Carb Restriction Conflict for Active Type 1 Diabetics?
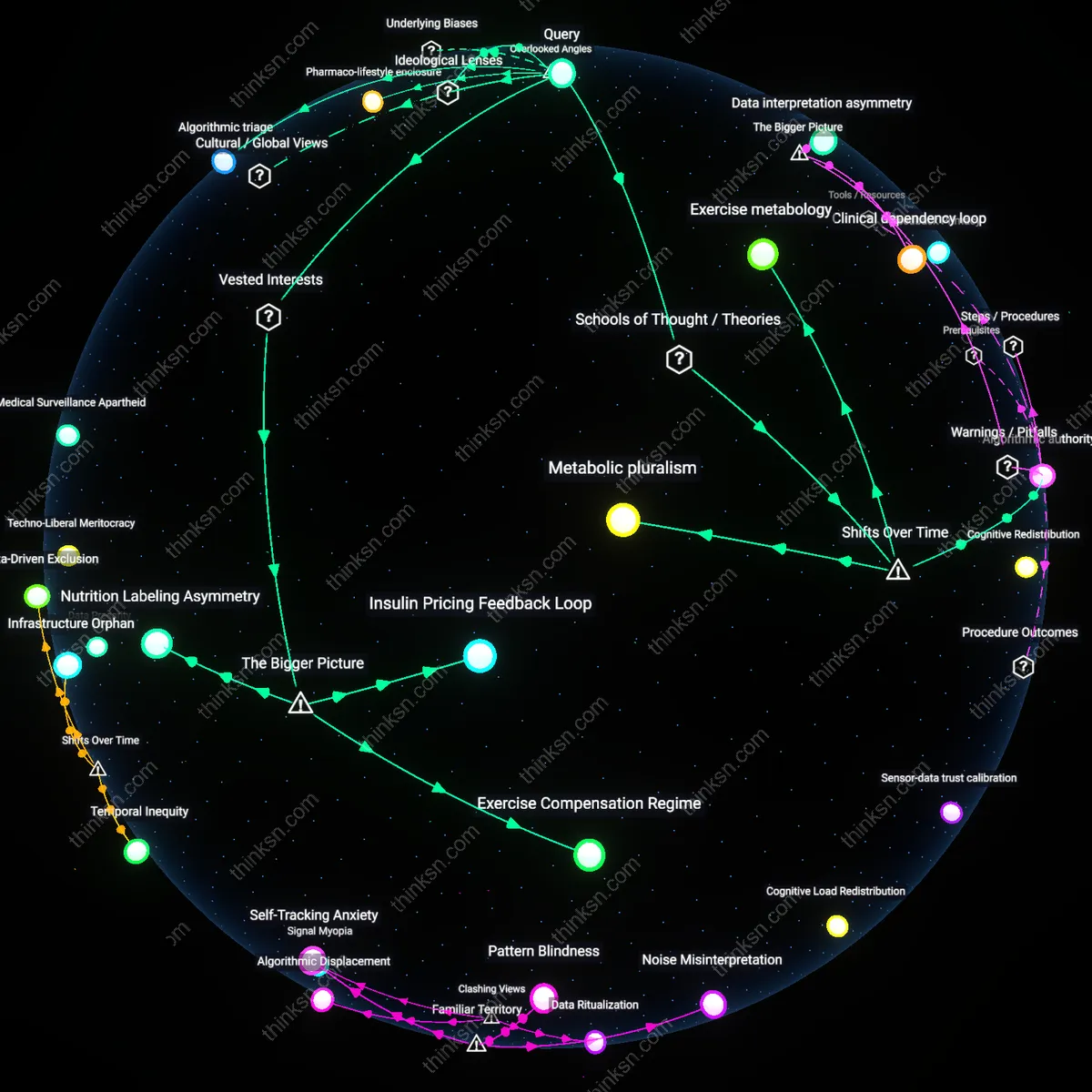
Analysis reveals 9 key thematic connections.
Key Findings
Algorithmic authority
Adopt continuous glucose monitoring–informed insulin protocols to resolve conflicting carbohydrate advice by deferring to real-time metabolic feedback rather than prescriptive dietary norms. This shift, crystallized in the 2010s with the widespread clinical adoption of hybrid closed-loop systems, transferred decisional authority from physician-guided carbohydrate counting to algorithmically processed glucose dynamics, embedding medical judgment within wearable devices. The mechanism—automated insulin titration based on interstitial glucose levels—reconfigures the clinician’s role from directive planner to supervisory interpreter, revealing how technological mediation has quietly displaced nutritional dogma in diabetes management. What is underappreciated is that this transition did not emerge from clinical consensus but from patient-led innovation and iterative device optimization, destabilizing traditional hierarchies of medical expertise.
Metabolic pluralism
Respect individualized glycemic responses by prioritizing personalized dietary experimentation over standardized macronutrient thresholds, a practice that gained legitimacy through the post-2015 proliferation of ambulatory glucose profile (AGP) analysis in diabetes centers. This shift from population-based guidelines to n-of-1 phenotyping reflects a broader epistemic turn in precision medicine, where interindividual variation in insulin sensitivity and fuel utilization becomes the central clinical variable rather than an outlier to be averaged away. Operating through structured trial periods with controlled carbohydrate loads, clinicians now map idiosyncratic metabolic behaviors that defy conventional low-, moderate-, or high-carb classifications. The underappreciated insight is that this trajectory undermines the very premise of universal carbohydrate recommendations, exposing them as artifacts of mid-20th-century nutritional epidemiology ill-suited to the variability of active type 1 diabetes physiology.
