Is Dying at Home Always Best with Medical Gaps?
Analysis reveals 8 key thematic connections.
Key Findings
Infrastructural betrayal
Dying at home is not inherently better when rural Alaskans face 48-hour medical evacuation delays, where the collapse of emergency aeromedical infrastructure turns home death into involuntary abandonment. The Alaska Native Tribal Health Consortium documents cases where patients in remote villages cannot access critical care, rendering the romanticized choice of 'dying at home' a consequence of systemic exclusion, not preference. This reveals that autonomy in end-of-life decisions is undermined not by cultural failure but by logistical disinvestment, making physical infrastructure a silent arbiter of dignity. The non-obvious insight is that choice dissolves when geography overrides intention, exposing a moral hazard in policies that equate place of death with quality of death.
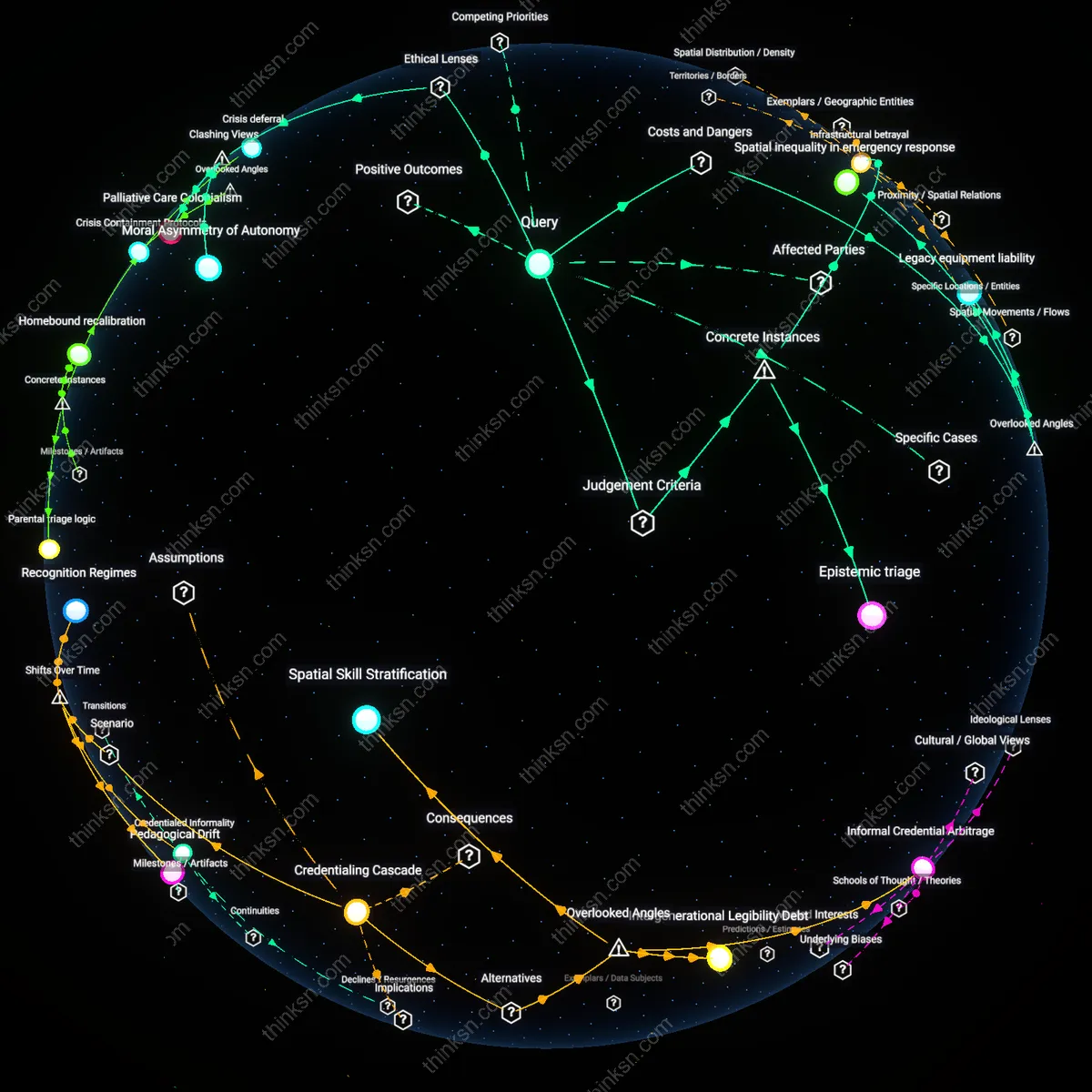
Epistemic triage
In Mumbai’s Dharavi during the 2020 COVID-19 surge, home deaths were normalized not by choice but by triage protocols that excluded slum residents from hospital beds based on age and comorbidity scoring. Field reports from Médecins Sans Frontières show that 'home dying' became the default for tens of thousands due to institutionalized resource allocation, not cultural or personal preference. This reframes home death as a category of administrative sorting, where efficiency criteria supplant patient autonomy and redefine 'better' as system-preserved rather than person-centered. The non-obvious truth is that medical triage operates epistemically—by defining who counts as 'savable'—thus producing home death as evidence of systemic exclusion, not fulfillment.
