Refusing Life-Sustaining Treatment: Justifiable Sacrifice or Missed Hope?
Analysis reveals 6 key thematic connections.
Key Findings
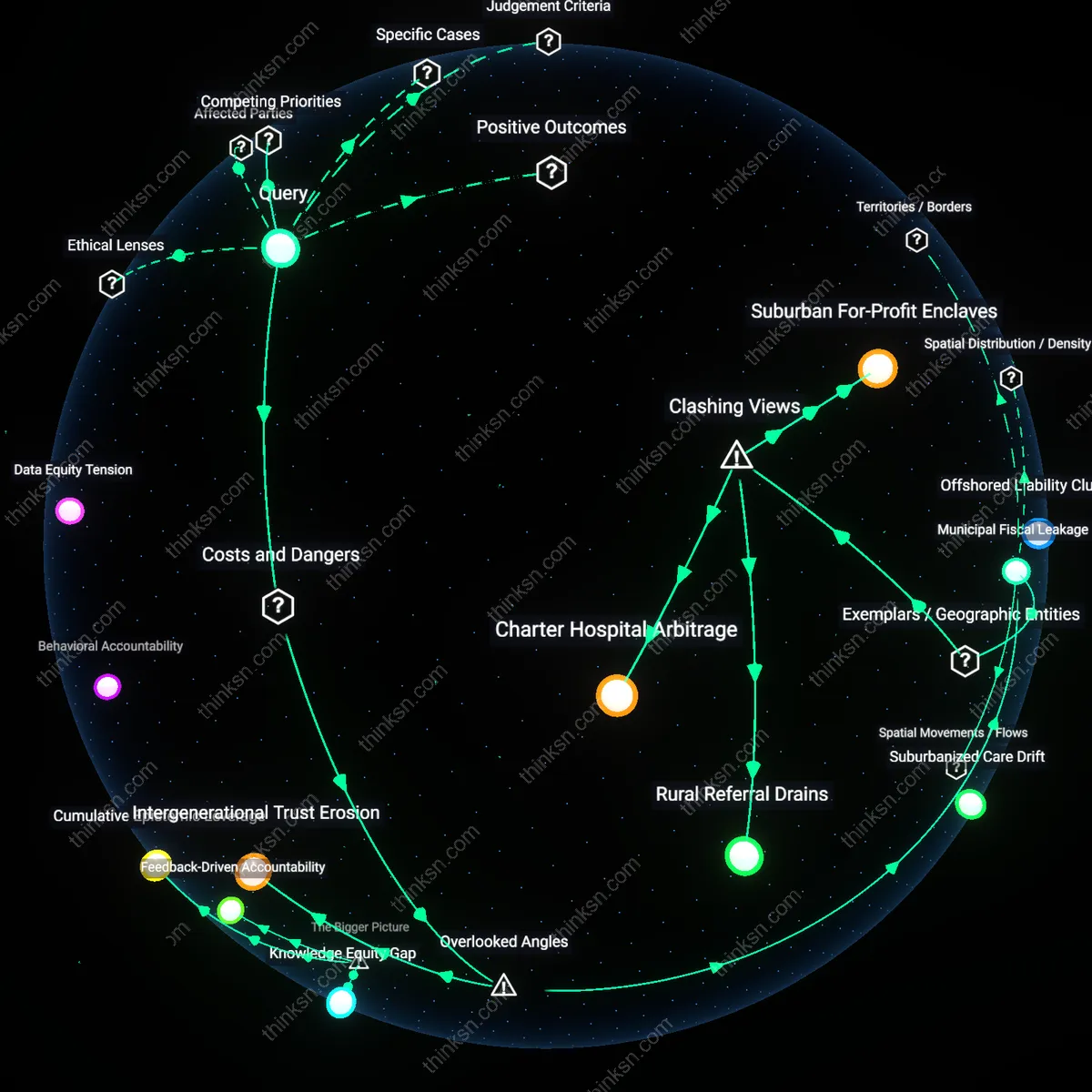
Intergenerational Care Debt
Refusing life-sustaining treatment via living will generates intergenerational care debt by shifting the burden of end-of-life monitoring and decision validation onto younger family members, who must navigate legal and medical gatekeeping to honor the document. This responsibility emerges not at death but years prior, as cognitive decline activates the will’s directives, requiring kin to perform emotional, bureaucratic, and clinical labor to enforce a decision made decades earlier—often without their input. Most ethical debates assume autonomy is self-contained, but the non-obvious reality is that advance directives create relational obligations long before death, embedding future dependents in a cascade of unacknowledged duties that strain familial systems and deplete social reserves.