Exercise metabology
Integrate fueling strategies based on acute exercise modality—such as endurance, resistance, or interval training—because the post-2000s expansion of sport science research into type 1 diabetes revealed that muscle contraction-induced glucose uptake fundamentally alters carbohydrate requirements independently of insulin. This recalibration replaces static dietary advice with dynamic metabolic forecasting, where pre-exercise glycogen status, post-exercise insulin sensitivity windows, and catecholamine surges dictate carbohydrate needs more than baseline disease protocols. The mechanism is embedded in exercise physiology laboratories and specialized diabetes-sports clinics that treat physical activity not as a modifier of metabolic risk but as a primary regulator of glucose homeostasis. The overlooked consequence is that this development severs carbohydrate guidance from traditional nutritional frameworks, producing a new clinical domain where athletic training principles override inherited dietary orthodoxy.
Algorithmic triage
Adopt clinic-based hierarchical review by specialized diabetology ethics boards to resolve conflicting carbohydrate advice by institutionalizing algorithmic triage that weighs adherence risk against metabolic variability. These boards—composed of endocrinologists, behavioral specialists, and health informaticians—deploy protocolized decision trees derived from real-world glycemic outcome datasets, adjusting recommendations based on a patient’s historical compliance patterns and activity-linked insulin sensitivity shifts. The non-obvious mechanism is that medical conflict resolution increasingly operates not through expert consensus but through proceduralized computational governance embedded in clinical workflows, where ethical deferral to algorithms masks unresolved clinical ambiguity while maintaining operational continuity.
Nutritional sovereignty
Empower patients to generate personal dietary epistemologies through open-access continuous glucose monitoring data sharing collectives, activating nutritional sovereignty as the means to transcend conflicting top-down carbohydrate guidelines. Physically active patients with type 1 diabetes leverage decentralized platforms like DIYAPS and OpenAPS communities to co-produce context-specific carbohydrate-response models that challenge institutional norms by validating lived metabolic experience over clinical averages. What remains overlooked is that dietary conflict is not merely scientific but political—resolving it requires redistributing knowledge authority from medical institutions to networked patient-citizens who treat carbohydrate metabolism as a site of bodily self-determination.
Pharmaco-lifestyle enclosure
Expose how insulin pricing structures in the United States coerce clinicians into low-carbohydrate recommendations regardless of patient activity levels, making metabolic guidance a proxy for cost-containment in a privatized care system where high-carbohydrate regimens necessitate more frequent insulin titration and monitoring supplies. The unresolved dependency lies in the alignment of dietary advice with pharmaceutical revenue models, where recommendations converge on low-carb not due to efficacy alone but because they reduce insulin volume demand and stabilize profit margins for vertically integrated biotech-payer conglomerates. This reveals that medical conflict is ideologically suppressed through a pharmaco-lifestyle enclosure, wherein dietary freedom is constrained by the financial architecture of drug markets.
Insulin Pricing Feedback Loop
Align prescription guidelines with insulin affordability by tying clinical carbohydrate recommendations to pharmaceutical pricing pressures. U.S. insurers and endocrinologists increasingly tolerate higher-carb diets because they reduce demand for ultra-rapid insulin analogs, which are both costly and heavily marketed by firms like Eli Lilly and Novo Nordisk; when patients consume more carbohydrates, slower-acting insulins suffice, reinforcing dependence on older, cheaper formulations that remain profitable under fixed reimbursement models. This alignment between medical advice and cost containment emerges not from physiological consensus but from a feedback loop in which pharmaceutical pricing structures indirectly shape dietary guidelines through formulary decisions and provider incentives, revealing how drug economics—not metabolic science—stabilizes treatment norms in high-insulin-cost environments.
Exercise Compensation Regime
Adopt sport-specific carbohydrate protocols calibrated to training load cycles rather than fixed metabolic rules, because elite athletic institutions like the NCAA and professional leagues systematically suppress low-carb diabetes management to preserve competitive eligibility under current anti-doping and medical oversight frameworks. Since low-carbohydrate regimes can lower exogenous insulin requirements and mask insulin misuse in non-diabetic athletes, governing bodies tacitly endorse higher-carb intake to maintain metabolic ‘normalization’ that aligns with urine and blood screening thresholds. This creates a hidden regulatory incentive where medical advice diverges not over health outcomes but over institutional risk management, exposing how anti-cheating mechanisms in sports physiology inadvertently standardize diabetes care toward higher carbohydrate dependence.
Nutrition Labeling Asymmetry
Prioritize whole-food carbohydrate sources in guidelines to counteract the influence of medically justified low-carb advocacy being undermined by the deregulated supplement industry’s exploitation of ‘diabetes-friendly’ labeling loopholes. Companies like KetoSports and Quest Nutrition market high-fat, near-zero-carb products as compatible with type 1 diabetes, but these items circumvent FDA nutrition claims oversight by classifying as dietary supplements, not medical foods—enabling them to promote metabolic stability claims without accountability for glycemic variability in active users. As physicians dispute carb thresholds, the unregulated flood of these products creates de facto treatment pathways shaped by commercial labeling arbitrage, revealing how fragmented food regulation disables clinical consensus by allowing private actors to operationalize fringe interpretations of metabolic science.