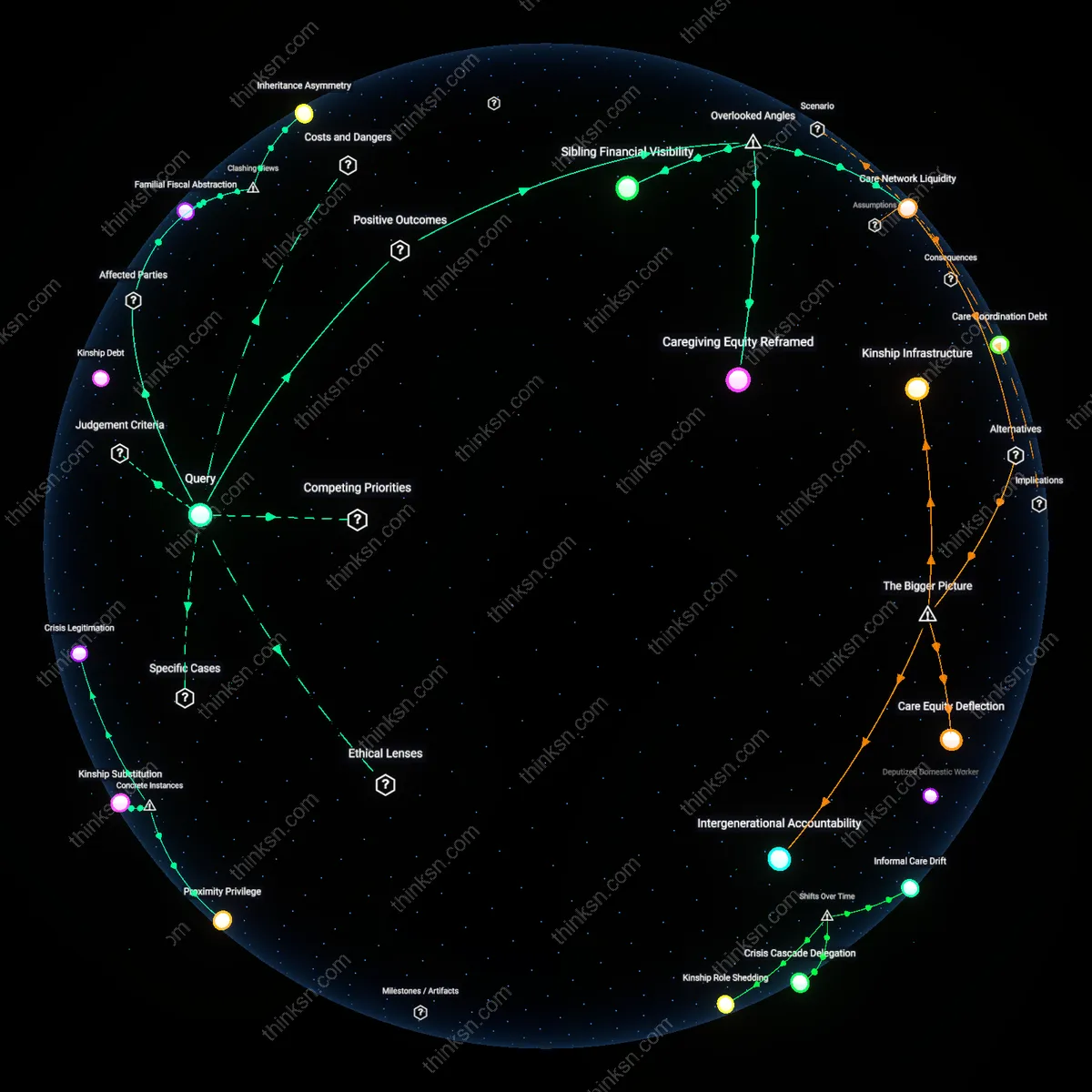
Informal caregiver burnout
Dying at home often worsens patient outcomes because it transfers critical medical labor to untrained family members, whose sustained stress leads to delayed symptom response and medical errors. In the U.S. home health system, where 70% of care is provided by informal caregivers without standardized training, chronic sleep deprivation and emotional fatigue erode decision-making capacity over time—creating a hidden failure point in home-based end-of-life care. This dynamic is rarely accounted for in policy or cost models, which treat families as frictionless care delivery units rather than vulnerable individuals at risk of collapse. The overlooked reality is that caregiver breakdown, not medical insufficiency alone, often precipitates crisis.
Spatial inequality in emergency response
The belief that dying at home is better ignores how rural geography undermines access to timely palliative intervention when complications arise. In remote areas like the northern Midwest, ambulance response times exceed 30 minutes, and telehealth infrastructure is sparse, turning minor crises into fatal events due to delayed access to specialist judgment. This creates a covert risk gradient where home death correlates with increased preventable suffering not because of patient preference failure, but because the spatial distribution of emergency capacity makes home a higher-stakes location. Most analyses assume home and hospital are connected by seamless transit, when in reality geography introduces a hidden variable in outcome disparities.
Legacy equipment liability
Home medical environments inadvertently increase patient danger by relying on consumer-grade equipment that lacks clinical monitoring safeguards, such as hospital-grade oxygen regulators or infusion pumps. When patients use repurposed or retail medical devices—common in cost-saving home setups—malfunctions are more frequent and less detectable, leading to undiagnosed hypoxia or dosage errors. This creates a latent system risk where the domestic setting appears safe but introduces technical failure modes absent in regulated facilities. The overlooked dimension is that home care often trades institutional oversight for unmonitored device autonomy, converting medical technology into a silent hazard.
