Delayed Biologics: Ethics of Step Therapy and Treatment Equity?
Analysis reveals 8 key thematic connections.
Key Findings
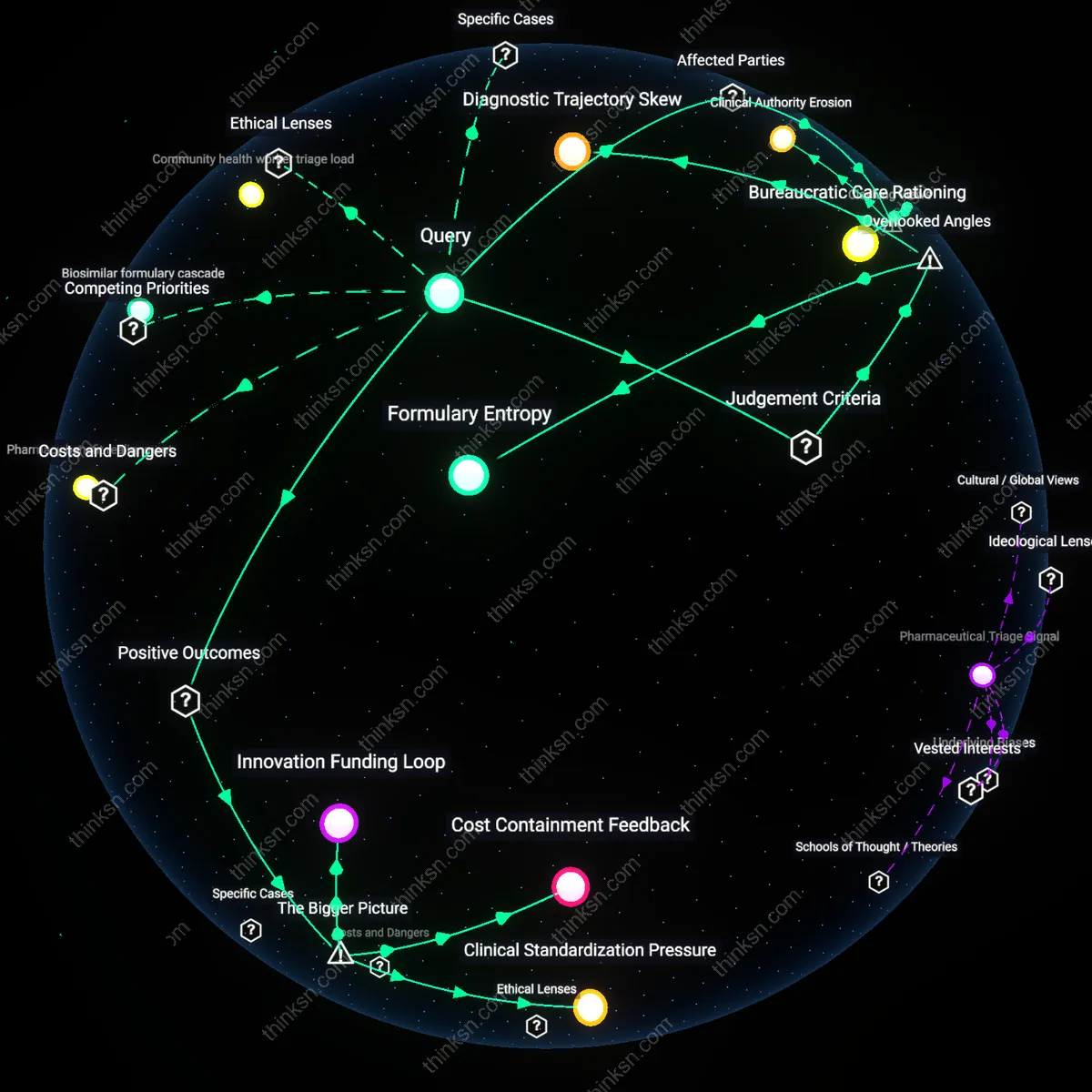
Bureaucratic Care Rationing
Step therapy mandates prioritize institutional cost containment over clinical immediacy, directly implicating insurers as active agents of treatment delay rather than passive intermediaries. Insurers deploy formulary protocols that force sequential drug trials, disproportionately impacting patients with rapidly progressing autoimmune conditions like rheumatoid arthritis, where months of delays erode joint integrity. This reveals that the real-time infliction of biological harm is not a side effect of policy but a designed feature of reimbursement algorithms calibrated to fiscal outcomes, challenging the notion that insurance oversight is medically neutral.