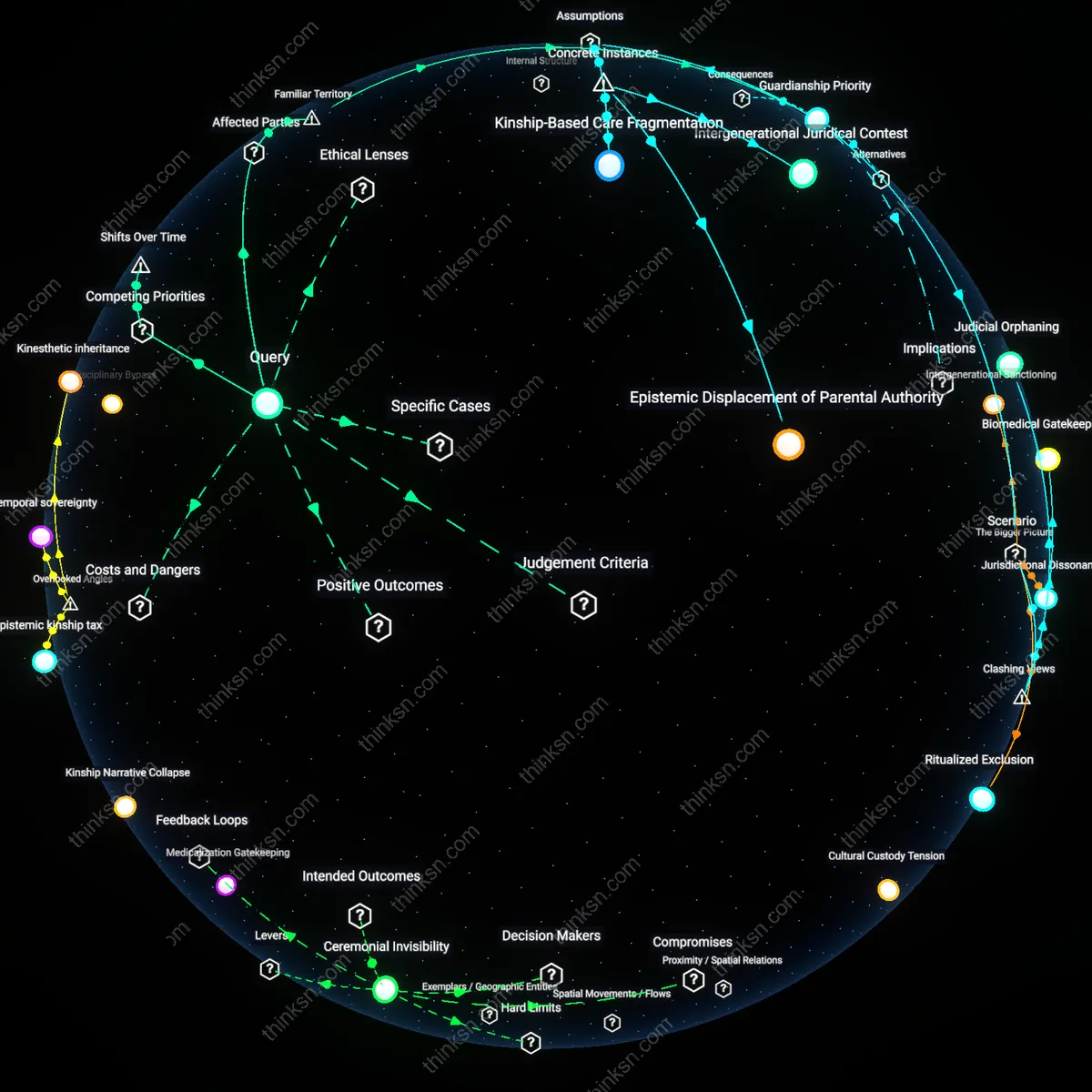
Medical Temporal Privilege
Living wills entrench medical temporal privilege by locking in treatment refusals during eras of limited therapeutic options, thereby disallowing future clinicians from applying innovations the testator could not foresee. This creates a silent veto power across time, where a person’s historical medical context overrides emergent standards of care—such as gene therapies or neural prosthetics—that could transform previously fatal or degenerative conditions into manageable ones. The underappreciated mechanism is not the will’s clarity but its immutability in a system where knowledge evolves asymmetrically; this rigidity risks preserving outdated prognostic fears and underestimating future clinicians’ capacity to restore agency, thus privileging past judgment over future possibility in ways that are ethically inert but dynamically destructive.
