Is Prolonged Appeal Worth Emotional Cost for Denied Physiotherapy?
Analysis reveals 4 key thematic connections.
Key Findings
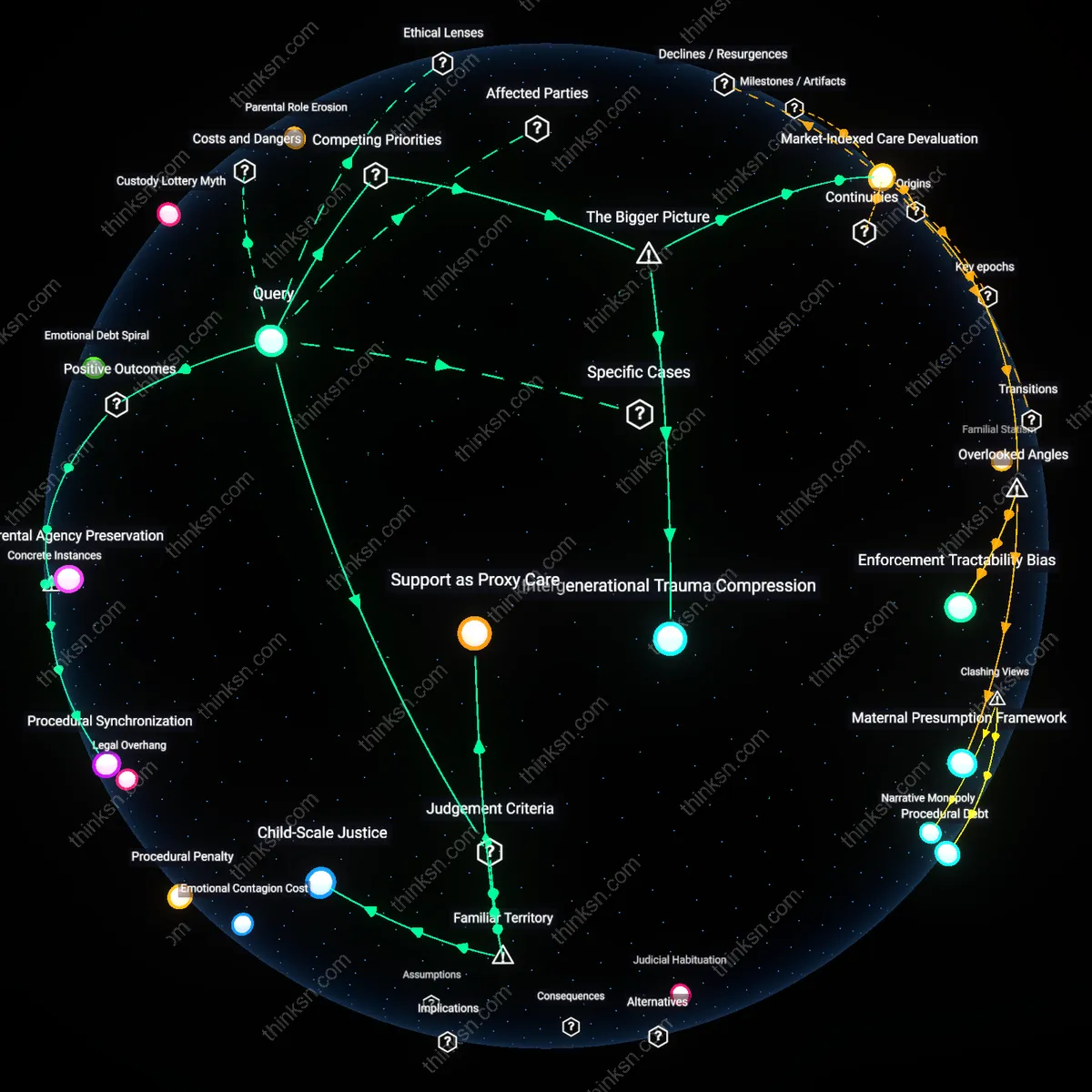
Temporal Identity Fracture
A patient can reduce emotional burden by formally designating a future self as the recipient of treatment benefits, thereby psychologically decoupling present suffering from deferred outcomes. This shift leverages legal and administrative timelines to construct a narrative in which the current self sacrifices for a distinct, anticipated identity—common in injury compensation systems where treatment access is contingent on appeals dragging over months. What’s overlooked is that the mind treats prolonged bureaucratic time not as a neutral container but as a transformer of selfhood, making present emotional costs feel less wasted if they serve a temporally distant 'other'; this reframing mitigates helplessness by converting passive waiting into active inter-self negotiation.
