Is Appealing to State Commissioners Worth It for New Diabetes Drugs?
Analysis reveals 6 key thematic connections.
Key Findings
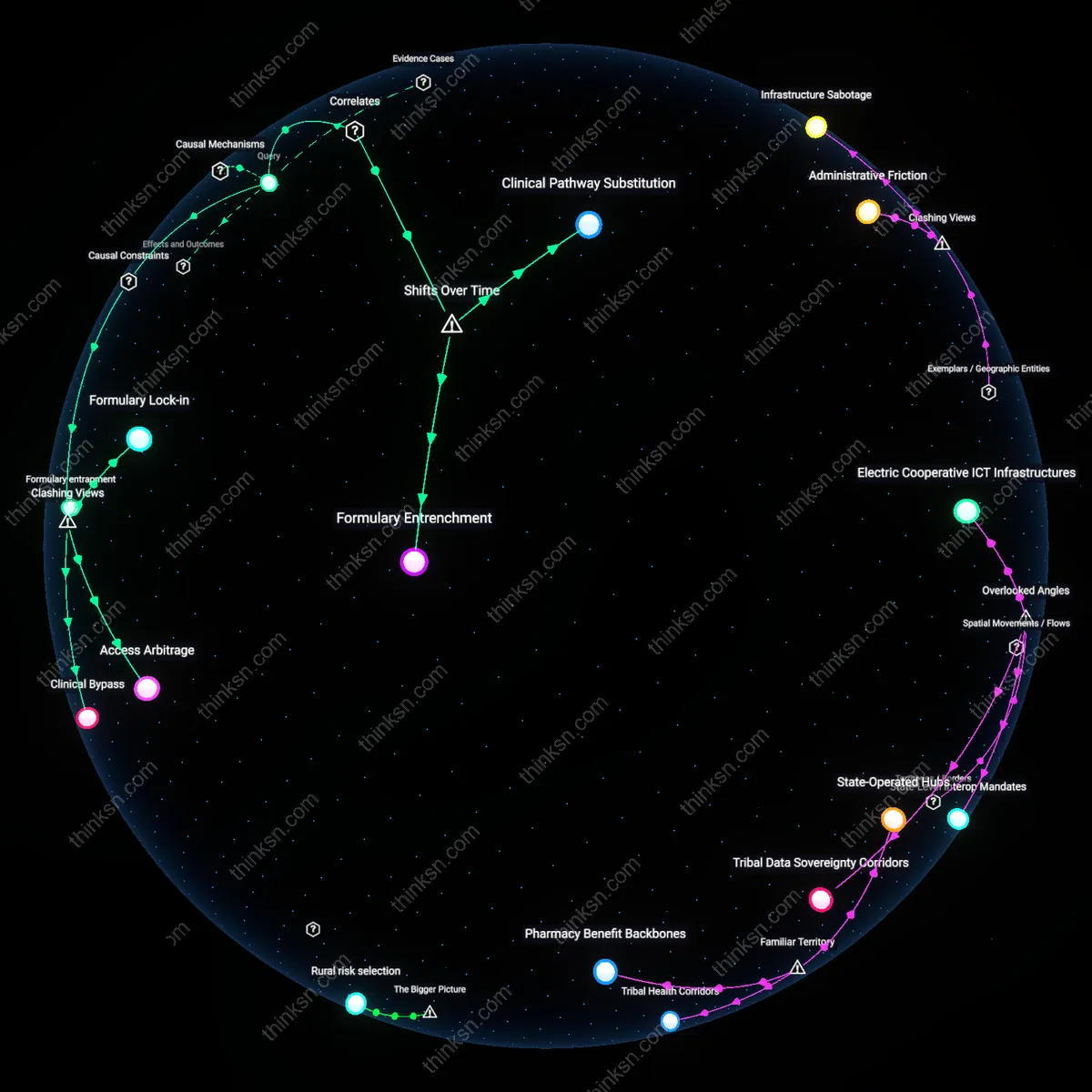
Regulatory Theater
Appealing to a state insurance commissioner is ineffective because commissioners lack enforcement authority over private formulary decisions, rendering appeals procedurally inert within the actual machinery of insurer deliberation. The process functions as a symbolic concession to patient advocacy while preserving payer autonomy, thereby draining patient energy into a bureaucratic cul-de-sac that mimics responsiveness without altering outcomes. This reveals how regulatory visibility can be manipulated to legitimize inaction, privileging systemic inertia over therapeutic access.
