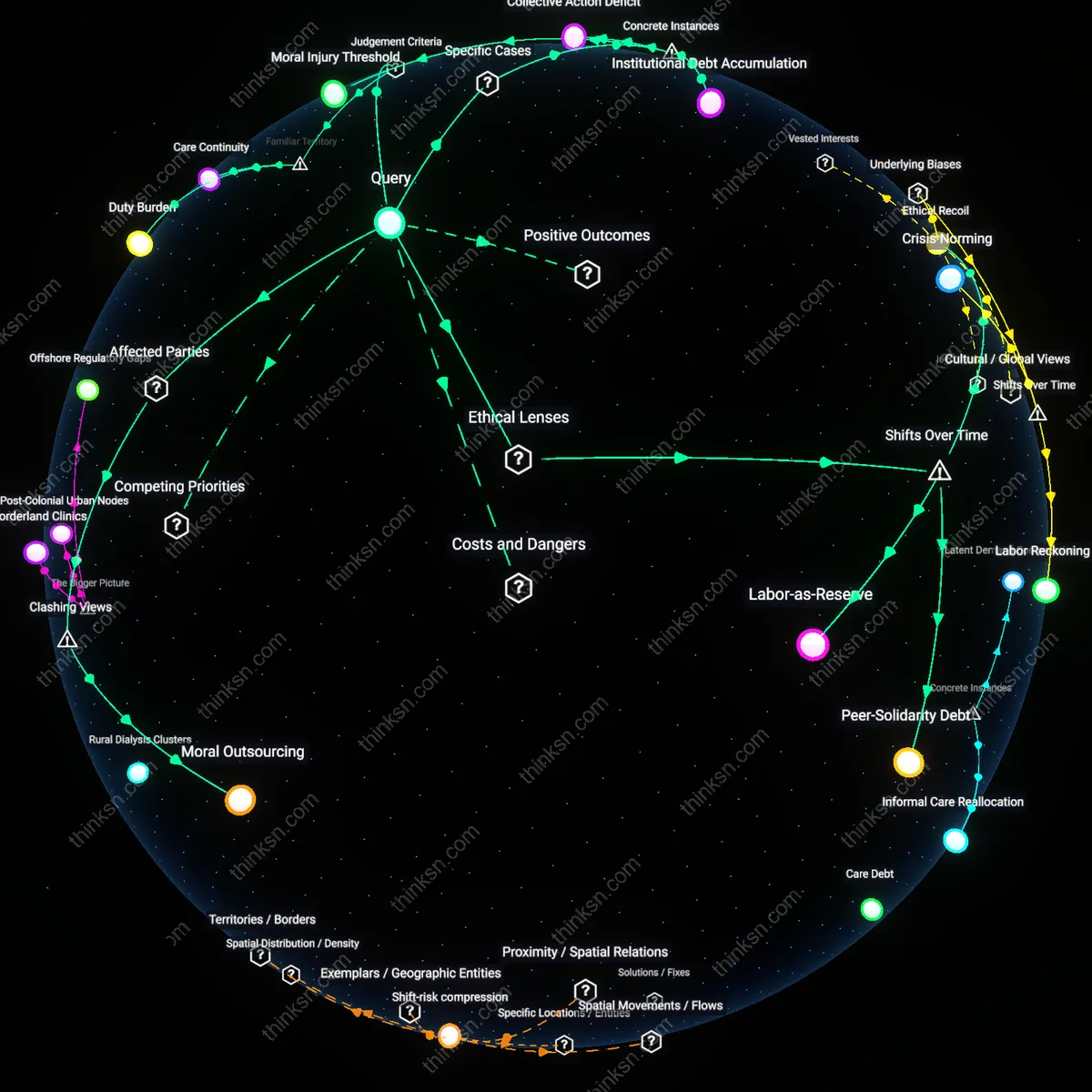
Moral Outsourcing
Yes, it is rational for a nurse to take family leave during hospital staffing shortages because institutional accountability, not individual sacrifice, should bear the burden of care continuity—shifting responsibility onto nurses frames systemic failures as personal moral tests. Hospitals and administrative leadership design staffing models, allocate budgets, and set policies that determine workforce resilience; when these systems fail, demanding nurses forfeit legally protected leave entrenches a cycle where professionals absorb institutional risk. This dynamic is most visible in for-profit hospitals in states like Texas and Florida, where nurse-to-patient ratios routinely exceed safety benchmarks, yet leaders face no liability for understaffing. The non-obvious insight is that peer resentment toward leave-taking nurses is often a redirected response to management decisions, revealing how institutions manipulate moral sentiment to obscure their own culpability.
Care Chain Sabotage
Yes, it is rational for a nurse to take family leave during staffing shortages because sustaining human caregiving capacity across generations depends on protecting caregivers’ own familial roles—disrupting one link, like parental leave, collapses the broader intergenerational infrastructure of care. When nurses delay bonding with a newborn or miss caring for an aging parent, they erode the very social foundation that produces resilient health workers, particularly among women of color who constitute a growing share of the nursing workforce and often support extended families. This mechanism operates through the lived reality of ‘second shift’ caregiving, where Black and Latina nurses in urban hospitals like those in Chicago and Los Angeles are disproportionately expected to manage home and hospital labor without institutional support. The dissonance lies in viewing leave as withdrawal when it is, in fact, investment in long-term care capacity—a truth obscured by a medical culture that treats bodies as machines needing constant operational presence.
