Abandoned corridors
In former industrial cities like Pittsburgh and Detroit, workers who qualify for lung surgery but cannot afford lost wages are increasingly ending up in understaffed public hospitals, navigating fragmented care systems that emerged after deindustrialization and Medicaid retrenchment in the 1980s. These institutions, once backup systems for acute emergencies, now function as permanent holding zones where surgical eligibility is acknowledged but deferred indefinitely due to staffing shortages and bureaucratic triage protocols that prioritize immediate survival over long-term recovery—producing a spatial limbo where medical recognition and economic impossibility collide. The non-obvious outcome is not just delayed surgery but the geographic sequestration of treatable illness in regions where post-industrial decline turned healthcare infrastructure into a temporal delay system.
Disability chasm
Across the U.S. Sun Belt—especially in Texas and Georgia—workers excluded from lung surgery due to income-related time constraints are increasingly falling into a gap between formal employment and federally recognized disability, a zone solidified after the 1996 Welfare Reform Act restricted access to SSDI for respiratory conditions lacking acute incapacitation. Because lung function decline is gradual and surgery requires preemptive time off, many remain technically 'working' while medically decompensating, disqualifying them from disability benefits but unable to sustain labor, revealing a policy-designed threshold where bodily deterioration is neither fast nor total enough to trigger state support. This chasm emerged not from absence of safety nets but from their recalibration in the 1990s to exclude those in slow-motion health collapse.
Invisible cohort
In rural Appalachia, particularly in eastern Kentucky and West Virginia, miners and industrial laborers who medically qualify for lung surgery are increasingly disappearing from institutional view altogether—operating outside both healthcare follow-up and disability registries—due to a collapse of local clinics after coal industry contraction and the 2017 closure of specialized respiratory programs funded by Black Lung benefits. Without visible tracking systems, these individuals exist in a medically acknowledged but administratively uncounted state, sustained by informal networks and over-the-counter symptom management, a condition made legible only through epidemiological gaps that began expanding in the 2010s. The overlooked shift is not refusal of care but the depopulation of care infrastructure itself, rendering need visible only in absence.
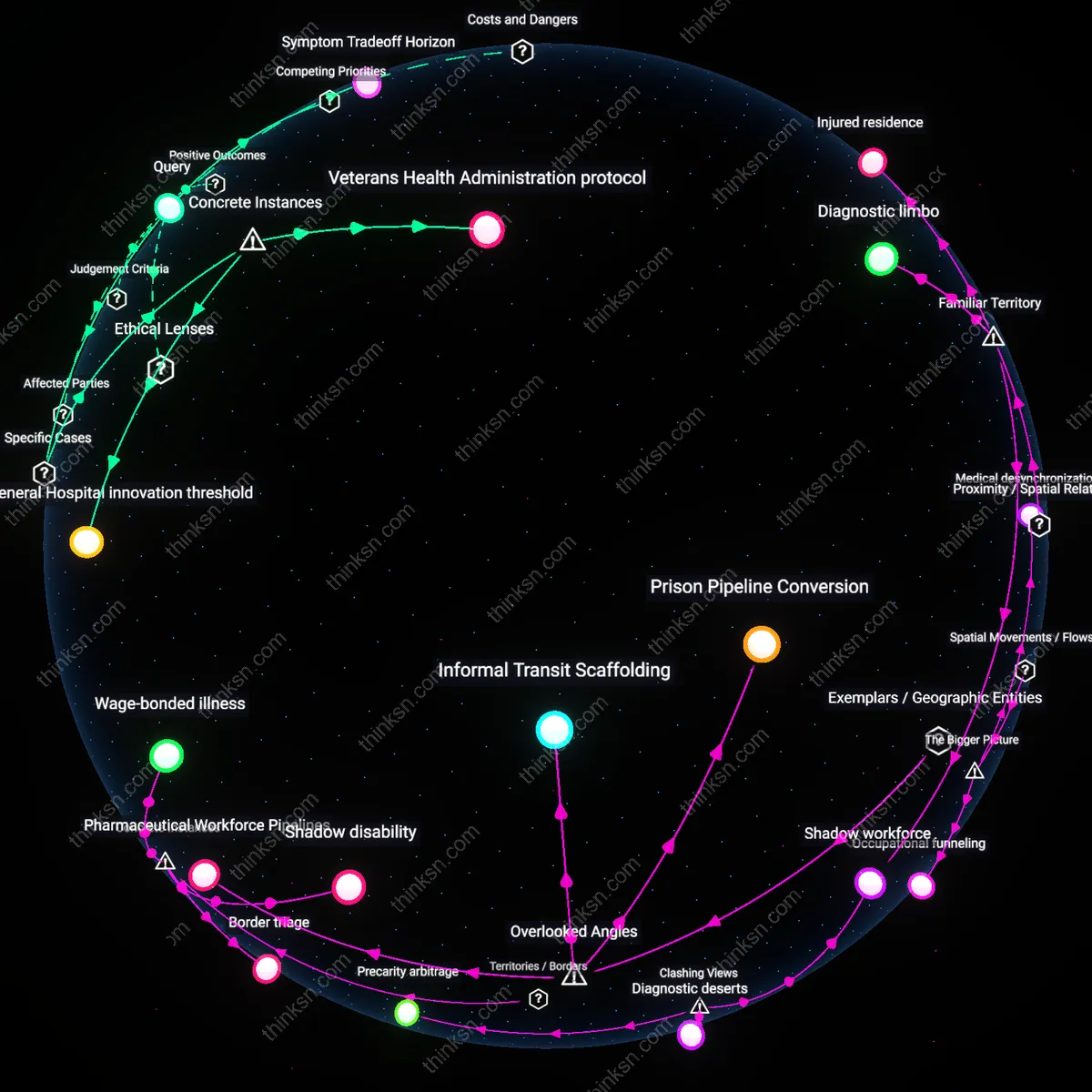
Shadow workforce
They are still working in modified but economically essential roles, often in spatial clusters like rural extraction industries or urban service economies where medical absenteeism is structurally intolerable; the mechanism is employer-dependent disability accommodation avoidance, operating through informal employer-employee risk-sharing agreements that delay care until crisis, revealing that the dominant narrative of medical exit from labor underestimates the extent of submerged, high-risk work continuation among the medically vulnerable.
Diagnostic deserts