Clinical Bypass Risk
Appealing to a state commissioner inadvertently increases patient harm by delaying timely escalation to clinically viable alternatives, such as manufacturer patient assistance programs or therapeutic substitutions, because patients and providers mistake the appeal as a binding corrective pathway. The delay embeds administrative optimism into treatment timelines, where the belief in systemic redress postpones adaptive action, turning procedural engagement into a vector of therapeutic lag with measurable glycemic consequences.
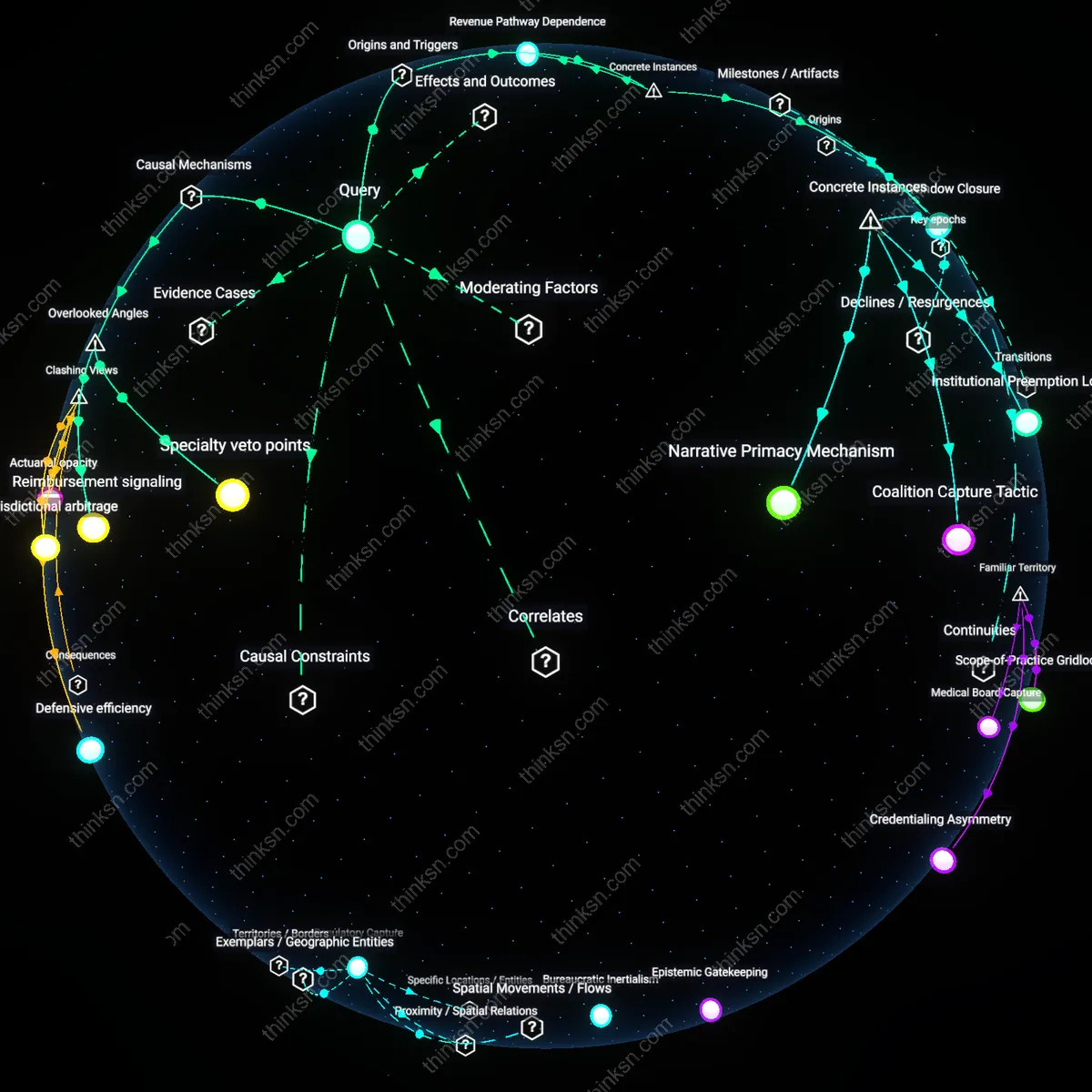
Asymmetric Accountability
The appeal process strengthens insurer control by codifying patient grievances as isolated incidents rather than patterns of exclusion, allowing payers to absorb complaints without reforming formulary design, since commissioners compile data without public disclosure or mandatory intervention thresholds. This transforms individual appeals into surveillance inputs that refine risk-based denial strategies, effectively weaponizing patient engagement to optimize cost containment under regulatory camouflage.