Therapeutic Time Debt
Patients from low-income urban communities bear accumulated harm when step therapy extends treatment timelines, effectively taxing those least equipped to manage prolonged illness. For example, Medicaid recipients in Detroit or Baltimore face compounded inequity as prior authorization processes demand clinical documentation they struggle to obtain due to fragmented care access. This dynamic reframes delay not as a temporary inconvenience but as a structural liability transferred from insurers to vulnerable populations, exposing how procedural burden functions as an invisible transfer mechanism in health financing.
Clinical Authority Erosion
Specialists in academic medical centers such as those in the Mayo Clinic system experience systematic sidelining when step therapy overrides treatment decisions based on patient-specific biomarkers and disease trajectory. The protocol reduces physician discretion to comply with predetermined pathways created by non-clinical pharmacy benefit managers, turning evidence-based judgment into appeal-driven labor. This inversion—where clinicians become administrative petitioners—reveals that step therapy doesn’t merely constrain access but reconfigures medical expertise as subordinate to managed care bureaucracy.
Formulary Entropy
Insurance-mandated step therapy accelerates formulary entropy by systematically degrading the coherence and responsiveness of drug benefit design over time, as payer policies ossify around legacy cost assumptions while biologic pipelines evolve. This creates a feedback loop where delayed adoption entrenches older, less effective drugs not due to clinical preference but administrative inertia, distorting physician prescribing norms and weakening the evidentiary base for newer agents. Typically unseen is how step therapy doesn’t just block access temporarily — it corrodes the adaptive capacity of insurance formularies, making them progressively less capable of integrating innovation, which undermines long-term treatment equity in ways invisible to short-cycle cost analyses.
Diagnostic Trajectory Skew
Step therapy distorts diagnostic trajectory skew by forcing clinicians to delay or avoid definitive diagnoses that would justify bypassing step requirements, especially in conditions like psoriatic arthritis where early biomarker use is discouraged by cost-contingent treatment rules. This results in diagnostic deferral — a hidden adaptation where physicians withhold confirmatory testing to prevent patient exposure to futile initial therapies, thereby altering the very shape of disease recognition. Rarely acknowledged is that step protocols don’t merely follow diagnosis; they reshape diagnostic behavior itself, creating iatrogenic uncertainty that disproportionately affects marginalized patients whose symptoms are already more likely to be discounted.
Cost Containment Feedback
Mandating step therapy reduces short-term pharmaceutical spending for insurers, which in turn stabilizes premium pricing for large employer-sponsored health plans in competitive markets like the U.S. commercial insurance sector. Insurers, under pressure from employers to curb rising drug costs, deploy step therapy as a gatekeeping mechanism that defers expensive biologic prescriptions until older, cheaper treatments fail—thereby maintaining financial sustainability within risk-pooled systems. This creates a feedback loop where cost discipline in one domain (drug utilization) enables broader system viability (insurance affordability), even as it introduces latency in therapeutic access—a trade-off rarely transparent to patients. The non-obvious implication is that the durability of insurance products themselves can depend on delaying innovation uptake.
Clinical Standardization Pressure
Step therapy protocols reinforce a systemic push toward uniform treatment pathways by aligning prescribing behavior with evidence-based guidelines validated in large-scale population data, such as those from the FDA’s Sentinel Initiative or real-world evidence networks. Payers, leveraging their position as data aggregators across millions of lives, can identify patterns where newer biologics are overprescribed relative to marginal clinical gains—then use step therapy to correct outlier practices among physicians influenced by pharmaceutical marketing. This standardization reduces unwarranted variation in care, promoting a more predictable and equitable baseline of treatment across geographies and provider types. The underappreciated dynamic is that payer mandates can function as de facto quality control mechanisms in decentralized care systems.
Innovation Funding Loop
Delaying access to newer biologics through step therapy indirectly sustains long-term innovation by preserving the financial viability of payer systems that ultimately fund future drug development via reimbursement commitments. Because biopharmaceutical firms rely on predictable revenue streams from insurers to justify R&D investments, especially in rare or complex conditions, the economic stability provided by cost-containment practices ensures continued participation in high-risk therapeutic markets. This creates a feedback loop where today’s access restrictions support tomorrow’s drug pipelines—a paradoxical but essential dependency between access friction and future medical advancement. The overlooked reality is that payer frugality can be a structural precondition for sustained biologic innovation.