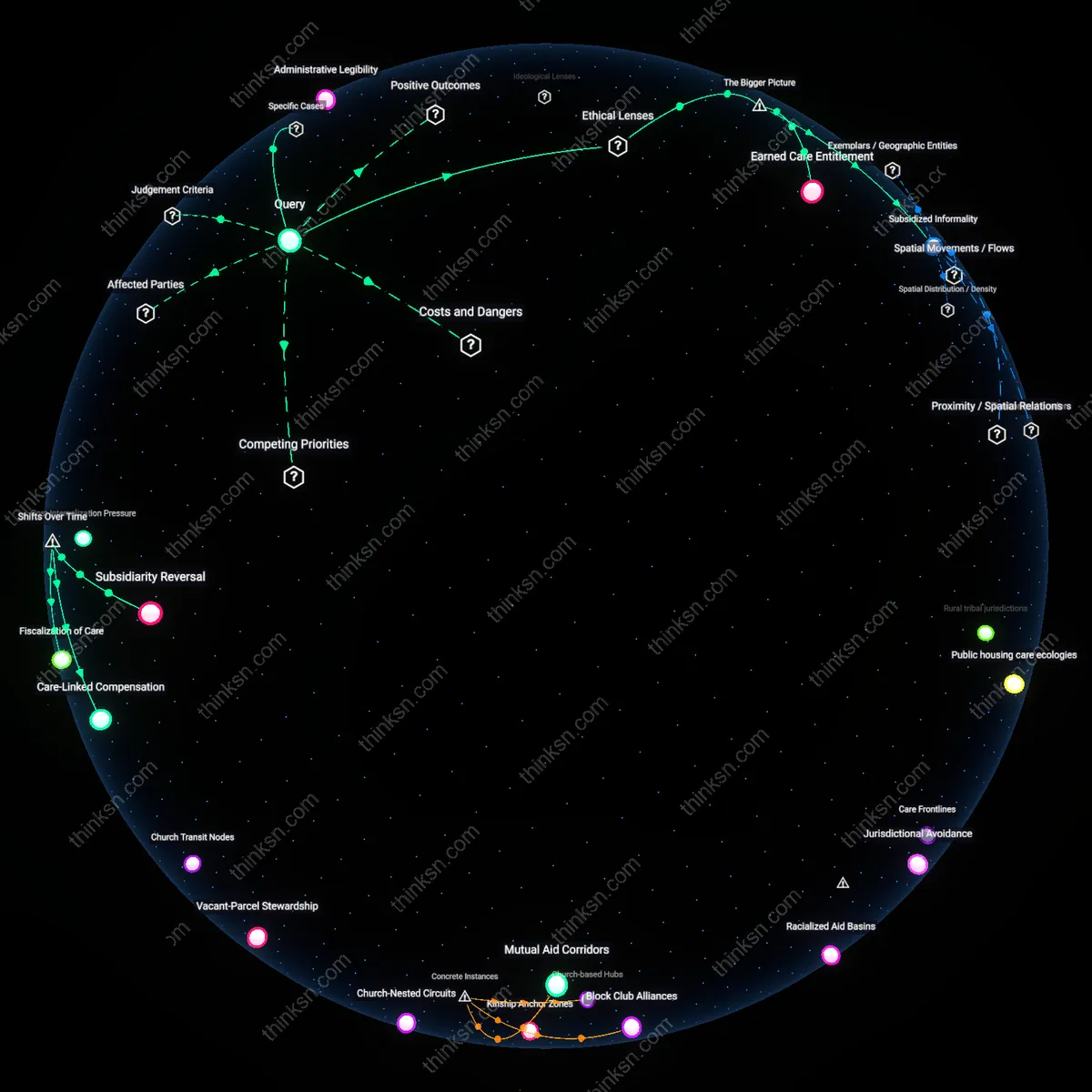
Church-based Hubs
Informal care networks in Youngstown are concentrated in historic Black church congregations such as St. Mark Missionary Baptist Church on Selby Avenue, where pastors coordinate food pantries, rental assistance, and mental health counseling through volunteer deacons and stewardship committees that link families across the city’s South Side and downtown corridors; this structure reveals how religious institutions function as institutional nodes that sustain care beyond formal social services, leveraging trust and moral authority to maintain continuity amid municipal disinvestment.
