Does a Big Emergency Fund Cover Health Shocks with High Deductible Insurance?
Analysis reveals 11 key thematic connections.
Key Findings
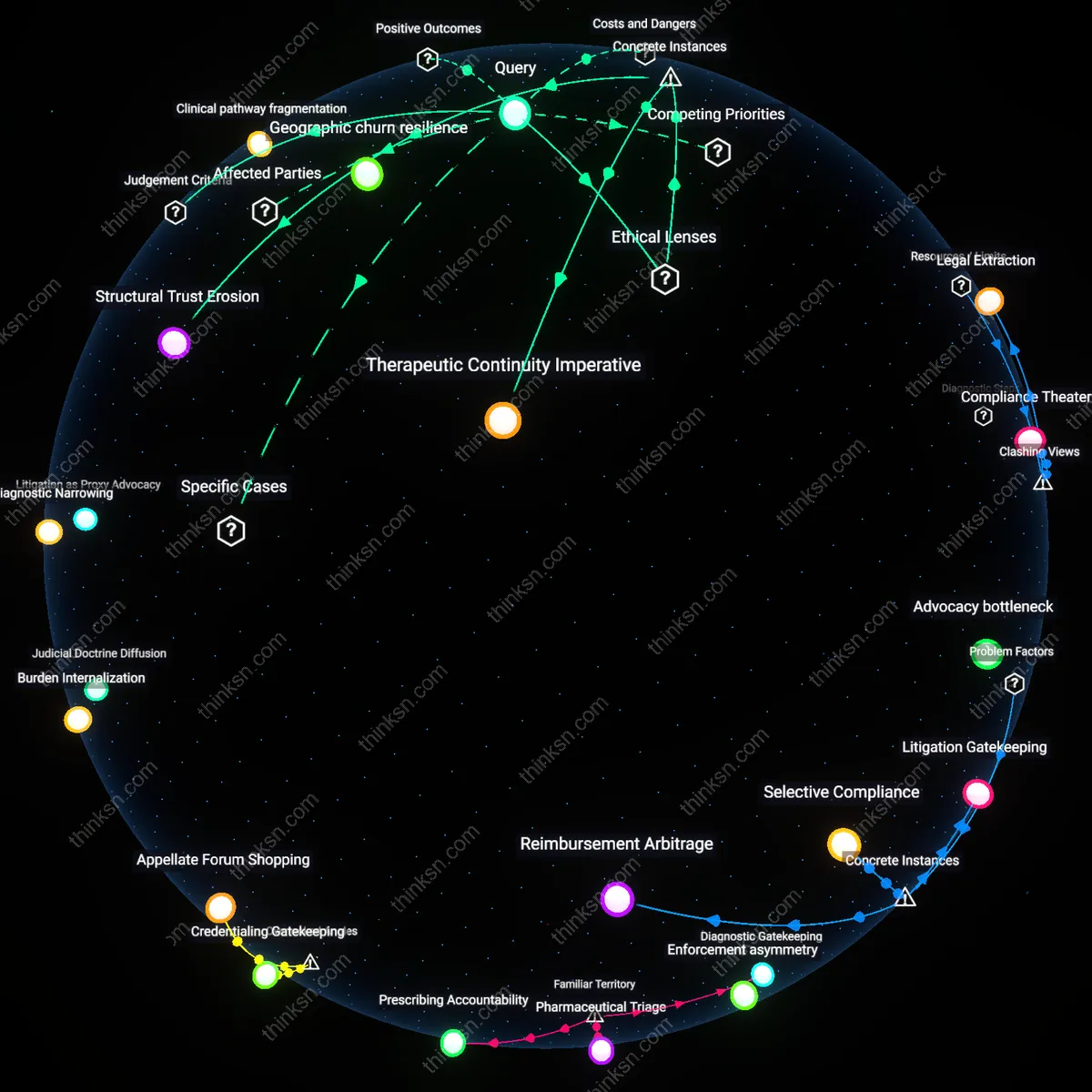
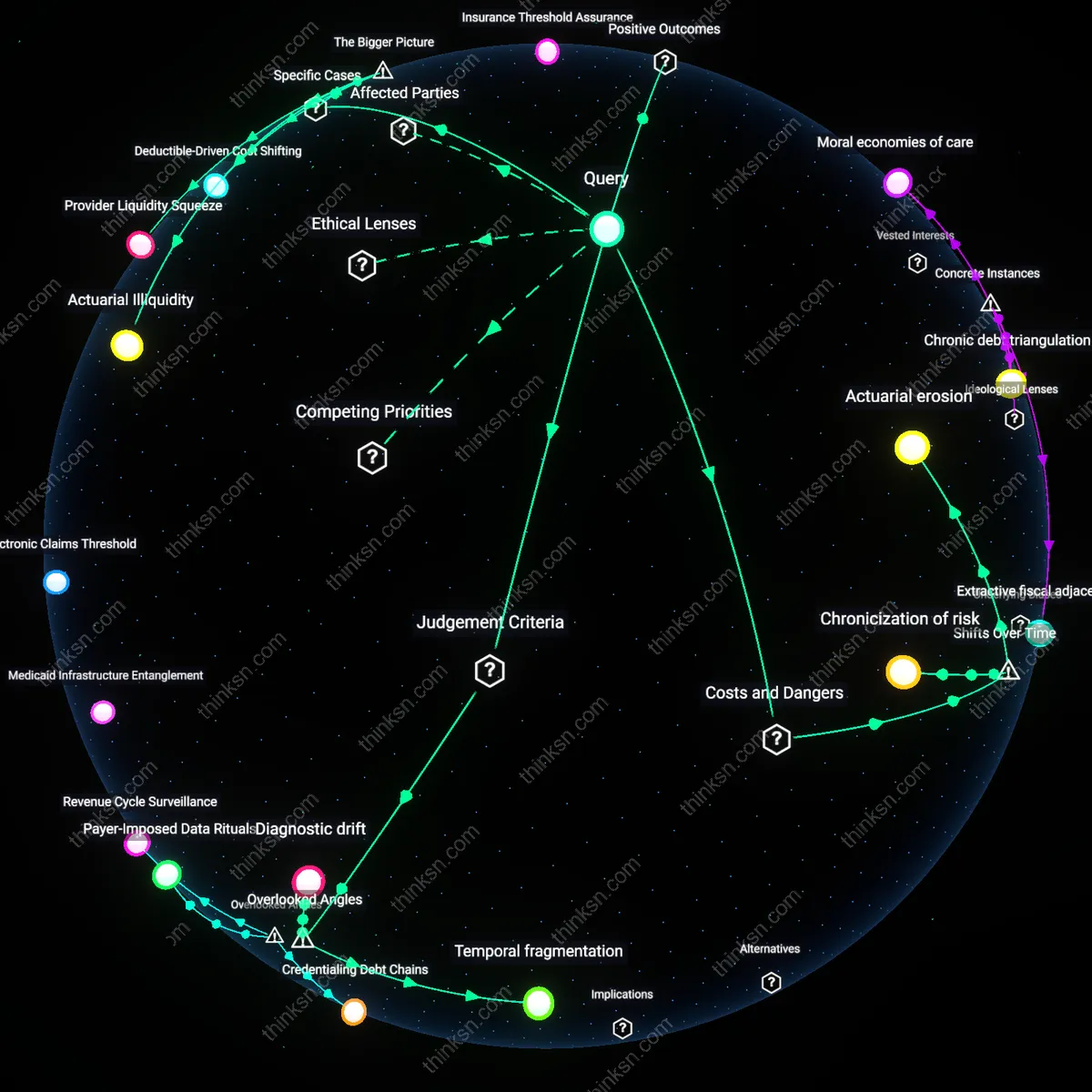
Temporal fragmentation
A larger emergency fund fails to reliably cover unexpected healthcare costs under high-deductible insurance because the timing of expenses disrupts cash flow continuity, even when total savings exceed annual deductibles. Families face medical bills in unpredictable bursts—such as a child’s asthma emergency in winter followed by an orthopedic injury in summer—forcing repeated cycles of depletion and cautious replenishment that prevent sustained financial resilience. This fragmentation, not the absolute size of savings, determines effective coverage—yet most financial planning overlooks the rhythm of medical need in favor of static thresholds, mistaking adequacy for availability.
Provider liquidity mismatch
A larger emergency fund cannot reliably cover unexpected healthcare costs when hospitals or clinics refuse to honor installment plans that align with family cash flow cycles, triggering outsized penalties that drain reserves disproportionately. Providers often treat insurance as the primary payer and impose rigid, front-loaded payment demands after denial or delay, leaving families with savings but no access to time-smoothed disbursement—particularly in rural clinics reliant on rapid revenue cycles. This institutional insensitivity to household liquidity schedules—overlooked in insurance-centered analyses—means that even fully funded reserves become practically inaccessible when timing misaligns with medical billing rigidity.
