At Home or Nursing Home: Honoring End-of-Life Wishes vs. Professional Care?
Analysis reveals 6 key thematic connections.
Key Findings
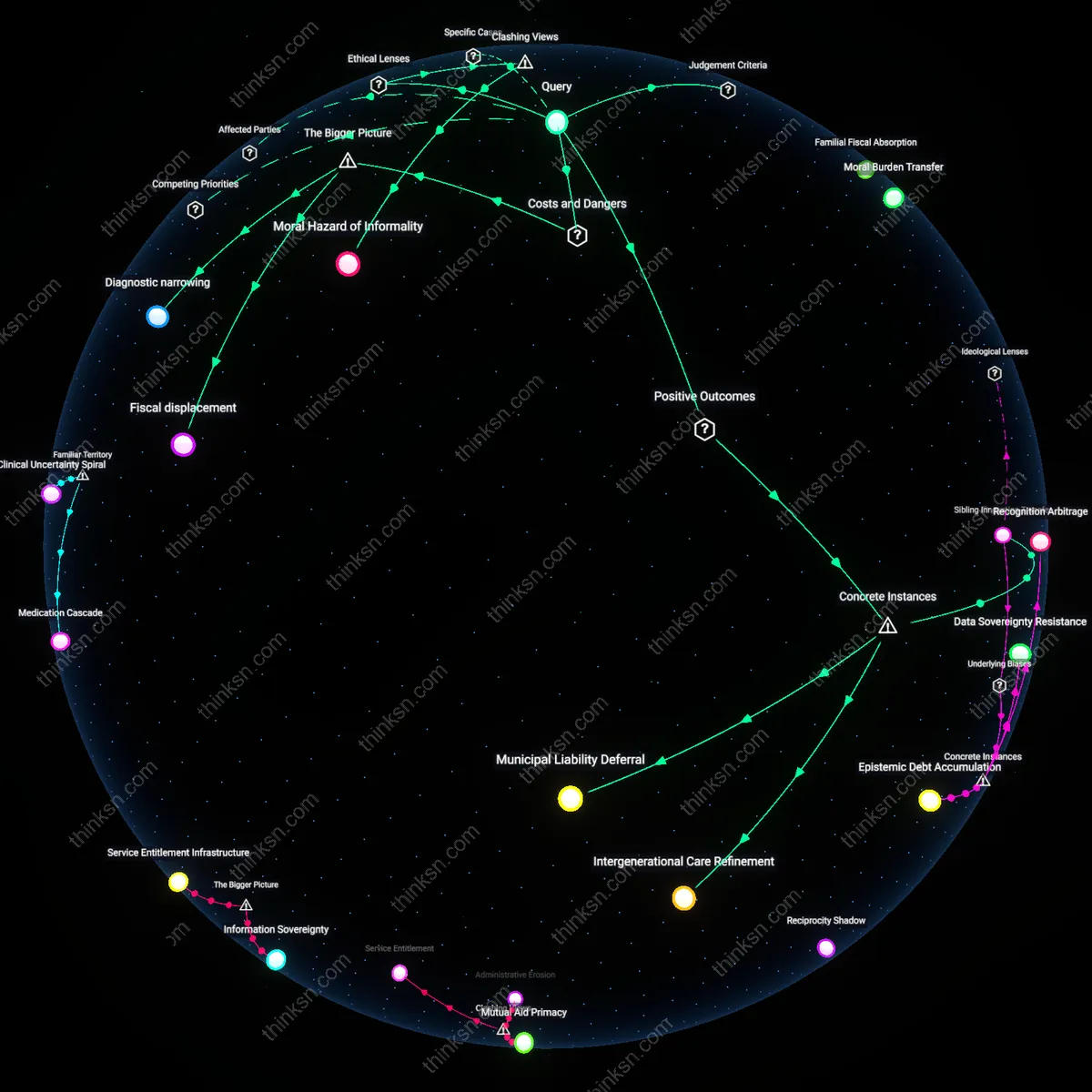
Kinship labor subsidy
Families can absorb a dying parent’s home care by relying on unpaid familial labor, primarily from female relatives, which functions as an informal subsidy to overstretched health systems unable to meet demand for in-home skilled nursing. This arrangement persists because gendered norms naturalize women’s caregiving, allowing hospitals and insurers to discharge medically complex patients into environments where round-the-clock attention is expected but not resourced—a dynamic entrenched in Medicaid’s home- and community-based services waivers, which limit public funding despite rising need. The non-obvious consequence is that private family sacrifice neutralizes political pressure to expand public long-term care infrastructure, preserving fiscal austerity under the guise of patient autonomy.
