When More Coverage Costs You Less Protection?
Analysis reveals 6 key thematic connections.
Key Findings
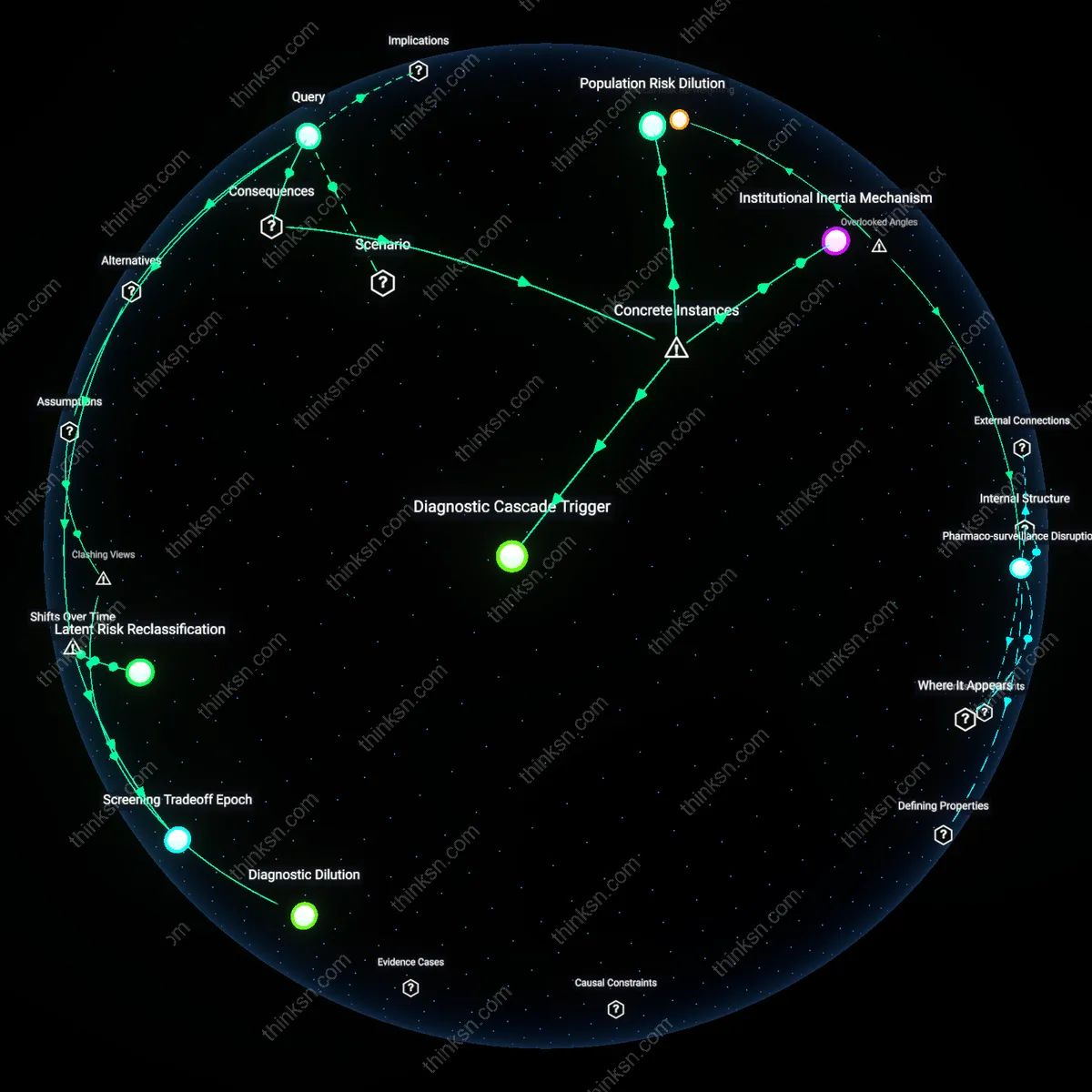
Moral hazard threshold
Raising the out-of-pocket maximum stops improving financial protection when the cost burden shifts from infrequent users to insurers, dissuading healthy individuals from cost-conscious care use. This occurs because high deductibles and low maximums already insulate the insurer after a threshold, making further increases in the cap irrelevant for those who rarely access care; the real financial risk they face is not catastrophic bills but overconsumption incentives due to prepaid coverage. The non-obvious element is that financial protection isn’t eroded by the cap level alone, but by how much the structure encourages unnecessary utilization, which redistributes risk inefficiently across the risk pool.
Actuarial irrelevance point
Financial protection ceases to improve when the out-of-pocket maximum exceeds the 99th percentile of actual medical spending, rendering higher caps invisible to nearly all enrollees, including rare users. Insurance functions on pooled risk where maximums are set based on predicted extreme but plausible use; once the cap surpasses historically observed high-cost cases, raising it further only affects theoretical, not real, financial exposure. The underappreciated insight is that rare users aren't protected by ever-higher caps because their protection comes from coverage of unpredictable catastrophes, not incremental increases beyond what medical reality justifies.