Block Club Alliances
In the Idora neighborhood of Youngstown, the Idora East Community Organization operates a block club network where residents on contiguous streets like Wick Avenue and Selma Road share emergency contact lists, perform wellness checks, and organize trash cleanups through neighborhood captain roles that extend informal care into a spatially coordinated system; this illustrates how hyperlocal territorial organization enables resilience by transforming geographic adjacency into a relational infrastructure that persists despite population decline.
Mutual Aid Corridors
Following the 2016 closure of the Youngstown Municipal Health Department’s East Side clinic, residents around the Lincoln Knolls housing complex initiated a decentralized mutual aid corridor, using Facebook groups and church basements to route insulin deliveries and ride shares between Mahoning Avenue and Elm Road households; this case exposes how care networks reconfigure along digital-physical hybrid pathways when institutional vacuums force ad hoc connectivity across discontinuous urban zones.
Kinship Anchor Zones
Informal care networks are most concentrated in older, working-class neighborhoods where multi-generational households persist, such as those near Youngstown’s historic steel mill districts. These areas exhibit high spatial density of familial caregiving because aging homeowners remain in place while adult children, often economically constrained, co-reside or settle nearby—forming clusters of intergenerational support that function as de facto care infrastructure. The non-obvious significance is that these zones are not random but anchored in residual industrial geography, where declining mobility and limited housing turnover consolidate care within kinship structures rather than disperse it into formal systems.
Church-Nested Circuits
Informal care networks radiate outward from established African American congregations in neighborhoods like Eastgate and Austintown, where local churches serve not just as spiritual centers but as logistical hubs for meal delivery, transportation, and elder check-ins. These circuits operate through volunteer deacons, neighborhood stewards, and parish-based mutual aid lists, creating lateral connections between households that span several blocks but remain bounded by congregational reach. The underappreciated insight is that these networks are not merely symbolic or episodic—they form persistent, addressable care topologies that city services often mistake for spontaneity rather than structure.
Pharmacy-Triangle Nodes
Care coordination unofficially clusters around corner pharmacies in commercially thin districts, such as those along South Meridian Avenue, where pharmacists develop personal knowledge of elderly patrons and act as sentinels for health deterioration or social isolation. These nodes become waypoints where neighbors relay updates, pick up medicines for others, or notice who has stopped coming in—triggering informal interventions. The overlooked mechanism is that these are not just points of service but observational infrastructure, turning routine commercial spaces into low-resolution surveillance systems that map vulnerability through attendance.
Care Frontlines
Informal care networks in Youngstown are concentrated not in low-income neighborhoods as expected, but along the deindustrialized corridors where former steelworker households maintain reciprocal obligations across emptied blocks. These networks operate through retired union members who coordinate medical transport, food sharing, and housing watch systems using landline trees and church bulletins, bypassing digital platforms; this spatial distribution contradicts the assumption that care follows current poverty density, revealing that residual industrial citizenship—not present need alone—structures where informal support endures.
Jurisdictional Avoidance
These networks concentrate in extramural zones—spaces between incorporated city boundaries and unincorporated county land—where municipal services have withdrawn, and residents respond by forming off-grid care collectives that deliberately obscure their locations from official registries. By situating themselves in unaddressable gaps of governance, these groups leverage jurisdictional invisibility to avoid surveillance while sharing prescription medications and childcare duties; this challenges the normative view that care networks seek institutional integration, exposing an active preference for sanctioned abandonment as a survival strategy.