Diagnostic inflation threshold
Families can defer skilled nursing placement by escalating a parent’s medical designation—such as declaring hospice eligibility or advancing a cognitive diagnosis—to unlock home-based services otherwise unavailable, thereby aligning clinical categorization with residential preference. This works because Medicare and private insurers tie coverage for in-home nursing and equipment to specific diagnostic codes, incentivizing clinicians to stretch criteria when family capacity and advocacy are present. The underappreciated mechanism is that diagnostic precision becomes negotiable at the end of life, not due to medical ambiguity alone, but because reimbursement systems create a ladder of eligibility that families and providers jointly climb to avoid institutionalization.
Neighborhood care sovereignty
Families can sustain home-based end-of-life care by activating localized mutual aid networks—such as faith-based visiting teams, block clubs, or diaspora associations—that provide food, transport, and overnight shifts unaddressed by formal care plans. These networks operate outside clinical surveillance and insurance protocols, particularly in communities with low trust in medical institutions or immigrant enclaves with strong communal traditions, and they absorb risks that skilled nursing facilities are designed to mitigate. The overlooked reality is that urban residential stability and ethnic social cohesion function as de facto long-term care infrastructure, enabling home death not through medicalization but through social density and reciprocated obligation.
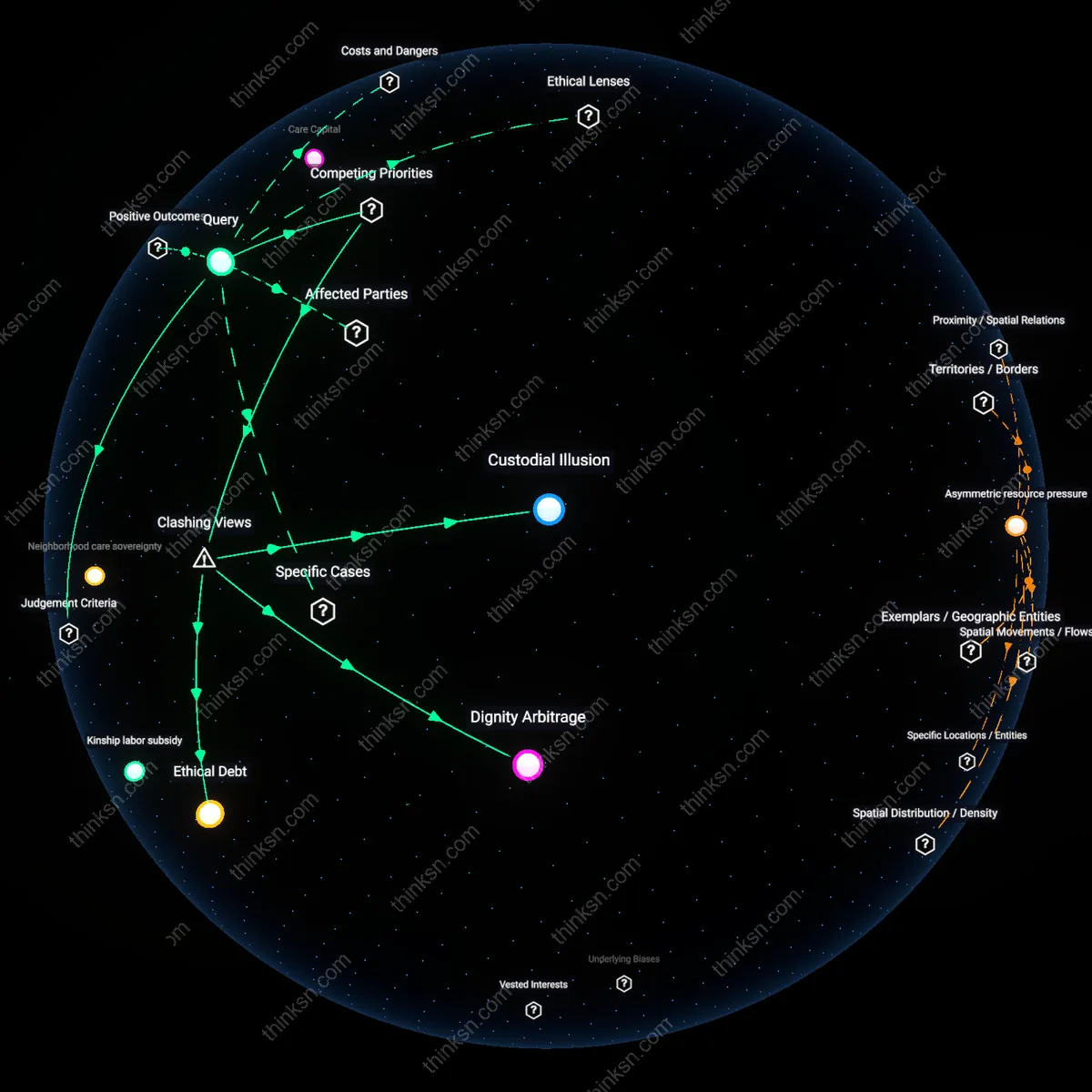
Custodial Illusion
Honor the parent's wish to remain at home by formally classifying family caregivers as de facto medical custodians, thereby shifting financial and legal liability from institutional systems to the household. This reclassification activates Medicaid's Family Caregiver Support programs in states like Oregon and Maine, where informal caregivers can be reimbursed for clinical tasks—yet it simultaneously erases the distinction