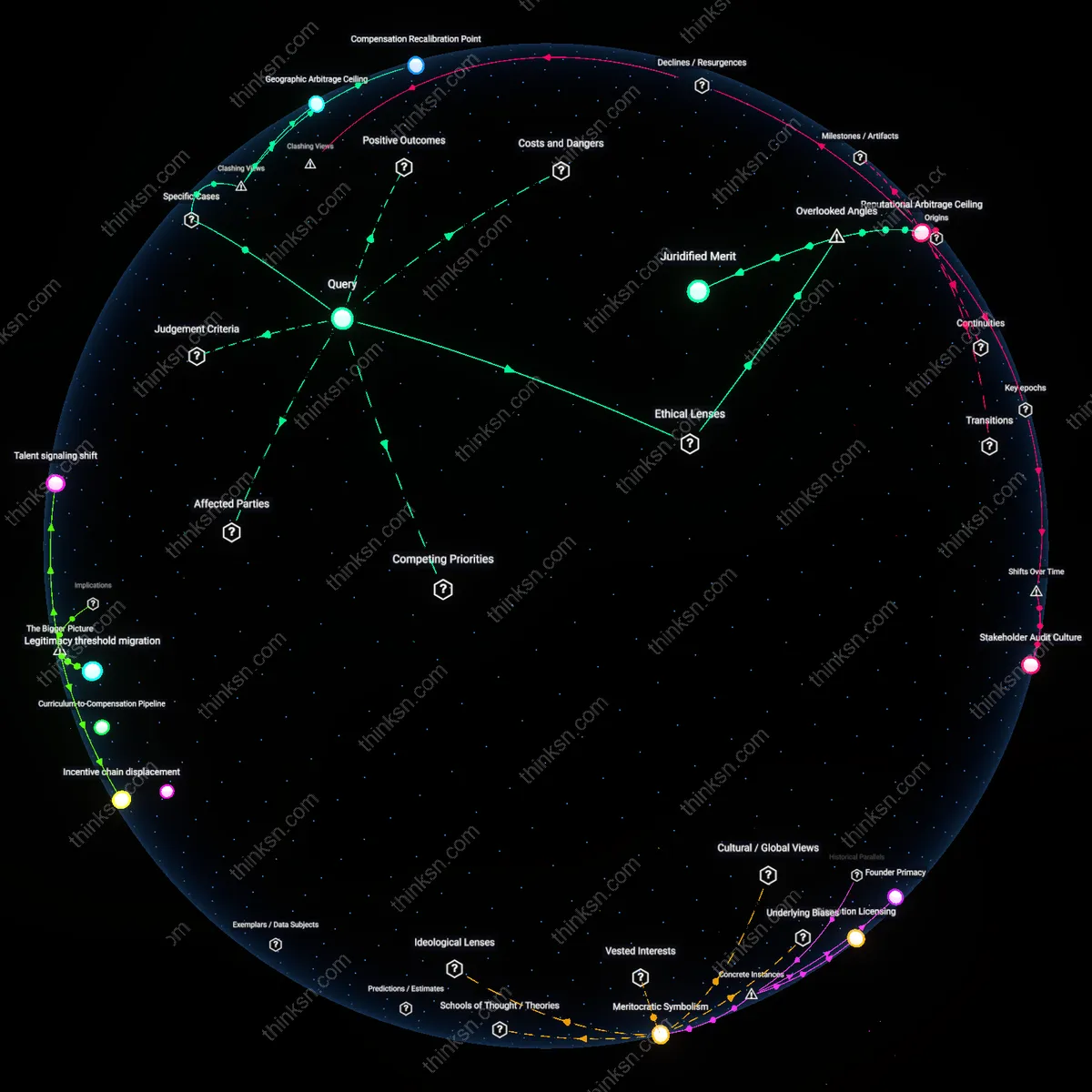
Perceived fairness boundary
The out-of-pocket maximum stops enhancing financial protection when public trust in insurance erodes due to visible cost-shifting, even if actuarially justified. When caps rise markedly without corresponding benefit increases, infrequent users interpret the system as prioritizing insurer stability over personal security, weakening the social contract of shared risk. The non-obvious factor here is that financial protection isn’t solely economic—it depends on whether people feel the system is fair, and that perception hinges on visible limits that anchor expectations, regardless of statistical likelihood of needing them.
Insurance Design Blindspot
Raising the out-of-pocket maximum fails to improve financial protection for low-users when plan design inflates cost-sharing for routine access, as seen with high-deductible health plans tied to health savings accounts in the U.S. commercial market; insurers, employers, and policymakers assume that catastrophic protection suffices for infrequent users, but this ignores how elevated deductibles—often exceeding $3,000 annually—discourage early care even among those who might eventually need complex treatment, embedding a structural neglect of preventive engagement into risk pooling; this reveals an underappreciated misalignment between financial protection metrics and behavioral health economics, privileging actuarial thresholds over real-world utilization triggers.