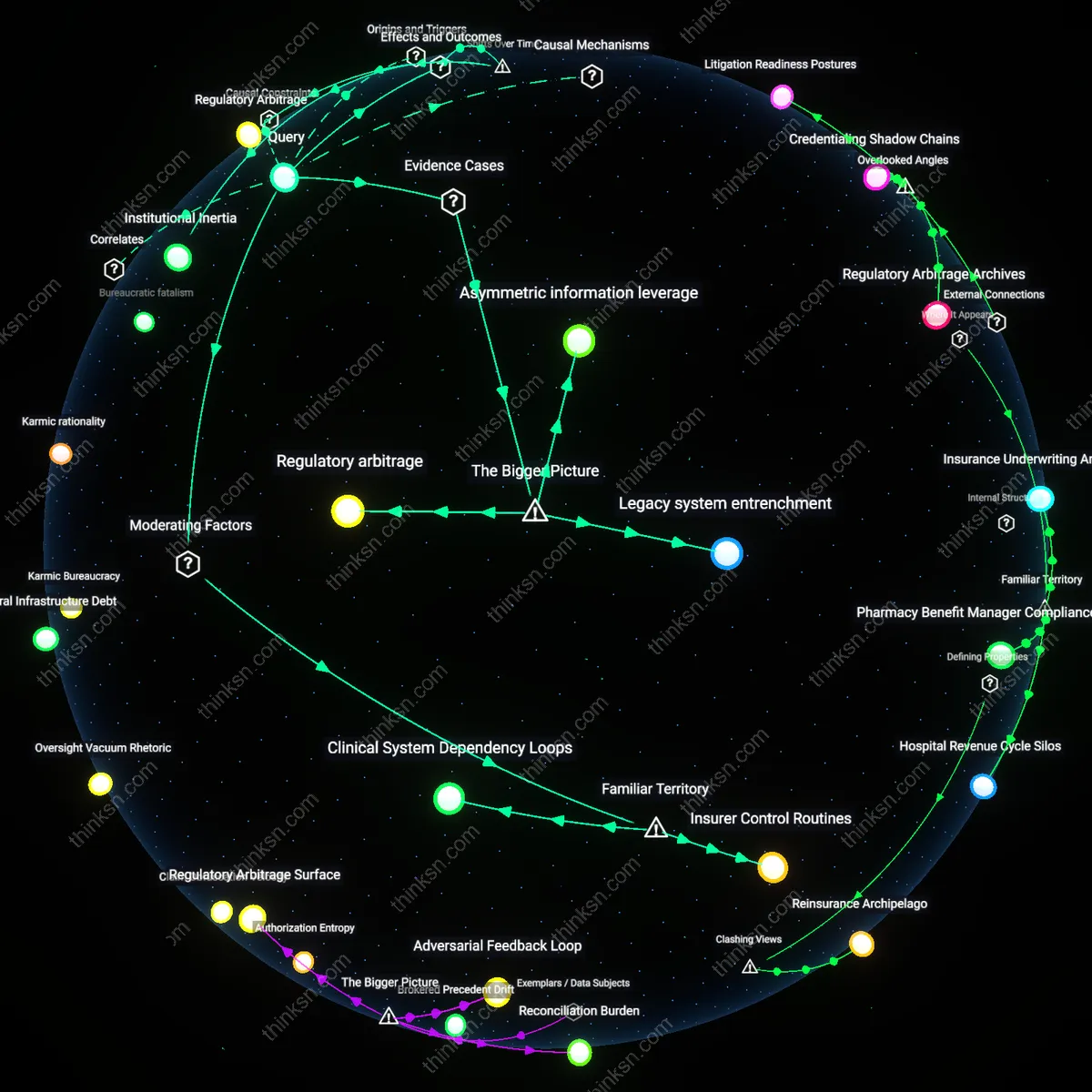
Regulatory Arbitrage
Appealing to a state insurance commissioner can effectively compel coverage of an excluded diabetes drug when patient advocacy leverages statutory authority under state-mandated formulary appeal processes, as demonstrated in Massachusetts in 2017 when Commissioner Gloria Schaffer upheld a patient's appeal for coverage of Tresiba under Chapter 224’s drug cost transparency law, activating a rarely used mechanism that forced MassHealth to revise its formulary justification—revealing that commissioners can serve as operational, rather than symbolic, gatekeepers where statutory frameworks mandate clinical review, a function often overlooked in federalist debates over insurance regulation.
