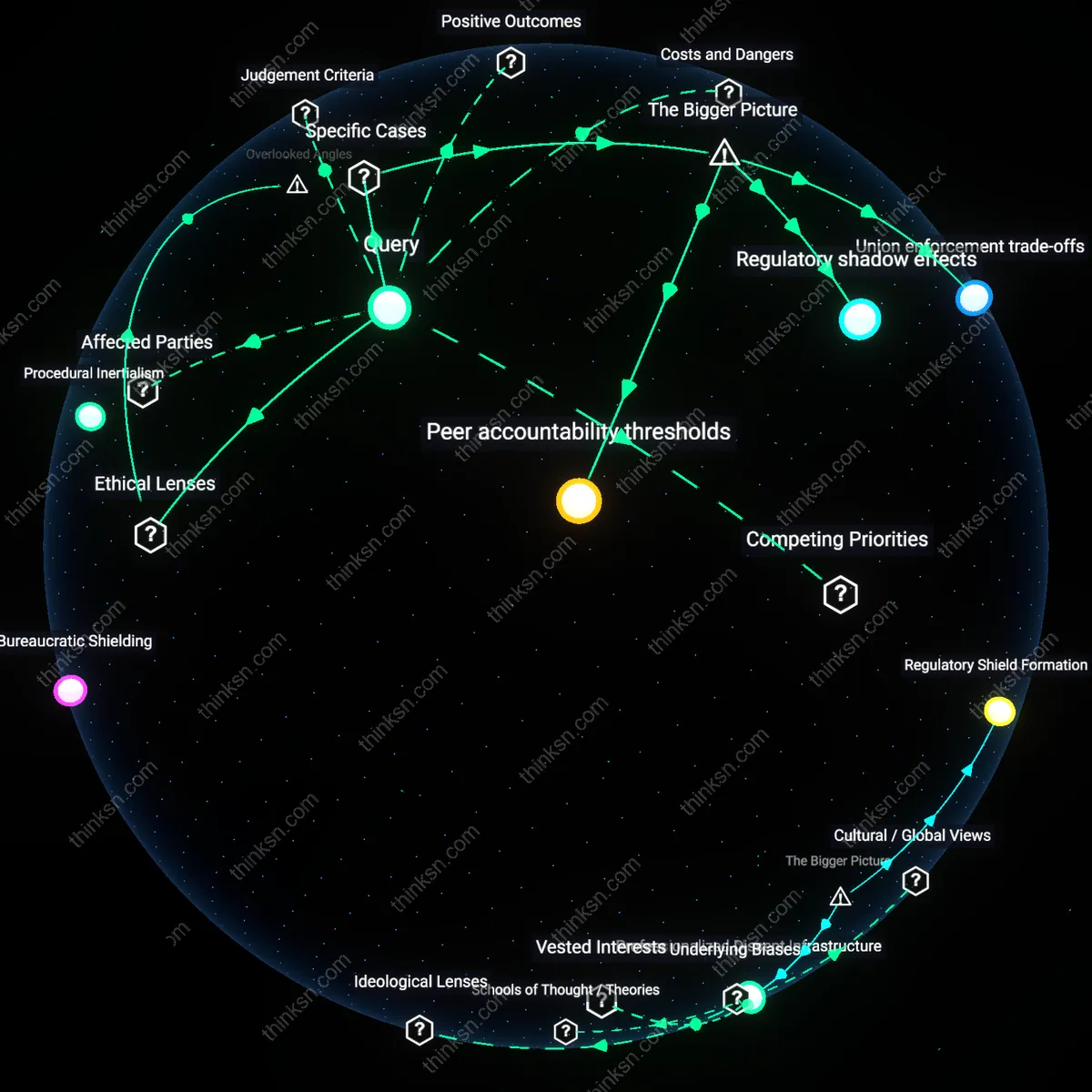
Regulatory Shield Formation
The shift from individual whistleblowing to contractual grievance procedures in unionized healthcare settings began in the late 1970s within U.S. public hospitals, where rising malpractice litigation and federal patient safety mandates incentivized institutional risk management; unions negotiated grievance clauses as liability-limiting mechanisms, transforming whistleblower vulnerability into procedurally shielded reporting through collective bargaining agreements. This change was driven by hospital administrators and union representatives jointly seeking to insulate both workers and institutions from legal exposure, embedding formalized complaints within enforceable labor contracts rather than relying on ad hoc moral courage. The non-obvious consequence is that safety reporting became depoliticized—individual ethical outrage was absorbed into bureaucratic channels, reducing retaliatory risks but also narrowing the scope of what could be challenged.