Diagnostic drift
A larger emergency fund weakens in effectiveness because escalating diagnostic intensity after an initial event—such as repeated imaging or specialist referrals following a single emergency room visit—generates layered costs that exceed predictable outlays, despite deductibles being known. These cascading micro-decisions by clinicians, incentivized by fragmented reimbursement and liability avoidance, produce expense paths that are temporally dispersed and cognitively invisible to families managing savings. Most cost projections assume bounded events, not compounding ambiguity, rendering emergency funds structurally mismatched to the slow bleed of diagnostic creep, a process buried in clinical workflows and rarely modeled in household risk planning.
Financial Buffer Stability
A larger emergency fund directly enables families with high deductible insurance to pay for urgent medical procedures without resorting to credit, preserving their creditworthiness and reducing financial stress during health crises. This stability emerges because out-of-pocket costs for emergencies like ER visits or surgeries are often predictable in range—if not in timing—and a sufficiently large fund aligns with these known cost bands, especially when held in liquid accounts tied to routine banking relationships. Most people intuitively connect emergency savings with avoiding debt, yet the deeper utility lies in maintaining decision autonomy during care episodes, insulating household planning from insurer reimbursement delays.
Insurance Threshold Assurance
A robust emergency fund reliably covers costs up to the deductible, allowing families to activate full insurance benefits faster by meeting plan thresholds without hesitation. This mechanism functions through the design of high-deductible health plans themselves, where once the deductible is met, coinsurance and network coverage kick in, reducing downstream liability—so paying the initial amount confidently enables better long-term cost control. Though people commonly see deductibles as financial hurdles, the fund transforms them into predictable milestones, making the insurance structure work as intended and turning a barrier into a bridge.
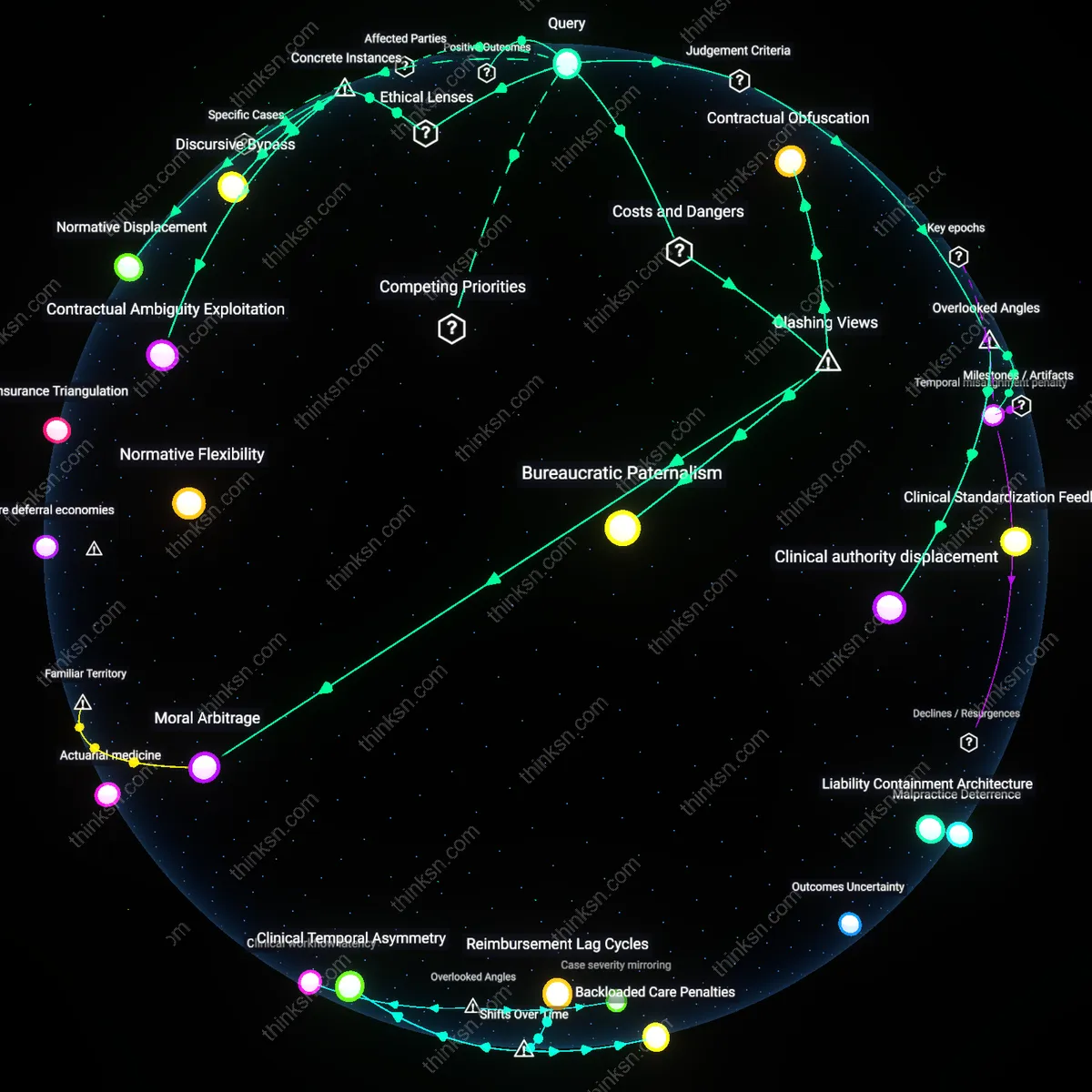
Actuarial erosion
A larger emergency fund fails to reliably cover unexpected healthcare costs under high-deductible insurance because the 2010 shift toward consumer-driven health plans recalibrated risk exposure away from insurers and onto families, who now face unpredictable pricing and treatment timing that undermine savings stability. Health systems, incentivized by fee-for-service models widespread after the Affordable Care Act’s marketplace expansions, increasingly schedule or delay procedures in ways that compress costs into volatile, front-loaded periods—bypassing even robust household liquidity. This creates a temporal misalignment where saved funds are depleted by design rather than accident, exposing a hidden actuarial logic transferred from institutions to individuals.
Chronicization of risk