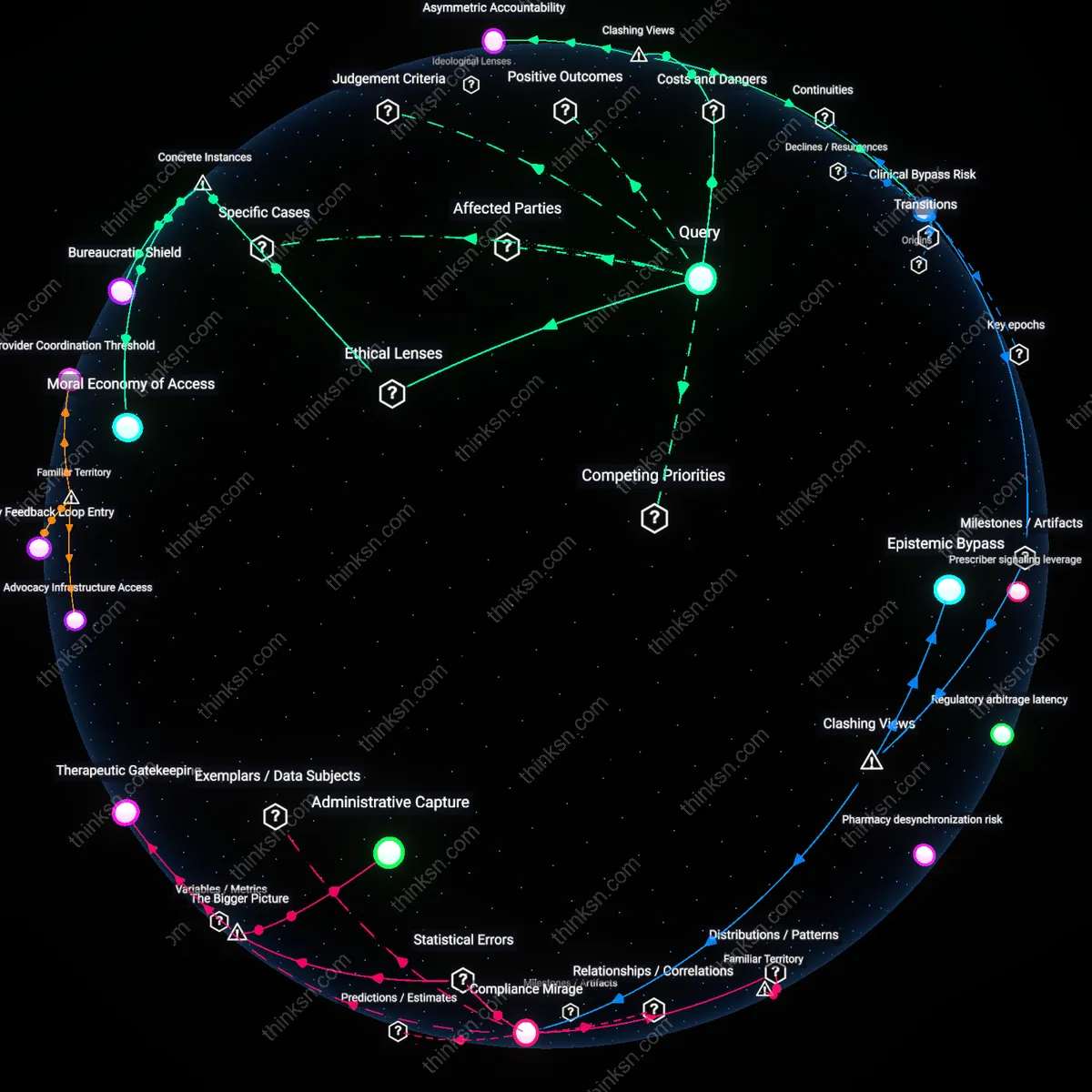
Moral Economy of Access
In New Mexico in 2020, a collective patient campaign targeting Insurance Commissioner Eric R. Fruchtenicht successfully reversed the exclusion of inhaled insulin Afrezza from Medicaid’s formulary by framing non-coverage as a distributive injustice under the state’s medical necessity doctrine, grounding appeal in a community moral claim that diabetes care is a baseline entitlement—demonstrating that commissioner appeals gain traction not through legal technicalities alone, but when embedded in a broader populist narrative of fairness, revealing the underappreciated role of moral discourse in shaping administrative enforcement priorities.
Bureaucratic Shield
In Florida in 2019, dozens of appeals to Insurance Commissioner David H. Schillinger to cover SGLT2 inhibitors for type 2 diabetics were systematically dismissed despite clinical evidence, because formulary decisions were legally delegated to private pharmacy benefit managers under Senate Bill 1702, exposing that commissioner power is intentionally structurally disabled in favor of managed care autonomy, making appeals symbolic rituals that preserve procedural appearance without altering outcomes—a function often masked by nominal patient rights frameworks.