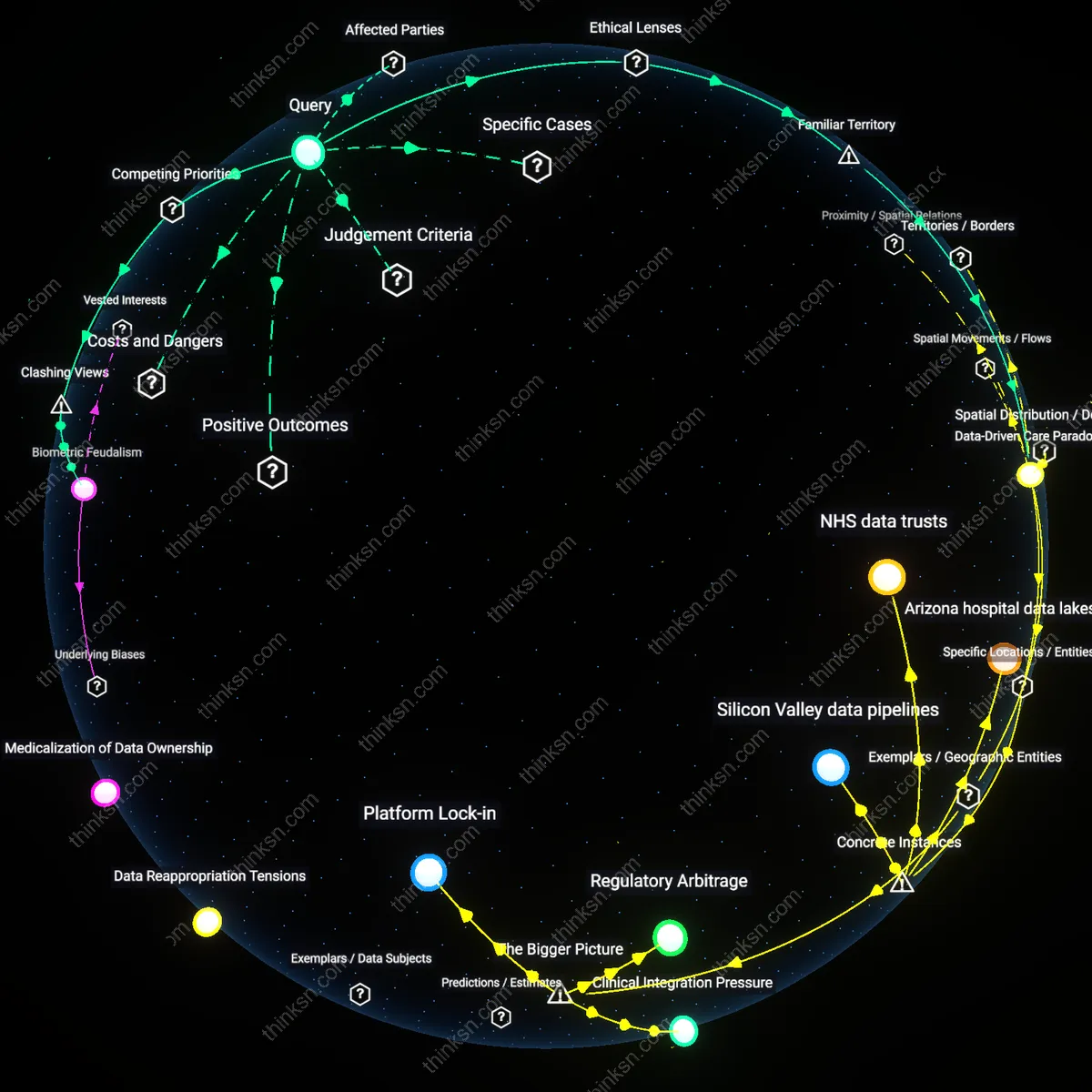
Are Heart-Rate Trackers Justified by Data or Demand?
Analysis reveals 11 key thematic connections.