The effectiveness of emergency savings diminishes over time for families with high-deductible insurance due to a post-2000 transition in employer-sponsored plans that redefined episodic medical events as recurring financial obligations, transforming what were once acute cost shocks into sustained out-of-pocket drains. As specialty drug regimens, preventive screenings, and chronic disease management became standard under managed care protocols, expenses became predictable in aggregate but unpredictable in sequence—eroding lump-sum funds through repeated, staggered withdrawals. This chronicization converts emergency reserves into de facto payment plans, revealing the structural sabotage of short-term financial buffers by long-term medical timelines.
Temporal extraction
Larger emergency funds are systematically weakened by the timing of healthcare expenses because the consolidation of hospital systems after 2015 enabled coordinated billing cycles and procedural bundling that exploit known depletion patterns in household savings. Providers, operating under private equity-backed efficiency mandates, increasingly cluster non-emergent but urgent services—like imaging, diagnostics, and follow-ups—within single deductible windows to maximize patient liability capture. This timing strategy, refined through data analytics on consumer payment behavior, transforms the emergency fund not into a shield but into a target, extracting value through temporal precision rather than medical necessity.
Actuarial Illiquidity
A larger emergency fund fails to cover high-deductible healthcare costs for working-class families in metro Atlanta because sudden hospitalization forces liquidity conversion during wage-interruption periods, exposing a mismatch between saved assets and cash-flow timing; this mechanism intensifies under employer-based insurance systems where deductibles reset annually regardless of income volatility, revealing that financial buffers are constrained not by total saved value but by the synchronization of asset availability with episodic income shocks.
Provider Liquidity Squeeze
In rural Maine, even substantial emergency funds falter in covering unexpected care because local clinics demand upfront payment before billing high-deductible plans, forcing families to exhaust savings months before insurance coverage activates; this reflects a systemic misalignment between patient savings capacity and medical providers’ need for immediate revenue stabilization under value-based care models, where delayed reimbursement cycles push financial risk onto consumers at the point of service.
Deductible-Driven Cost Shifting
For Latino gig workers in Los Angeles County, large emergency funds are systematically depleted by routine care misclassified as emergencies due to narrow provider networks under high-deductible ACA plans, triggering full-cost liability before deductible thresholds are met; this effect emerges from regulatory gaps allowing insurers to enforce strict network rules while classifying out-of-network care as non-qualifying, thereby converting savings into premium cost-shifting mechanisms that benefit insurers’ risk-pool management at the household level.