Bureaucratic Containment Logic
The transition accelerated in the 1990s as accreditation bodies like The Joint Commission mandated internal incident reporting systems, which were then fused with union grievance infrastructures in facilities such as Kaiser Permanente, where standardized workflows subsumed individual disclosures into tiered dispute resolution ladders. This integration allowed healthcare organizations to absorb potential public scandals into private arbitration processes, managed by union stewards and HR mediators, thereby containing reputational damage and maintaining operational continuity. The underappreciated dynamic is that this system prioritized organizational stability over transparency, converting moral claims into technical disputes subject to time-bound procedures and evidentiary rules that often excluded patient testimony or systemic critique.
Professionalized Dissent Infrastructure
Beginning in the early 2000s, especially in Canadian provincial health systems like Ontario’s, the formalization of clinical governance frameworks led unions to reframe grievances as quality-of-care interventions, embedding nurse and technician concerns into routine performance reviews rather than exceptional whistleblowing events. This repositioning was enabled by cross-sector alliances between union negotiators and clinical leadership teams who jointly designed protocols that treated staff complaints as data inputs for continuous improvement, not as personal accusations. What remains overlooked is that dissent itself became professionalized—worker advocacy was preserved but only when expressed through sanctioned forms, effectively displacing individual moral agency into institutional improvement machinery.
Bureaucratic Containment
Contractual grievance procedures in unionized healthcare settings did not replace individual whistleblowing but instead absorbed and neutralized it as a political act. Through the post-1970s expansion of collective bargaining agreements in public-sector hospitals, unions negotiated formal channels for reporting safety and ethical violations—channels that redirected moral dissent into codified, hierarchical processes managed by neutral arbitrators. This shift transformed whistleblowing from a public, ethically charged rupture into a procedural step susceptible to delay, confidentiality, and institutional control, thereby depoliticizing challenges to management while preserving systemic power. The non-obvious consequence is that the very mechanisms designed to protect workers also functioned as instruments of institutional insulation against disruptive accountability.
Ethical Derailment
The migration from individual whistleblowing to contractual grievances in unionized healthcare since the 1990s actually eroded frontline clinicians’ ability to act on ethical imperatives, particularly in for-profit hospital chains where union contracts were designed in collaboration with management to prioritize labor peace over patient advocacy. Grievance procedures, while offering job protection, required violations to be framed as contractual breaches rather than ethical harms—rendering patient safety concerns actionable only if they coincided with worker conditions. This narrow framing severed moral agency from institutional redress, making it structurally difficult for nurses or technicians to escalate issues like medication errors or understaffing unless they could prove personal harm. The dissonance lies in how procedural protections, meant to empower workers, ended up circumscribing the legitimate scope of ethical speech.
Union Complicity Regime
From the 1980s onward, the institutionalization of grievance procedures in unionized healthcare settings produced a system in which unions themselves became gatekeepers who routinely suppressed individual whistleblowing to maintain negotiation leverage with hospital administrations. In settings like U.S. Veterans Health Administration facilities and large urban public hospitals, union stewards developed informal screening practices that disqualified grievances involving patient care abuse unless they met strict contractual criteria, effectively treating public-interest disclosures as secondary to labor-management stability. This created a tacit alliance between union leadership and hospital executives, where the formal grievance system operated not as a tool of worker or patient advocacy but as a mechanism for mutual risk containment. The underappreciated reality is that unionized protections, in practice, often penalized moral initiative in favor of institutional predictability.