Actuarial Irrelevance Threshold
Once the out-of-pocket maximum exceeds the typical annual spending of low-utilizers, further increases confer no meaningful financial benefit, as observed in Medicare Advantage plans where enrollees with chronic conditions but stable care patterns face nominal caps around $7,500 yet rarely surpass $2,000 in actual expenses; the cap's level becomes symbolically protective rather than functionally relevant because risk models prioritize worst-case scenarios over distributional usage patterns, enabling regulators and payers to inflate caps without accountability for decoupling from actual patient exposure; this reflects how performance metrics anchored on extreme events obscure marginal utility in risk protection, privileging system stability over equity in cost predictability.
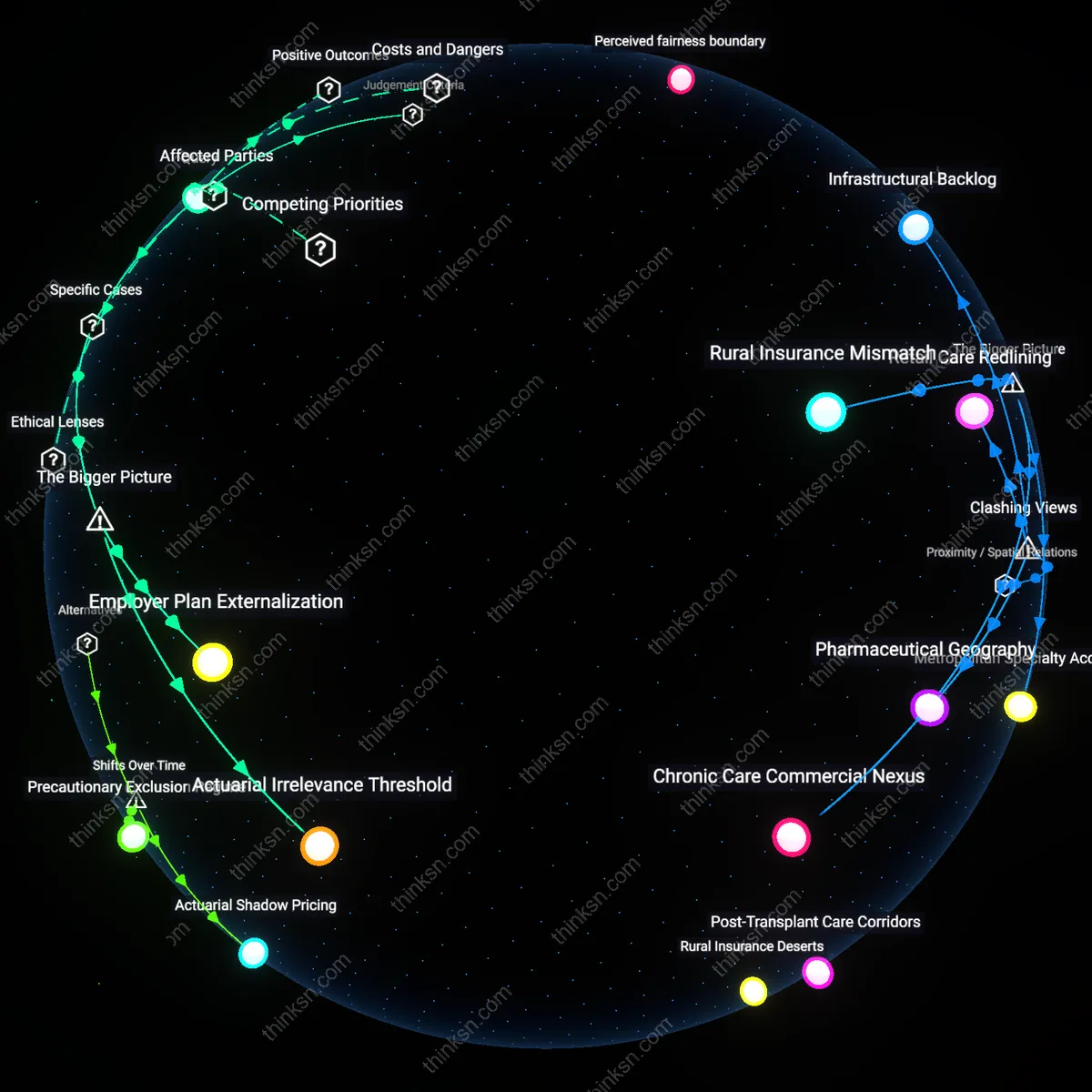
Employer Plan Externalization
In self-insured employer-sponsored plans—common among large U.S. firms like Walmart or Union Pacific—raising the out-of-pocket maximum has diminishing returns on financial protection for low-users because employers use high caps to suppress premium contributions while shifting administrative risk to employees through network restrictions and prior authorization, not just cost; these employers treat the maximum as a compliance floor rather than a floor for security, exploiting regulatory allowances under ERISA to minimize liability without improving access, which reveals how corporate benefit design treats financial protection as a legal minimum rather than a health outcome, offloading behavioral and informational burdens onto workers who don’t anticipate care needs until they arise.