Duty Burden
Yes, it is rational for a nurse to take family leave during staffing shortages because professional ethics prioritize caregiver autonomy when personal crises intersect with systemic labor demands. Nurses operate under binding institutional contracts that legally entitle them to protected leave, and hospitals routinely plan—through shift-swapping systems and float pools—for expected absences, meaning individual leave does not collapse care delivery. What is underappreciated in public discourse is that the moral weight of ‘duty’ is structurally distributed across the workforce and institution, not atomized onto single nurses; framing one person’s leave as endangering patients ignores administrative responsibility for resourcing and distorts the shared nature of clinical obligation.
Care Continuity
No, it is not rational for a nurse to take family leave during critical staffing shortages because frontline patient safety depends on predictable personnel density, particularly in high-acuity units like ICUs where handoffs and team coherence directly affect outcomes. In hospitals already operating below benchmark nurse-to-patient ratios, each absence increases cognitive load and error risk for remaining staff, and peer resentment accumulates when leave is perceived as disregarding team interdependence. The underappreciated reality beneath the common emphasis on individual rights is that nursing operates as a real-time coordination system—like air traffic control—where reliability depends on mutual presence, making timing and context central to ethical leave-taking.
Institutional Reciprocity
It is rational for a nurse to take family leave during staffing shortages if the hospital has previously failed to invest in staff retention, because workforce stability depends on mutual obligation between employer and employee. When institutions avoid competitive wages, mental health support, or safe staffing policies, they undermine their moral claim to expect self-sacrifice during crises, and employee leave becomes a form of corrective feedback within the labor contract. What is rarely acknowledged in public debate is that leave functions not just as a benefit but as a market signal—its use during strain reveals the imbalance in organizational reciprocity, transforming a personal decision into an indicator of institutional credibility.
Labor-as-Reserve
Yes, it is rational for a nurse to take family leave because modern hospital labor management, shaped by post-1980s neoliberal health reforms, treats nursing staff as a flexible labor reserve rather than a protected professional class, making individual leave decisions a rational response to systemic precarity. Under managed care and just-in-time staffing models, hospitals optimized cost efficiency over workforce stability, eroding collective staffing norms; this shift turned nurses’ personal time into a fungible resource, so taking legally protected leave is a rational exercise of rights within a system that instrumentalizes their labor. The non-obvious insight is that leave-taking resists normalization of perpetual availability, exposing how labor rights persist even as institutions undermine them.
Ethical Recoil
Yes, it is rational for a nurse to take family leave because the transformation of biomedical ethics after the 1970s—particularly the rise of principlism and patient autonomy—unintentionally legitimized professional self-care by shifting moral authority from institutional hierarchy to individual conscience. As nurses gained formal ethical recognition in the 1990s through codes like the ANA’s, the duty to self became ethically coextensive with duty to patient, especially during systemic failures; taking leave amid shortages thus reflects a developed professional subjectivity that resists sacrificial norms. The overlooked aspect is that this ethical maturation emerged not from policy but from decades of gendered labor struggle, reframing care work as bidirectional.
Peer-Solidarity Debt
Yes, it is rational for a nurse to take family leave because the erosion of collective bargaining power in U.S. healthcare since the 1980s has transformed peer relationships from institutional obligations into moral economies of reciprocal debt, where leave is rational not in isolation but as a claim on accumulated solidarity. As union density declined and hospitals replaced staff nurses with travel labor after 2000, peer burdens became personalized rather than structurally managed, so taking leave tests and reinforces informal support networks essential under austerity. The underappreciated reality is that such acts sustain cohesion in fragmented workforces, revealing that rationality now depends on maintaining social credit, not merely following rules or ethics.
Moral Injury Threshold
A nurse at Providence Regional Medical Center in Everett during the 2020 COVID-19 surge took legally protected FMLA leave despite peer pressure to remain, triggering a critical drop in ICU staffing that forced crisis triage protocols—this case reveals how individual compliance with legal rights can collide with informal care rationing systems, exposing a threshold where ethical duty to self fractures team-based moral coherence. The mechanism operates through institutional underinvestment in psychological safety nets, making the nurse’s rational choice generate second-order moral harm among peers who interpret the absence as abandonment, not self-preservation.
Collective Action Deficit
In 2022, when nurses at UCLA Medical Center coordinated family leave requests during a statewide staffing crisis, patient diversion orders were issued for the first time in five years—this instance shows that individually rational leave-taking, when aggregated without institutional coordination, functions as a collective action failure where each decision follows personal logic but jointly produces systemic breakdown. The dynamic emerges from the absence of shared decision-making infrastructure between staff and management, revealing that rationality at the individual level actively undermines group-level care stability.
Institutional Debt Accumulation
At Harlem Hospital in 2019, chronic understaffing preceded the resignation of 14 nurses who cited unapproved family leave rejections as a tipping point—this case demonstrates that punitive responses to leave requests during shortages compound long-term institutional debt, where organizational erosion is accelerated not by the leave itself, but by the suppression of legitimate claims. The mechanism functions through management’s short-term retention tactics, which defer relational costs and later erupt as cascading departures, revealing that rational leave decisions expose pre-existing fragilities rather than create new risks.