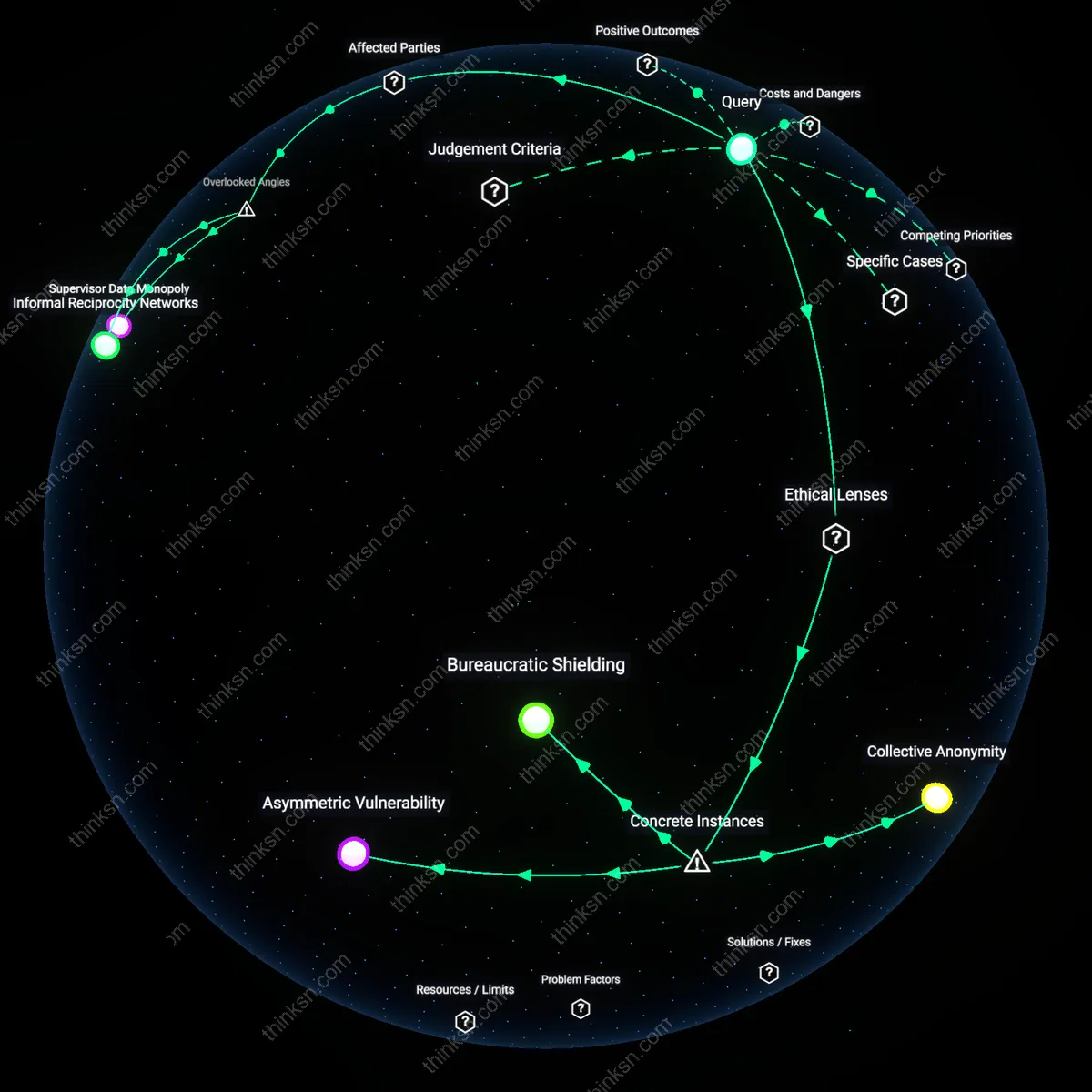
Bureaucratic Shielding
Union grievance procedures displaced individual whistleblowing by routing safety and ethics complaints through formal, contractual channels managed by shop stewards and labor representatives in hospitals like those in the Kaiser Permanente system. This shift embedded reporting within collective bargaining agreements, reducing direct worker-management confrontation but also depersonalizing moral outrage into procedural disputes, often delaying or diluting urgent disclosures. What’s underappreciated is how this familiar ‘protection’ often suppresses public revelation—precisely what whistleblowing is meant to enable—by prioritizing contractual compliance over transparency.
