Immunotherapy resistance inflection
Treatment breaks during melanoma therapy with ipilimumab show elevated tumor progression rates within six weeks of interruption, as observed in the 2011 Bristol-Myers Squibb phase III trial (MDX010-20), because cytotoxic T-cell activation requires continuous antigen exposure, and pauses disrupt the inflammatory cascade necessary for tumor lysis; this reveals that immunological memory engagement in checkpoint inhibition is not self-sustaining after withdrawal, a non-obvious contrast to chemotherapy’s cumulative toxicity model.
Toxicity adaptation threshold
In the UK INTERGROUP trial for metastatic renal cell carcinoma using sunitinib, dose interruptions beyond 14 days correlated with sudden grade 3 hypertension or hand-foot syndrome upon reintroduction, because sustained VEGF inhibition alters capillary endothelial integrity, and treatment breaks permit vascular regrowth that resets drug sensitivity; this demonstrates that side-effect severity can paradoxically increase post-hiatus due to physiological recalibration, challenging the assumption that breaks universally mitigate toxicity.
Response trajectory discontinuity
During the 2005 IDEAL-1 trial of gefitinib in non-small cell lung cancer, patients with EGFR-mutant tumors who paused treatment due to rash or diarrhea showed accelerated radiographic progression within eight days, as drug-concentration troughs permitted survival signaling via PI3K/AKT rebound; this illustrates that molecularly targeted therapies impose continuous evolutionary pressure, and interruptions create permissive windows for clonal expansion, an underappreciated dynamic in precision oncology timelines.
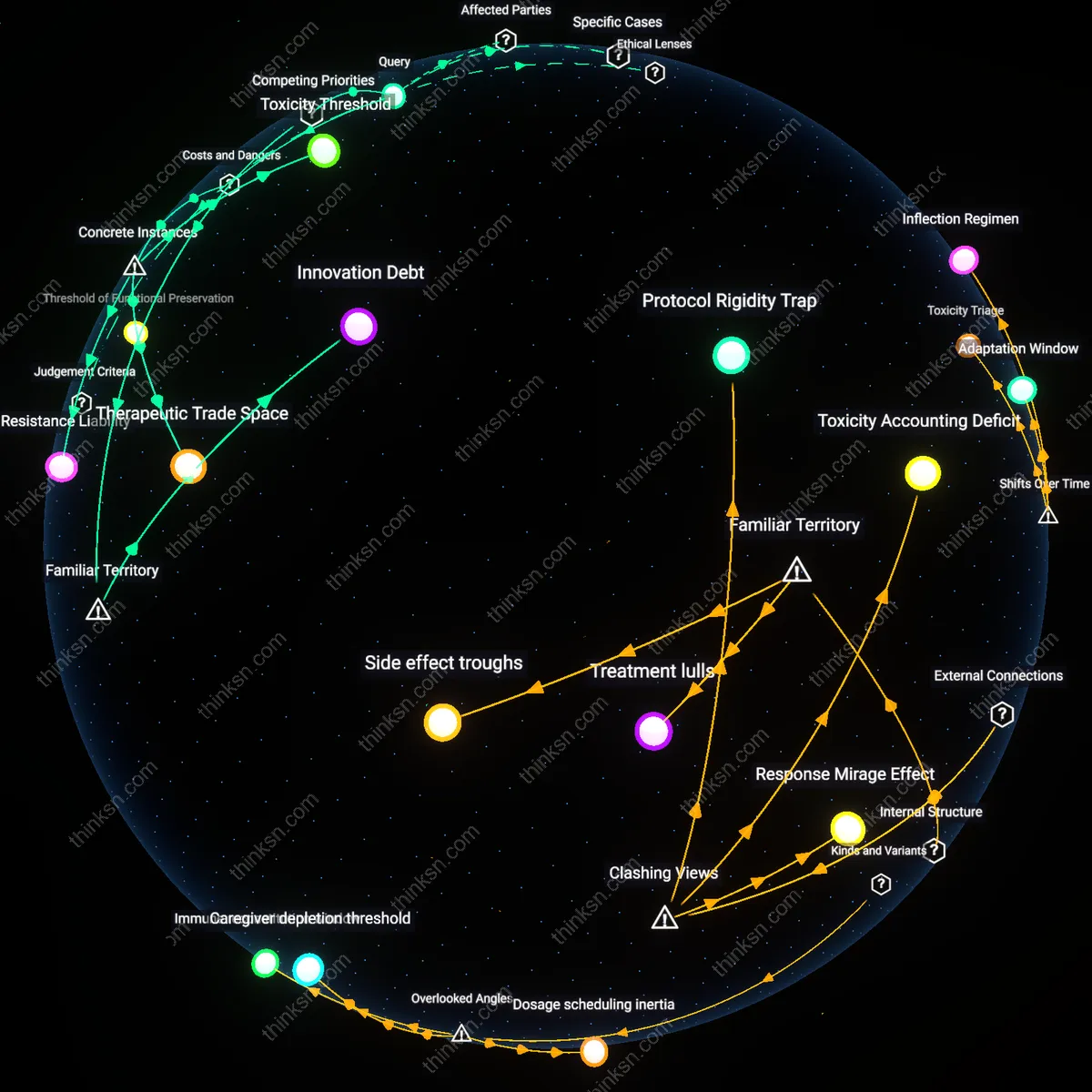
Treatment lulls
Treatment breaks show up most clearly during the intervals between chemotherapy cycles in infusion center schedules, where clinical protocols deliberately pause dosing to allow bone marrow recovery. These gaps are institutionally timed—typically every 3 to 4 weeks—and are operationally visible in appointment logs and drug ordering patterns, reflecting hematological constraints rather than tumor dynamics. What’s underappreciated is that these breaks, though framed as recovery periods, often coincide with delayed tumor rebound, not sustained response, because the public assumes treatment continuity drives efficacy, when in fact the cyclical absence is when resistance can silently emerge.
Side effect troughs
Treatment breaks are most evident when patient-reported symptom burden drops sharply after the cessation of checkpoint inhibitor infusions, particularly in melanoma regimens where steroid use subsides and fatigue lifts within days. These pauses align with immunological settling periods, when immune-related adverse events like colitis or hepatitis begin to resolve due to the withdrawal of systemic T-cell activation. The non-obvious insight is that side effect relief—not tumor shrinkage—is often the first tangible signal patients associate with therapeutic pause, reinforcing the public’s intuitive equation of symptom abatement with treatment success, even when tumor activity may be increasing.