Racialized Aid Basins
Informal care in Youngstown flows not across contiguous neighborhoods but through historically segregated circuits that follow mid-20th-century redlining contours, where Black mutual aid groups operate parallel to, but do not connect with, white ethnic parishes despite geographic proximity. These networks use neighborhood-specific kinship markers and church-based trust protocols that filter access, revealing that solidarity is not organic but gated by memory of past discrimination—undermining the progressive narrative that urban closeness naturally fosters integrated care.
Institutional Anchors
Informal care networks in Youngstown are concentrated near institutional anchors such as churches, community health clinics, and public housing complexes because these sites serve as trusted hubs where residents exchange caregiving resources under conditions of systemic disinvestment. Churches in neighborhoods like Idora and Mahoning West operate food pantries and transportation networks that bind together elderly, disabled, and low-income households across blocks with limited municipal services. The proximity to these institutions enables repeated, face-to-face coordination that sustains informal care—despite the absence of formal infrastructure—because clergy, volunteer coordinators, and long-term residents act as social glue under pressure from urban depopulation and austerity. What is underappreciated is that these nodes do not merely reflect community resilience but actively reproduce it by concentrating fragile caregiving labor where institutional presence creates minimal conditions for trust and continuity.
Spatial Mismatch
Informal care networks are fragmented across Youngstown’s neighborhoods due to spatial mismatch between where care is needed and where capable caregivers reside, a condition intensified by decades of job loss and suburban flight that have unevenly hollowed out household stability. On the city’s east side, aging homeowners without familial support live in isolation, while younger caregivers with kinship obligations are clustered in the more densely populated central corridors near downtown and educational institutions. This disjuncture disrupts network continuity because care relies on bodily presence and daily routines, making cross-neighborhood ties difficult without reliable transportation or coordinated community brokers. The overlooked systemic dynamic is that informal care does not scale across distance in shrinking cities—not because of cultural breakdown, but because deindustrialization created a geography where demand and capacity are structurally decoupled.
Service Void Feedback
Informal care networks thicken in Youngstown’s service voids—areas where public transportation, grocery stores, and health services have been withdrawn—because residents adapt to abandonment by turning kinship and neighborly obligation into functional substitutes for missing institutions. In the Fifth and Tenth Wards, for example, residents organize informal ride-shares to dialysis appointments and rotate meal deliveries for shut-ins, not as isolated acts of charity but as repeated, location-dependent responses to infrastructural collapse. These localized networks rarely connect across neighborhoods because survival demands are immediate and place-bound, trapping care labor in micro-geographies and preventing the formation of citywide mutual aid structures. The non-obvious consequence is that municipal neglect does not simply strain care systems but actively shapes their spatial limits, reinforcing a feedback loop where isolation breeds hyperlocal solutions that cannot aggregate into broader resilience.
Vacant-Parcel Stewardship
Informal care networks shifted from private homes to semi-public land parcels after 2005, when the Youngstown 2010 plan triggered mass demolition of vacant housing, relocating care practices to repurposed lots where former neighbors co-manage gardens, memorials, and storage spaces. This spatial redistribution transformed care from domestic duty to stewardship, embedding it in contested terrain between municipal abandonment and resident persistence, with elders often serving as lot 'caretakers' who maintain social ties through shared land use. The underappreciated shift is that care infrastructure became visible only when structures were removed, revealing land itself as a connective substrate across hollowed neighborhoods.
Church Transit Nodes
After the closure of the Southern Ohio Medical Mission outreach in 2012, storefront churches in Youngstown’s 44504 and 44505 ZIP codes reorganized as transit nodes, converting Sunday services into coordinated ride-sharing schedules that connect elderly congregants across formerly segregated north-south corridors. These nodes emerged precisely when public transit routes were cut by Mahoning County in 2013–2014, forcing congregations to substitute spiritual gathering with logistical coordination to maintain access to dialysis clinics, pharmacies, and food banks. The critical insight is that religious infrastructure did not merely host care—it became a real-time routing system, with pastors doubling as dispatchers in a city whose formal mobility systems had collapsed.