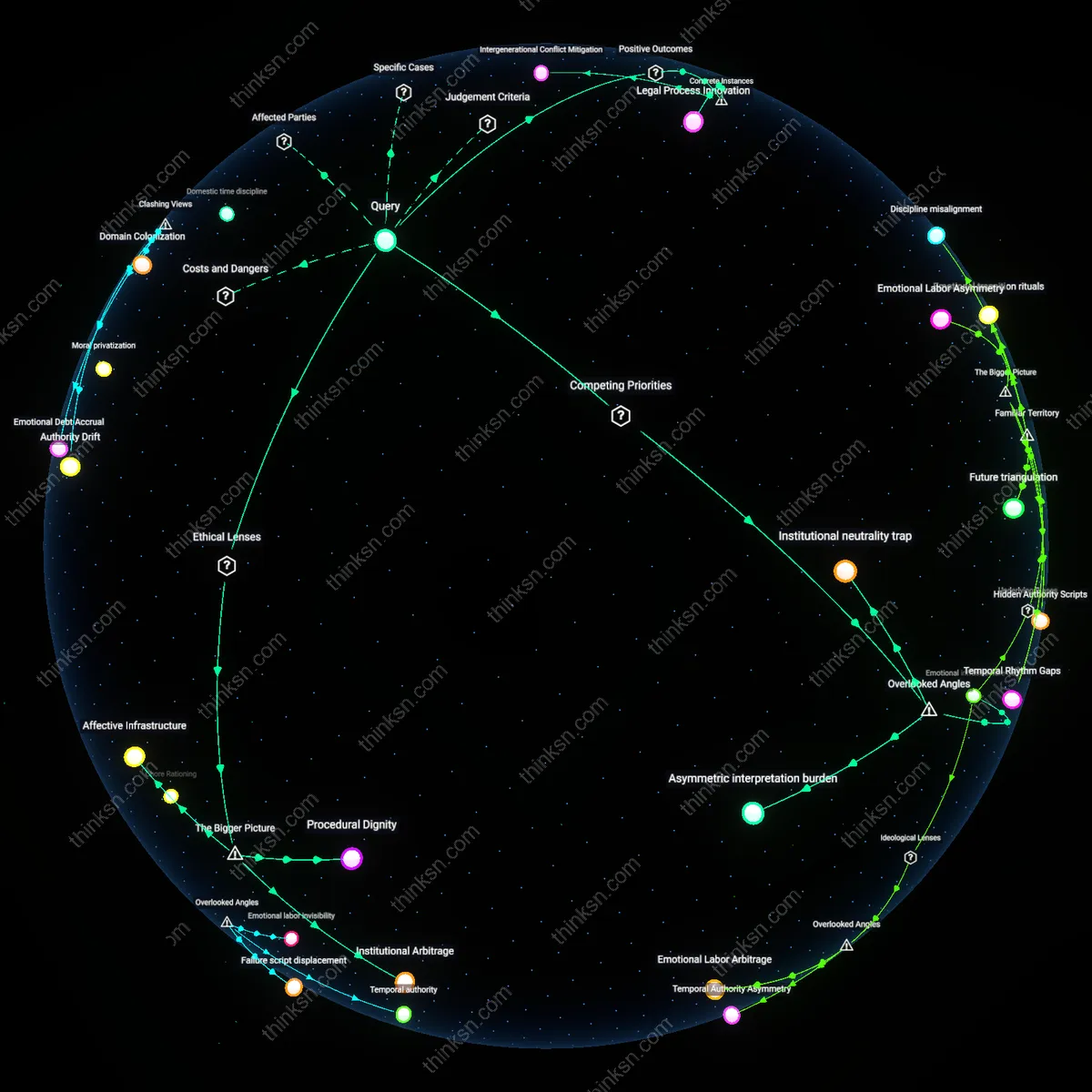
Therapeutic Suspension Debt
Initiating low-intensity, self-administered physio routines during the appeal—even if suboptimal—creates a psychological ledger where continued effort accrues moral credit toward future healing, reducing the perceived cost of bureaucratic delay. The unacknowledged dynamic is that treatment denial doesn’t just withhold care but severs the patient’s sense of therapeutic continuity, and small acts of adherence rebuild narrative cohesion between diagnosis and recovery. This matters because standard coping models assume patients must either disengage emotionally or endure constant stress, ignoring how provisional action sustains identity as an active healer rather than a passive appellant.