Key Findings
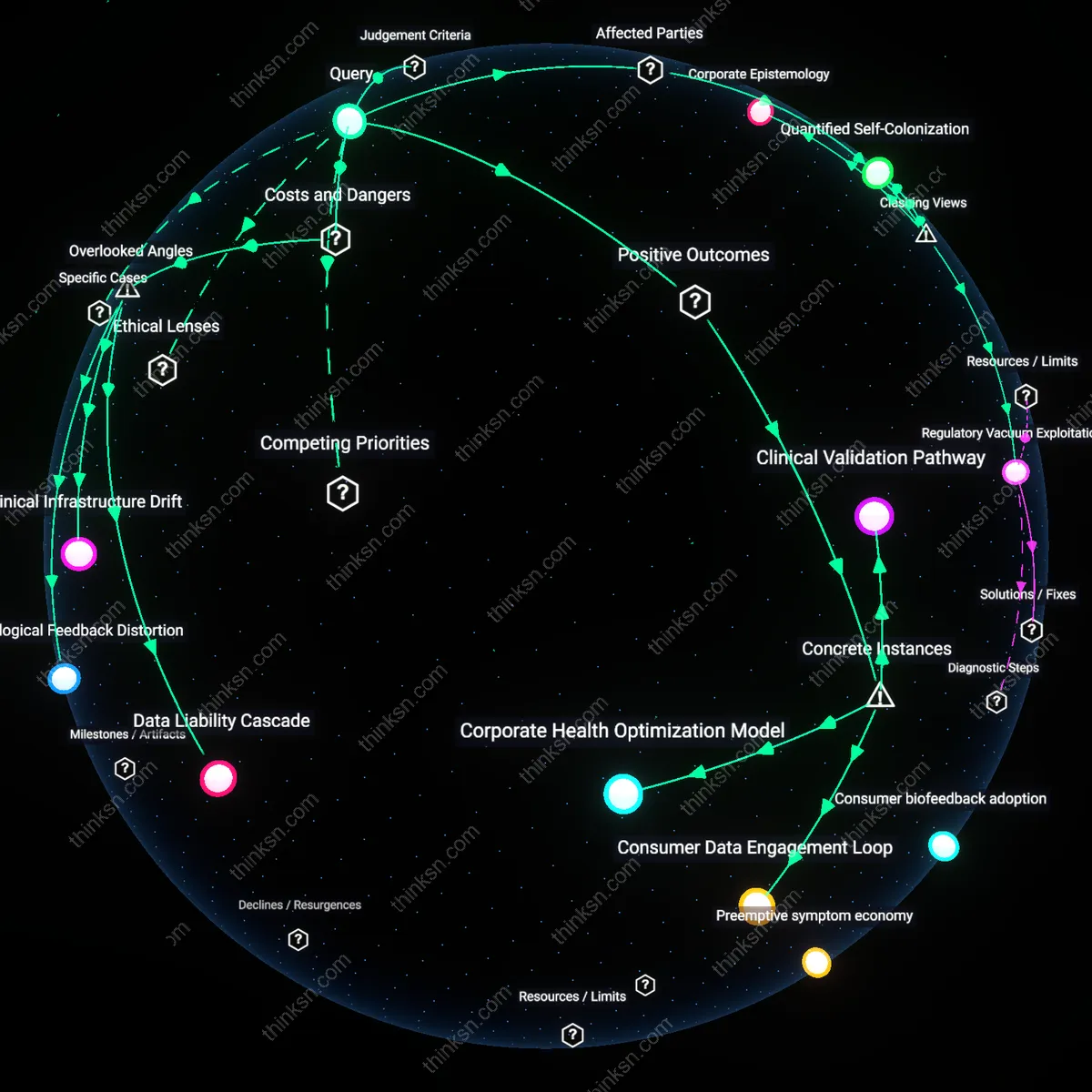
Corporate Epistemology
The promotion of wearable heart-rate variability trackers is driven primarily by corporate imperatives to generate proprietary health data ecosystems, not by robust predictive evidence or spontaneous consumer demand. Device manufacturers like WHOOP and Oura partner with employers, professional sports teams, and insurance-adjacent wellness programs to embed their metrics into performance and risk-assessment protocols, effectively manufacturing validity through institutional adoption rather than clinical validation. This reframes HRV as a performative health signal—its utility emerging from repeated use in high-stakes contexts, not from evidence of causality—revealing how commercial entities now shape what counts as medical knowledge. The non-obvious mechanism is not consumer curiosity or scientific rigor, but the strategic alignment of wearable firms with institutions that can enforce usage and normalize interpretation.
Quantified Self-Colonization
Wearable HRV tracker promotion thrives on a hidden transfer of biometric labor from clinical settings to individuals, where self-tracking becomes an unpaid responsibility to optimize one’s own health viability. Employers and healthcare systems increasingly incentivize or expect continuous HRV monitoring through wellness programs, subtly shifting accountability for health outcomes onto employees and patients while reducing institutional obligations to provide care. This dynamic disguises austerity-driven disinvestment in public health as personal empowerment, making it appear that individuals are gaining insight when they are actually absorbing systemic risk. The clash lies in reframing consumer interest not as autonomous curiosity but as coerced participation in a data economy that benefits actuaries, HR departments, and platform owners.
Regulatory Vacuum Exploitation
The expansion of HRV tracker marketing is enabled by deliberate regulatory gaps that allow companies to make implicit health claims without meeting FDA-grade evidentiary standards for medical devices. By positioning devices as 'wellness' or 'fitness' tools, firms like Fitbit and Garmin bypass rigorous validation while still leveraging associations with clinical terminology, such that cardiologists, athletes, and corporate wellness coordinators adopt HRV trends as decision-making inputs absent peer-reviewed consensus. This creates a de facto standard of health assessment developed in Silicon Valley, not cardiology wards, where market presence substitutes for scientific proof. The underappreciated force here is not consumer desire or scientific progress, but the strategic exploitation of legal ambiguity to pre-empt regulation through widespread normalization.