between emotional presence and medical duty, turning kinship into a subcontracted labor role within the home health bureaucracy. The non-obvious consequence is that fulfilling autonomy through domestic care actually institutionalizes the family unit as an extension of the care facility, exposing the Custodial Illusion—the belief that staying home preserves independence when it often embeds the family in a covert, underregulated tier of medical compliance.
Dignity Arbitrage
Satisfy medical recommendations by temporarily admitting the parent to a skilled nursing facility during acute episodes, then rapidly cycling them back home during periods of stability, using Medicare’s 3-day rule to qualify for covered rehabilitation stays. This strategy exploits a loophole in post-acute care financing that allows families to access skilled care without permanent placement, turning the parent’s body into a mobile eligibility unit navigated through institutional thresholds. The clash arises because the medical establishment sees continuity of care as essential, while the family treats care as episodically extractable—revealing Dignity Arbitrage, where the currency of dignity is traded across settings, maximized in location but minimized in clinical coherence.
Ethical Debt
Postpone institutionalization by retrofitting the home with clinical infrastructure—hospital beds, oxygen lines, call buttons—funded through HUD’s Section 202 Supportive Housing grants and local Area Agency on Aging waivers, effectively transforming the residence into a stealth medical site. This mimics skilled care conditions without changing residence, but concentrates decision-making authority in adult children who lack clinical training yet assume diagnostic responsibilities, such as interpreting fever spikes or managing wound care. Evidence indicates this leads to delayed emergency responses and moral injury among siblings, exposing Ethical Debt—the accumulating cost of deferring institutional oversight, where short-term adherence to autonomy compounds long-term ethical burdens on unprepared family agents.