Moral Asymmetry of Autonomy
The belief that dying at home is inherently better is ethically flawed because it privileges patient autonomy over distributive justice, privileging those with private resources to secure adequate home care while obscuring systemic failures in publicly funded support. This moral asymmetry operates through liberal bioethical frameworks—particularly principlism, with its emphasis on autonomy—that dominate clinical guidelines and advance care planning, yet fail to account for the material conditions required to make home death viable. The non-obvious consequence is that the right to die at home becomes a class-based entitlement, exposing how ethical norms can reinforce inequity when abstracted from structural capacity.
Clinical Invisibility of Home
Dying at home is not inherently better because the home is structurally excluded from clinical surveillance and institutional accountability, rendering complications undetected and care gaps unaddressed under the standard of care expected in hospitals. This invisibility functions through legal doctrines like the Emergency Medical Treatment and Labor Act (EMTALA) in the U.S., which mandates hospital care access but imposes no parallel obligation for home-based acute support, thereby normalizing substandard monitoring outside institutions. The contradiction reveals that the romanticization of home death depends on ignoring how medical legitimacy is legally codified within facilities, not dwellings.
Palliative Care Colonialism
The global promotion of home-based dying as ideal replicates neocolonial health ideologies by exporting Western individualist preferences to settings where kinship networks and communal care already sustain home death without medicalization. Driven by WHO palliative care policies that frame institutional care as progressive, this lens pathologizes non-hospital death in low-income countries while treating it as virtuous in high-income ones, exposing a double standard in how medical support is deemed necessary. The dissonance shows that the critique of inadequate home support is selectively applied, serving to justify health system expansion rather than respect context-specific care ecologies.