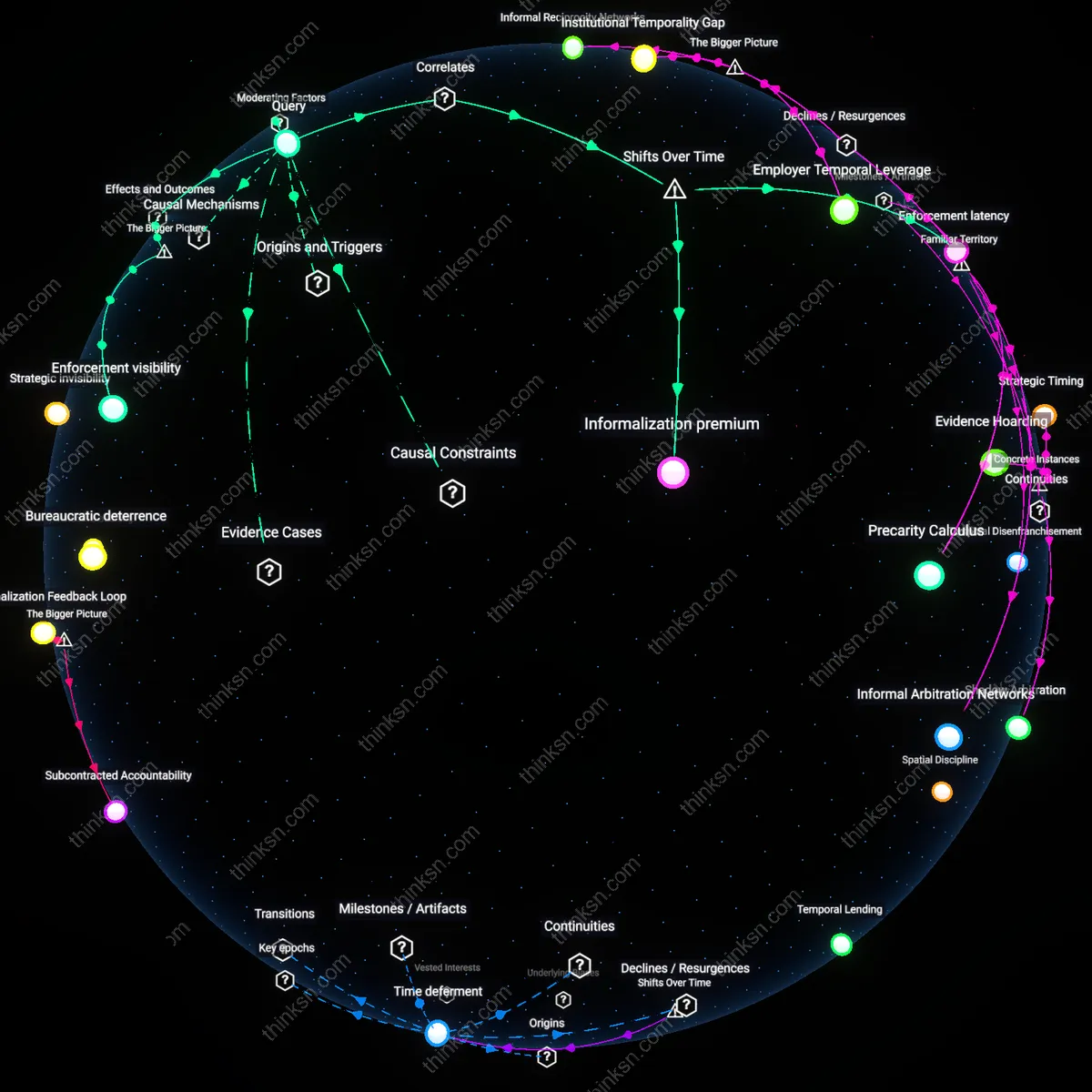
Therapeutic access arbitrage
Patients in rural Scotland who qualify for NHS-recommended physiotherapy but face appeal delays increasingly cross-subsidize private sessions using support from third-sector organizations like Chest, Heart & Stroke Scotland, creating a shadow market where charitable capacity fills clinical gaps while inadvertently legitimizing state underfunding. This dynamic persists because devolved healthcare budgets allow regional rationing to be masked as clinical prioritization, enabling policymakers to outsource moral risk to nonprofits that absorb both financial and emotional burdens. The non-obvious insight is that patient access now depends less on medical need than on the geographic density of charitable infrastructure—an uneven patchwork that turns civic altruism into a systemic reliever valve.