They are ending up geographically stranded in areas with low thoracic surgery density and high primary care turnover, not because they lack insurance but because spatial maldistribution of specialists creates a de facto time tax that exceeds wage tolerance; this occurs through the misalignment of federally funded safety-net hospitals and actual residential labor patterns, challenging the assumption that time off is a personal choice rather than a function of clinical geography.
Precarity arbitrage
They are being actively retained in low-wage jobs by employers who exploit the gap between surgical recovery timelines and disability eligibility windows, using just-enough accommodations to prevent formal sick leave claims; this functions through HR-managed presenteeism protocols in gig and warehousing sectors where marginal productivity justifies health risk absorption, undermining the idea that disability systems are the primary gatekeepers of labor exit.
Shadow disability
In the Appalachian coalfields of eastern Kentucky, miners diagnosed with black lung disease who qualify for surgical intervention continue working in modified surface roles at the same mines because worker’s compensation only covers lost wages if disability is formally adjudicated, and adjudication requires leaving employment—so clinics in Harlan County document delayed surgeries while patients remain on-site as ‘light-duty reserves,’ revealing a liminal status where medical eligibility and economic survival produce a formally unrecognized category of debilitated labor. This systemic deferral—enforced by private mine operators who avoid triggering federal disability claims—converts clinical need into a silent surplus workforce, exposing how jurisdictional loopholes in OSHA and Black Lung Benefit Program borders enable employers to absorb medically excused workers as quasi-employed, undermining the very definition of disability.
Border triage
In El Paso, Texas, Mexican nationals diagnosed with advanced pulmonary fibrosis in Juárez hospitals are routinely denied surgery at U.S. medical centers despite proximity because Medicare and private insurers do not cover non-residents, even in emergencies—so physicians at William Beaumont Army Medical Center informally coordinate with cross-border clinics to provide palliative care only, while patients return to Ciudad Juárez to work in maquiladoras with compromised lung function, trapped by the Rio Grande as a biopolitical fault line. This spatial disqualification—where clinical eligibility is overridden by citizenship-based access thresholds—produces a zone of managed degradation, in which the border itself becomes a diagnostic criterion, sorting bodies by nationality rather than physiology.
Wage-bonded illness
In Omaha, Nebraska, workers at a Smithfield Foods pork processing plant who developed chronic obstructive pulmonary disease from long-term ammonia exposure qualify medically for lung volume reduction surgery, but internal HR policies tie paid medical leave to continuous hourly production output, so employees ration unpaid absences across shifts and receive surgery only during plant ‘downtime’ windows between seasonal surges, re-entering the line within 10 days post-op under OSHA-exempt ‘voluntary return’ agreements. This time-locked dependency—where employer-controlled production cycles dictate medical timing—turns recovery into a performance metric, embedding health outcomes within wage structures and exposing how labor contracts function as invisible clinical gatekeepers, binding treatment to output rather than healing.