Protocol Rigidity Trap
Treatment breaks appear most clearly during fixed-cycle chemotherapy regimens, not at points of clinical deterioration, revealing that institutional scheduling protocols override real-time patient response data in determining therapy continuity. Oncology clinics prioritize adherence to trial-validated timelines—such as day-21 restarts in FOLFOX cycles—over dynamic assessments of tumor markers or toxicity, embedding inflexibility into care pathways. This creates a system where administrative rhythm governs therapeutic pause far more than biological signal, a dissonance that undermines the assumption that treatment gaps reflect clinical recalibration. The non-obvious insight is that breaks are often preprogrammed, not reactive, exposing how trial-derived templates dominate actual practice even when contradicted by side effect burden or early progression.
Toxicity Accounting Deficit
Treatment breaks align most sharply with cumulative grade 2 toxicities—like neuropathy or fatigue—rather than acute severe events, contradicting the dominant narrative that only life-threatening side effects drive therapy interruptions. In metastatic breast cancer protocols, oncologists routinely delay dosing when patients cross subjective thresholds of functional decline not counted in formal toxicity scales, such as persistent exhaustion impacting daily living. This reveals an informal 'toxicity accounting' system operating beneath standardized AE reporting, where unmeasured symptom clusters derail treatment outside clinical trial visibility. The break thus functions as a hidden correction mechanism, exposing a divergence between recorded adverse events and the lived symptom burden that actually governs care pacing.
Response Mirage Effect
The clearest treatment breaks emerge not after radiographic progression but during intervals of stable scan results, challenging the assumption that tumor dynamics directly regulate therapy continuity. In EGFR-mutant NSCLC patients on osimertinib, clinicians often pause treatment when scans show static disease precisely because they suspect emerging resistance before it becomes radiologically visible, using breaks as diagnostic probes. This strategic suspension turns therapeutic pause into a sensing tool, where the absence of change is interpreted as early failure, inverting the logic that only visible deterioration prompts action. The non-intuitive reality is that stability—deemed success in trial endpoints—can trigger discontinuation in practice, revealing a hidden clinical epistemology where non-response is anticipated invisibly.