Commercial Viability Imperative
The promotion of wearable heart-rate variability trackers is driven primarily by the need for device manufacturers to justify recurring revenue models through continuous data engagement, not by conclusive clinical validation. Companies like Fitbit and Apple invest heavily in HRV marketing because sustained user engagement unlocks subscription upsells and ecosystem lock-in, turning biometric tracking into a profit engine rather than a diagnostic tool. The mechanism—monetizing data streams via behaviorally sticky dashboards—reveals that economic efficiency, not medical accuracy, is the operative yardstick. Most consumers assume HRV feedback implies clinical utility, but the non-obvious reality is that these features often precede peer-reviewed endorsement, exploiting regulatory gaps in wellness tech.
Quantified Self Aspiration
Promotion of HRV wearables succeeds because it taps into the culturally ingrained belief that numerical self-tracking enables personal mastery, making consumer interest the dominant driver regardless of evidentiary strength. The familiar trope of the 'data-driven self'—visible in morning routine vlogs, corporate wellness challenges, and biohacking forums—frames HRV as a proxy for resilience, discipline, and optimization. Here, autonomy and self-determination function as the implicit moral principles, legitimizing adoption even when predictive validity is uncertain. The underappreciated insight is that the numbers need not be medically meaningful to be psychologically salient; the mere act of measurement satisfies a widespread desire for perceptible control over invisible bodily processes.
Clinical Validation Pathway
The Mayo Clinic's collaboration with Fitbit to validate heart-rate variability (HRV) data for atrial fibrillation detection demonstrates that medical institutions are integrating wearable HRV metrics only when aligned with clinical evidence, as seen in the 2021 mSToPS study, which used real-world wearable data to inform arrhythmia screening protocols, revealing that regulatory and institutional adoption hinges on verifiable predictive utility rather than consumer enthusiasm alone, a non-obvious restraint in a market flooded with consumer-driven health tech.
Consumer Data Engagement Loop
Oura Ring’s uptake during the 2020 Olympic athlete monitoring trials, where non-elite users emulated biohacking regimens after publicized data dashboards showed optimized recovery windows, illustrates how consumer fascination with quantified self-metrics drives market expansion independent of medical validation, operating through a feedback loop where visible data personalization enhances perceived self-efficacy, underscoring that commercial momentum often precedes and shapes evidence standards rather than awaiting them.
Corporate Health Optimization Model
Johnson & Johnson’s implementation of WHOOP bands in its employee wellness program at its New Brunswick facilities in 2022, which tied aggregate HRV trends to reductions in self-reported stress and absenteeism, reveals how enterprise adopters leverage wearable HRV data not for individual diagnosis but as a population-level productivity tool, where measurable biometrics serve as proxies for workforce resilience, exposing a growing institutional preference for actionable organizational insights over individual clinical precision.
Data Liability Cascade
Wearable HRV trackers are proliferating primarily due to unpriced downstream data externalities, not clinical validation or consumer health literacy. Health-tech firms and insurers benefit from aggregated, continuous biometric streams that feed risk modeling, yet individuals bear the costs when data is repurposed for employment screening or premium adjustments—mechanisms invisible at point of purchase. This creates a liability cascade where the harm emerges not from device inaccuracy but from the silent integration of personal physiology into actuarial systems that lack transparency or recourse. The overlooked dimension is that HRV data, framed as personal insight, functions more like a speculative commodity in administrative risk markets, shifting systemic risk onto users who are unaware they are feeding actuarial engines.
Physiological Feedback Distortion
The promotion of HRV wearables amplifies a hidden feedback distortion where users’ stress regulation is undermined by the very act of monitoring autonomic states in non-clinical settings. Because HRV is sensitive to acute psychological factors—including the anxiety of observing one’s own fluctuating metrics—tracking can induce dysregulation rather than insight, particularly in high-performing or clinically vulnerable populations. This iatrogenic loop is structurally embedded in consumer-facing devices that provide no contextual interpretation or clinical guardrails, turning intermittent surveillance into a maladaptive behavioral schema. The underappreciated reality is that continuous autonomic feedback, detached from therapeutic frameworks, can degrade self-regulation—a harm invisible to standard efficacy trials focused on data correlation rather than psychophysiological consequence.
Clinical Infrastructure Drift
The normalization of HRV tracking diverts public and institutional attention toward individualized, commercially owned monitoring systems while eroding investment in equitable, population-level cardiovascular diagnostics and care. As clinics and employers adopt consumer-grade wearables as proxies for health risk assessment, gaps widen in access to validated tools like ambulatory ECG or cardiologist interpretation, particularly in underresourced communities. This drift repackages public health responsibility as personal data hygiene, enabling policymakers to cite 'democratized health tech' while defunding structural care pathways. The overlooked shift is the quiet substitution of clinical infrastructure with proprietary data pipelines that benefit device makers more than patients, particularly where regulatory oversight conflates data availability with medical utility.