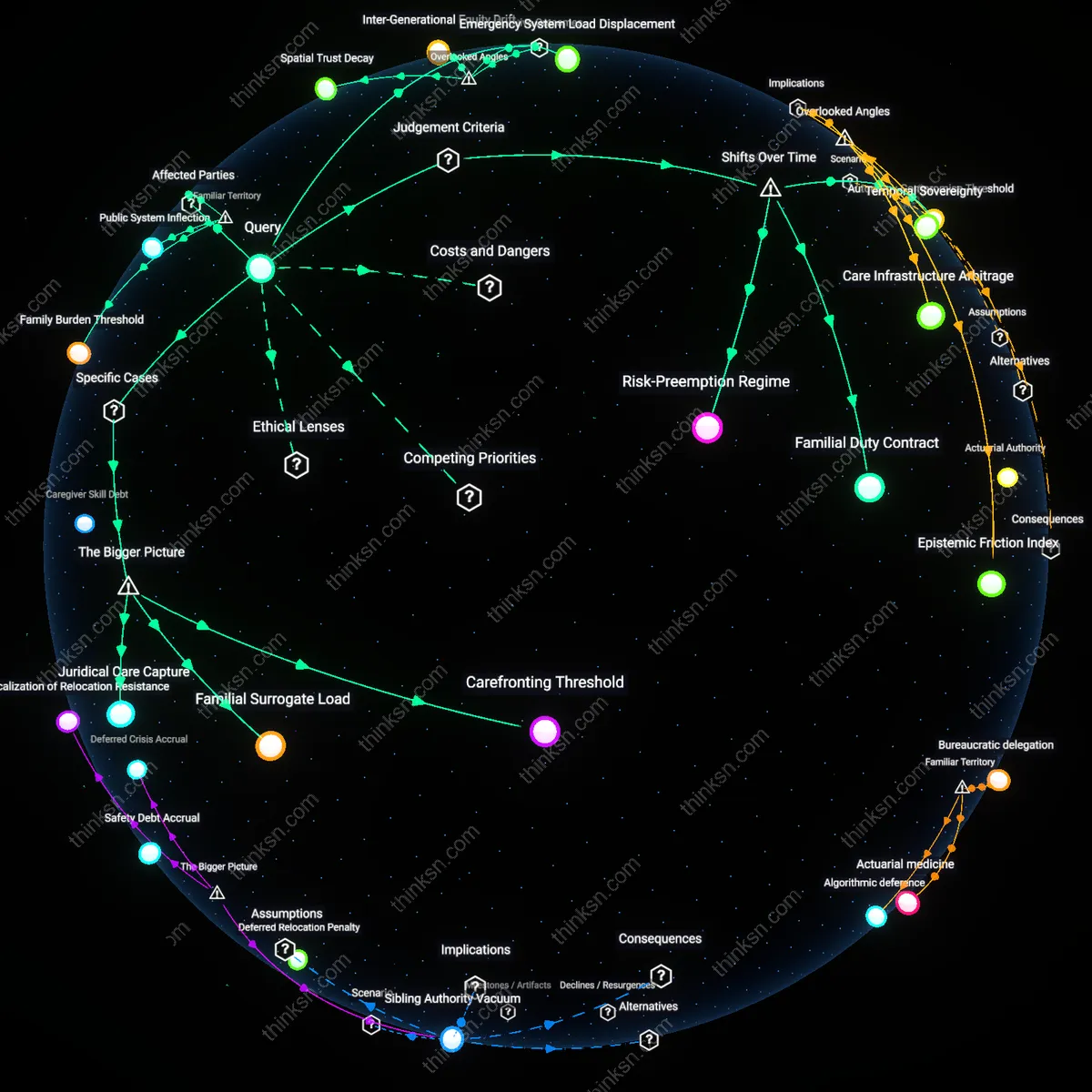
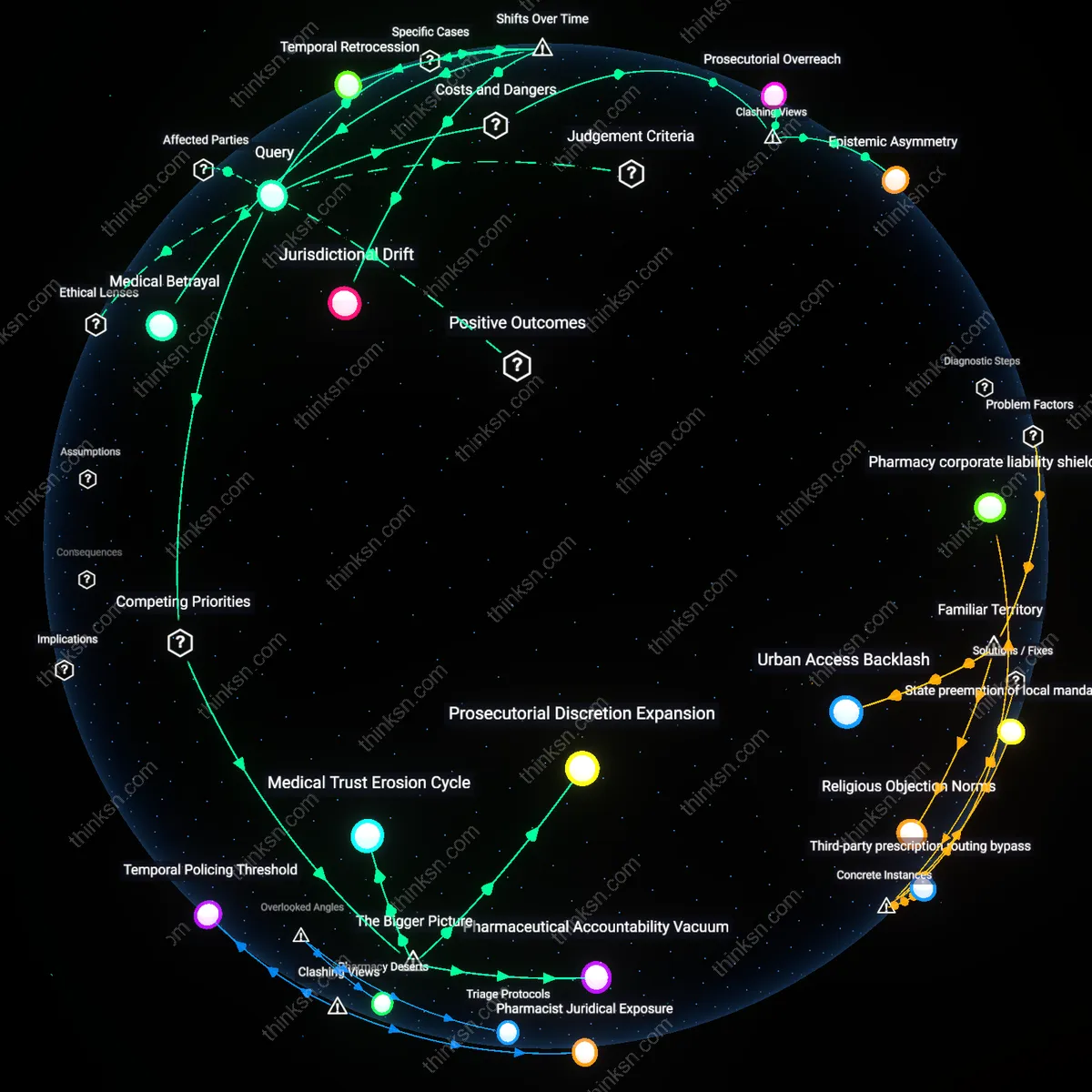
Institutional Memory Asymmetry
Hospitals and legal systems bear hidden costs from living wills due to institutional memory asymmetry—the gap between the individual’s documented intent and the organization’s need to verify, re-verify, and coordinate that intent across shifting staff and electronic health records over decades. A directive written in 1995 may resurface in 2040 during a crisis, but no clinician or administrator bears direct responsibility for its maintenance, leading to delays, defensive medicine, or override under ambiguity. The overlooked dynamic is that living wills export personal ethical risk onto fractured institutional ecosystems that lack longitudinal accountability, turning a private choice into a systemic liability with real consequences for patient safety and care efficiency.
Autonomy Primacy
A competent individual’s legally binding advance directive to refuse life-sustaining treatment is ethically justified under deontological ethics because it upholds the principle of respect for autonomy, as demonstrated by the U.S. Supreme Court’s recognition of the right to refuse treatment in Cruzan v. Director, Missouri Department of Health (1990), where the Court affirmed that refusing medical intervention constitutes a constitutionally protected liberty interest; this case reveals that even in the face of potential future improvements in quality of life, a person’s prior self-determined choice is institutionally privileged over state interests in preserving life, underscoring a normative commitment to self-governance in medical decision-making that resists paternalistic override.
Epistemic Humility
The refusal of life-sustaining treatment via a living will is ethically defensible because future medical advances are inherently unpredictable and cannot serve as a moral basis for overriding current autonomous decisions, as evidenced by the trajectory of Alzheimer’s research since the early 2000s, where decades of anticipated breakthroughs failed to yield transformative therapies despite significant investment and optimism, revealing that expectations of future quality-of-life restoration often rest on speculative assumptions rather than reproducible medical progress, making current autonomy a more reliable ethical anchor than uncertain prognoses.
Dignity Preservation
In the Netherlands, where advance directives are integrated into end-of-life care protocols under the Termination of Life on Request and Assisted Suicide (Review Procedures) Act (2002), individuals’ refusals of future life-sustaining interventions are honored even when emerging treatments might delay death, because the ethical framework prioritizes the preservation of a foreseen loss of personal dignity over mere biological survival, as illustrated by the 2016 case of a dementia patient whose directive was upheld despite familial and clinical hopes for neurological stabilization, exposing a commitment to experiential continuity rather than life extension.