Diagnostic limbo
They are clustering in the interstitial zones between primary care providers and overburdened specialty hospitals—often cycling through ER visits and short-term prescriptions without reaching surgical referral thresholds—because proximity to emergency infrastructure creates the illusion of access while actual pathways to intervention remain blocked by administrative delays and workplace contingency; this reflects the familiar narrative of ‘slipping through the cracks,’ where the system appears to function because people keep returning, but in fact entrenches a state of suspended medical eligibility that feels like waiting but operates as attrition.
Injured residence
They are settling in residential zones geographically isolated from both major medical centers and robust social services, such as aging suburban tracts or rural outposts where home equity substitutes for health security, relying on informal networks rather than formal support; this spatial anchoring to fixed, depreciating assets reinforces the familiar trope of ‘staying put no matter what,’ where the house itself becomes a proxy for stability even as health erodes, masking the absence of mobility—both physical and economic—with the appearance of choice.
Medical desynchronization
Patients who qualify for lung surgery but cannot afford time off work are ending up in distant urban hospitals during off-days, only to return immediately to rural job sites, creating a spatial-temporal split between care and recovery. This movement pattern emerges because employers in extractive industries—such as coal or timber in Appalachia—offer no paid medical leave, forcing workers to schedule surgeries in regional medical hubs like Lexington or Pittsburgh while maintaining residential and employment ties to remote counties. The system of fragmented labor protections and geographically centralized specialty care produces a disjuncture where treatment is accessed episodically across space but cannot be followed through locally, undermining surgical efficacy. What’s underappreciated is that the spatial flow isn’t migration toward health, but oscillation between extraction zones and medical enclaves, revealing how bodily care fails without temporal stability.
Occupational funneling
These patients are drifting into semi-structured liminal work arrangements in logistics or gig economies centered in mid-sized industrial towns, where shifts can be paused but income fluctuates, enabling just enough cash flow to avoid formal disability applications. Temporary staffing agencies in cities like Chattanooga or Youngstown actively channel post-surgical but unrecuperated workers into warehouse or delivery roles that exploit ambiguities in disability eligibility—requiring physical capacity just below the threshold for federal benefits but above sustainable exertion for compromised lungs. This spatial redistribution from rural homes to urban job basins is enabled by Medicaid’s refusal to cover travel for attendant care, making local recovery impossible without family support that often doesn’t exist. The overlooked mechanism is how spatial access to marginal work actively prevents exit from labor markets even when medically contraindicated, transforming geography into a trap.
Pharmaceutical Workforce Pipelines
Workers in rural Appalachia who qualify for lung surgery but cannot afford lost wages often end up in coal-derived pharmaceutical manufacturing plants, where disability-adjacent employment is informally structured into the hiring process. These facilities—such as those in Eastern Kentucky—routinely hire individuals with documented respiratory impairments because the work, though physically taxing, is classified as light industrial and allows irregular attendance, effectively absorbing those medically restricted from mining but still needing income. This system is sustained by regional economic monocultures and tacit coordination between occupational health clinics and employers, which rarely appears in disability policy discourse because it operates outside formal accommodations frameworks. The overlooked mechanism is not charity or government support, but the repurposing of bodily degradation into a labor-market niche—where diminished health becomes a hiring qualifier rather than a barrier.
Informal Transit Scaffolding
In cities like Delhi, where public healthcare offers free lung surgery but no recovery leave, patients often return immediately to rickshaw driving because informal transit networks absorb postoperative labor through flexible, cash-based scheduling coordinated by local union subagents. These drivers don’t formally qualify for disability due to the absence of written contracts, yet the rickshaw collectives maintain unrecorded mutual aid systems that provide short-term income replacements—only to be reclaimed through post-surgery labor premiums. This creates a de facto postoperative work pathway that is invisible to national labor surveys and healthcare outcome metrics. The overlooked dynamic is not that people work while healing, but that urban informal economies run on metabolically overdrawn bodies, where recovery time is arbitrated peer-to-peer, not through state or medical authority.
Prison Pipeline Conversion
In parts of Louisiana, individuals with surgically treatable lung conditions who cannot access paid medical leave are increasingly filtered into misdemeanor processing loops that feed into parish work-release programs, where postoperative recovery occurs under carceral labor conditions. Courts in Caddo and Orleans Parishes have shown patterns of accelerated citations for minor offenses among low-income patients discharged from public hospitals, effectively redirecting them into systems that mandate work but offer medical supervision minimal enough to qualify as care. This pathway replaces disability determination with criminal administrative status, avoiding formal income support while keeping bodies in motion. The unseen dependency is that correctional infrastructure, not healthcare or welfare systems, has become the de facto social ventilation for those whose medical needs conflict with wage labor continuity.