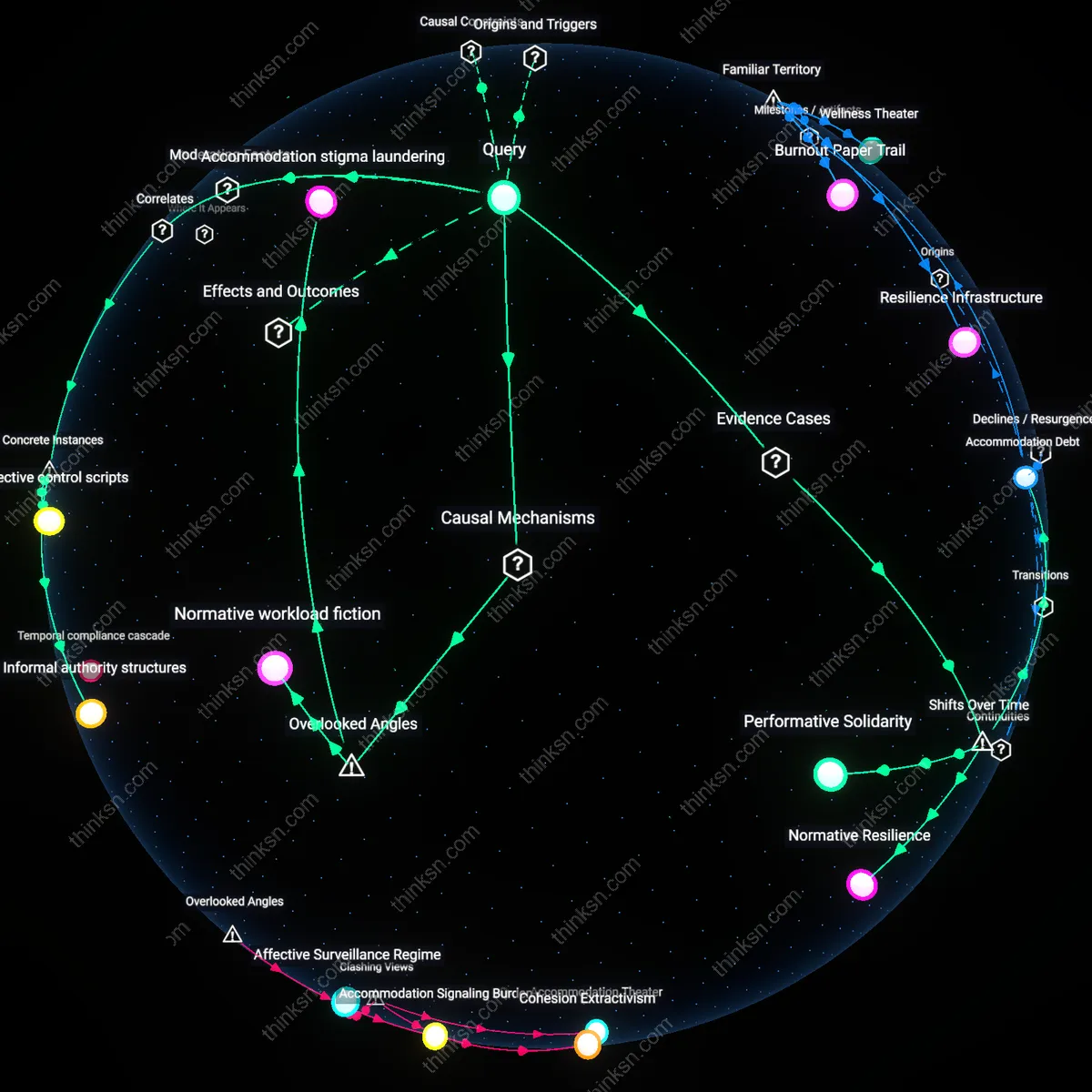
Affective labor redistribution
In Australia’s NDIS appeals process, parents of children with cerebral palsy routinely document daily mobility deterioration to strengthen their case, transforming intimate caregiving into evidentiary labor that reinforces emotional strain while being treated as administrative input by decision panels. This shift occurs because appeals rely on subjective ‘proof of deterioration’ rather than clinical eligibility, outsourcing assessment burdens to families while insulating providers from accountability for delayed intervention. The overlooked mechanism is that emotional distress becomes both a consequence of denial and a required fuel for contesting it—turning private suffering into a hidden procedural currency that sustains systemic deferral.