Dosage scheduling inertia
Treatment breaks appear most clearly between the second and third cycles of platinum-based chemotherapy regimens, where cumulative neurotoxicity from agents like oxaliplatin triggers protocol-mandated pauses; this gap aligns less with actual tumor volume changes than with institutional adherence to phase III trial-derived administration schedules that prioritize fixed intervals over response-adapted timelines. The mechanism operates through oncology pharmacy workflows, which lock in dosing calendars at cycle initiation, making mid-course adjustments administratively invisible despite emerging side effects — a dynamic rarely factored into response modeling. This reveals that treatment pauses are often artifacts of scheduling rigidity rather than clinical dynamics, shifting interpretation of 'response lag' from biological to bureaucratic origins.
Immune reconstitution window
The most pronounced treatment breaks occur after completion of induction immunotherapy in melanoma patients receiving anti-PD-1 agents, specifically during the six- to eight-week interval post-cycle four, where radiographic pseudoprogression precedes clinical deterioration, prompting clinicians to pause rather than escalate. This pause coincides not with tumor growth but with delayed T-cell infiltration that mimics progression on CT scans, forcing risk-averse holds until biopsy or PET confirmation. The overlooked mechanism is the temporal disjunction between immune activation kinetics and radiological assessment conventions, which assume monotonic tumor shrinkage — a mismatch that distorts the perceived efficacy timeline and causes avoidable discontinuation. This uncovers a hidden dependency on imaging interpretation latency shaping break patterns more than either toxicity or true progression.
Caregiver depletion threshold
Treatment breaks cluster most densely during the fifth to seventh weeks of concurrent chemoradiation for locally advanced lung cancer, corresponding not to nadir blood counts or peak mucosal injury but to the point at which informal caregivers — typically spouses managing transportation, medication, and symptom logs — exhibit measurable withdrawal due to cumulative strain. Oncology teams interpret missed appointments as patient intolerance, but ethnographic data show caregivers are the actual rate-limiting factor, halting treatment when emotional and logistical reserves are exhausted. This reveals that side effect burden is socially mediated, with therapy continuity depending on an unscheduled, unpaid labor ecosystem absent from clinical protocols — a hidden dependency that reframes treatment breaks as relational collapses rather than biomedical events.
Inflection Regimen
Treatment breaks in metastatic melanoma patients on BRAF/MEK inhibitors became most visible at six months into therapy in clinics across Memorial Sloan Kettering and Sydney’s Melanoma Institute, when radiographic stabilization was misinterpreted as durability, leading oncologists to pause treatment only to see rapid rebound in tumor growth within weeks; this pattern—observed between 2014 and 2017—marked a shift from continuous suppression models to miscalibrated rest periods, revealing how transient responses were mistaken for remission under pressure to reduce toxicity, and exposing a new decision architecture where side effect relief inadvertently reset evolutionary selection pressures on tumor clones.
Toxicity Triage
In 2018 at the MD Anderson Proton Therapy Center, extended treatment breaks during chemoradiation for head and neck cancers emerged most clearly not during disease progression but in the ninth week of therapy, when cumulative mucositis drove clinicians to suspend regimens; this moment marked a structural transition from oncology-dominated decision-making to palliative co-governance, as supportive care teams gained veto power over treatment continuity, institutionalizing a new temporal rhythm where symptom accrual, not tumor imaging, dictated therapeutic pauses—making the patient’s oral epithelium the primary site of clinical inflection.
Adaptation Window
Between 2020 and 2022 at the Gustave Roussy Institute, treatment breaks in adjuvant immunotherapy for high-risk renal cell carcinoma ceased to follow fixed calendars and instead clustered around the three-month mark only when ctDNA clearance was confirmed—a shift from empiric scheduling to molecular-guided pausing that redefined response as an actionable biomarker; this pivot revealed how intermittent dosing evolved from operational necessity into strategic design, producing a new therapeutic logic where absence of evidence became evidence for absence, and remission was no longer assumed but interstitially validated.