Procedural Inertialism
Healthcare unions such as SEIU Local 121RN institutionalized grievances as routinized, document-heavy processes requiring multiple escalations before action, transforming what was once a direct nurse-to-administrator moral appeal into a codified negotiation sequence. This shift, visible in facilities like those in the UPMC network, replaced the dramatic, media-ready moment of individual exposure with incremental backroom resolutions, embedding accountability within labor-management committees. The non-obvious consequence is that while retaliation risk drops, so does systemic visibility—problems are resolved locally but rarely generate broader institutional learning or public reform pressure.
Moral Delegation
Nurses and clinicians began assigning ethical responsibility for reporting to union representatives rather than acting as personal moral agents, a pivot evident in post-2010 grievance patterns across unionized VA hospitals. The union steward, not the frontline worker, became the recognized carrier of ethical concern, converting individual conscience into collective representation through standardized forms and union-led arbitration. What remains underrecognized is that this familiar transfer of duty—often celebrated as solidarity—can erode personal agency, making ethical action feel like a negotiated benefit rather than a professional imperative.
Institutionalized dissent
The 1999 California Nurse Association's negotiated inclusion of whistleblower protections in collective bargaining agreements with Sutter Health System established a durable mechanism by which nurses could report patient safety violations through formal grievance channels without fear of retaliation, marking a shift from individual moral courage to structured procedural recourse; this institutionalization embedded dissent as a routine operational function rather than an exceptional act, revealing how labor contracts can codify ethical agency within clinical hierarchies—a transformation often overlooked because it appears administratively mundane rather than ethically dramatic.
Contractual precarity
In 2014, home healthcare workers represented by SEIU Local 775 in Washington State exercised their contractual grievance procedure to challenge unsafe patient assignments, demonstrating that formalized channels did not eliminate risk but redistributed it into procedural delays and bureaucratic filtering; the shift to contractual mechanisms maintained continuity in worker vulnerability, exposing how grievance systems can reproduce precarity when managerial discretion persists behind neutral rules—a reality obscured by the outward appearance of procedural security.
Bargained transparency
At Kaiser Permanente facilities in Northern California after the 2009 labor-management accord between SEIU and hospital administration, safety concerns previously raised through individual whistleblower disclosures were systematically channeled into joint labor-management committees with binding dispute resolution protocols, illustrating how transparency itself became a negotiated commodity; this case reveals that the core continuity is not resistance per se but the controlled release of information, where the union’s role evolved from amplifying isolated voices to managing institutional visibility.
Bureaucratization of Voice
The shift from individual whistleblowing to contractual grievance procedures in unionized healthcare settings emerged decisively during the 1970s as collective bargaining agreements expanded in public-sector hospitals, replacing ad hoc moral appeals with codified dispute mechanisms. State-level labor reforms, particularly after the 1974 National Health Planning and Resources Development Act, incentivized formal grievance systems as substitutes for individual exposure, embedding conflict resolution within union-management committees. This transition disciplined dissent into predictable channels, reducing reputational risk for workers but also diluting the disruptive moral force of whistleblowing—what’s underappreciated is how this shift reframed ethical dissent as administrative procedure, not as a crisis of conscience but as a step in a negotiated workflow.
Contractual Substitution Effect
In the 1990s, the rise of managed care and hospital consolidation intensified cost-control regimes, prompting unions like the Service Employees International Union (SEIU) to prioritize grievance procedures that could scale across large healthcare networks, effectively displacing individual whistleblowing as the default response to patient safety concerns. Through master contracts with multi-site employers, grievances became standardized, routinized, and legally bounded—transforming whistleblower acts into enforceable breaches of contract rather than ethical revelations. The non-obvious consequence was not merely proceduralization but the strategic erasure of individual moral agency from labor advocacy, as unions traded public exposure for enforceable, but narrower, systemic corrections.
Ethical Re-domestication
Following the 2010 Affordable Care Act and the expansion of value-based care metrics, unionized healthcare institutions began reactivating individualized reporting channels within existing grievance frameworks, producing a hybrid model where whistleblowing resurfaced as a condition of regulatory compliance rather than union enforcement. Accreditation bodies like The Joint Commission mandated internal reporting systems that bypassed traditional grievance ladders, reintroducing individual moral agency—but this time under surveillance and institutional oversight. The underappreciated shift is that whistleblowing did not return as rebellion, but as a domesticated function of quality assurance, revealing how ethical resurgence in labor settings can be co-opted by administrative governance.