Why Does Medication Cost Soar After Insurance Change?
Analysis reveals 9 key thematic connections.
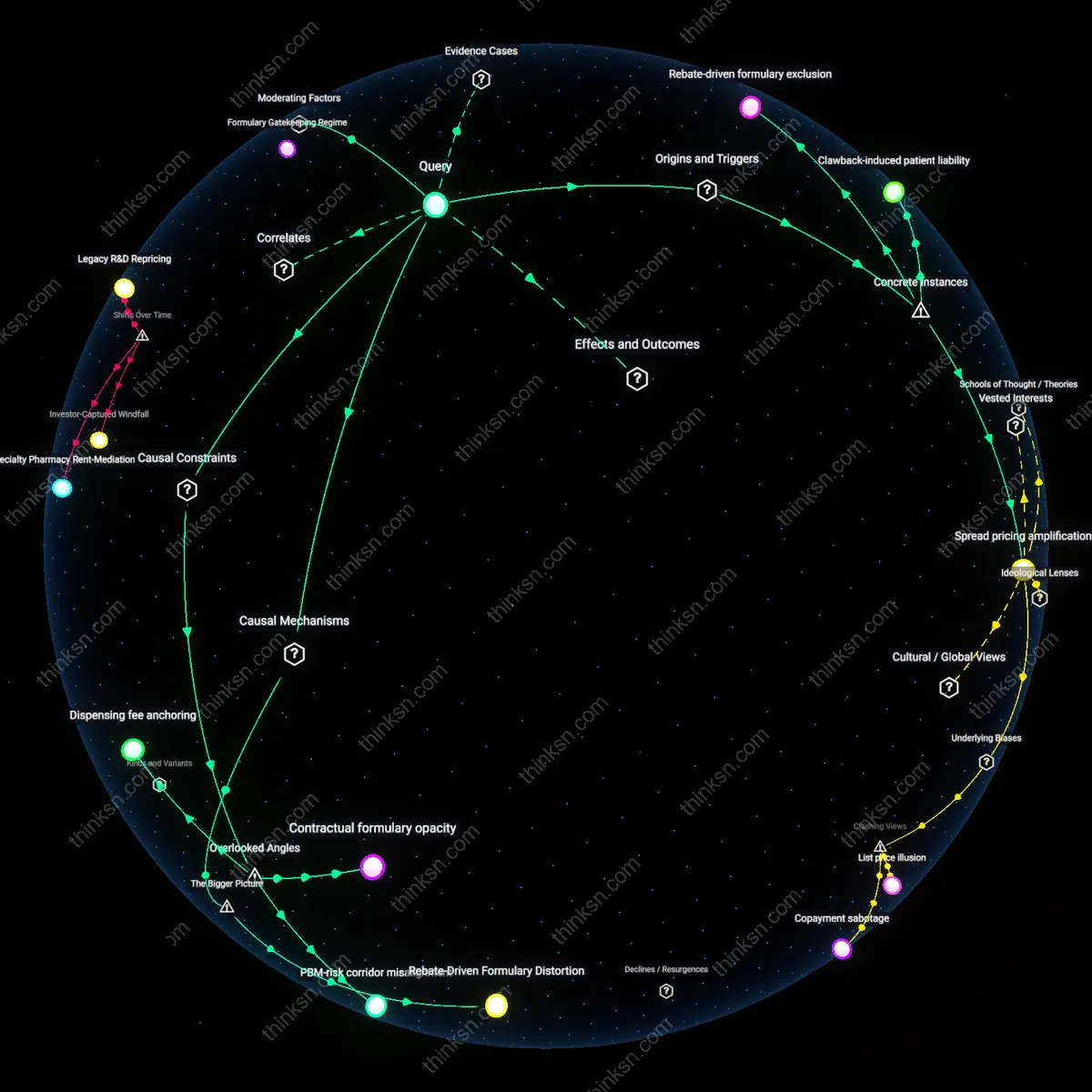
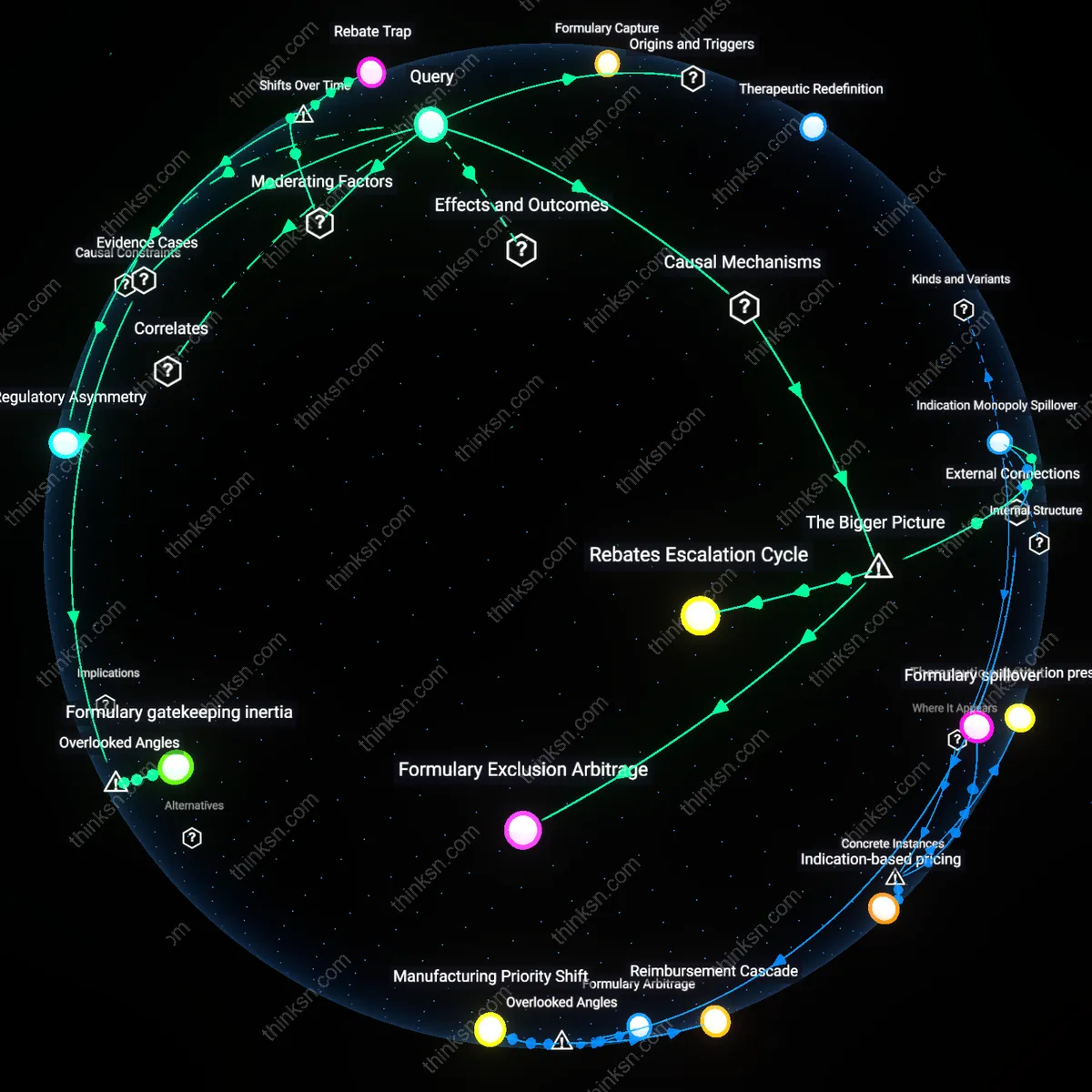
Key Findings
Regulatory Arbitrage
Changes in insurance coverage trigger price spikes not due to demand shifts but because manufacturers exploit gaps between public formulary design and private payer flexibility, allowing them to reposition drugs as 'specialty' products shielded from price competition. This mechanism hinges on the intentional misalignment between Medicare Part D’s coverage rules and commercial insurers’ benefit designs, which firms actively lobby to maintain—enabling list price increases without immediate access penalties. The non-obvious insight is that pricing surges are not market responses but calculated regulatory exploits, revealing price-setting as a legal-administrative maneuver rather than a commercial one.
Formulary Capture
Sharp medication price increases after insurance changes are driven by pharmaceutical firms securing preferential placement on restricted formularies through rebates that scale with list price, making higher prices strategically advantageous despite reduced volume. This occurs in oligopolistic therapeutic classes where PBMs (pharmacy benefit managers) accept inflated list prices in exchange for larger rebates, which offset insurer costs while entrenching market exclusivity. Contrary to the assumption that prices reflect scarcity or innovation, the driver is a perverse alignment between rebate infrastructure and tiered coverage, exposing how payer contracting structures incentivize inflation to secure access.
Therapeutic Redefinition
When insurance coverage narrows, manufacturers redefine their drugs’ clinical positioning—shifting from broad indications to narrow, high-cost patient subgroups—to justify exponential price hikes under the guise of precision medicine or orphan drug status. This reclassification leverages FDA regulatory pathways like product-specific guidances or risk evaluation strategies to lock in protected status, even when most patients remain unchanged. The critical rupture with standard market logic is that prices rise not from cost or demand pressures but from deliberate semantic and regulatory repositioning, revealing 'value' as a constructed category manipulated through clinical narrative.
Rebates Escalation Cycle
Changes in insurance formularies trigger dominant pharmacy benefit managers (PBMs) to renegotiate drug rebate contracts with manufacturers, which incentivizes manufacturers to raise list prices to preserve net revenue after rebates, thereby shifting costs to uninsured or high-deductible patients. This mechanism operates through the PBM-manufacturer rebate system, where higher rebates are tied to higher list prices, creating a feedback loop that amplifies price increases independent of production costs. The non-obvious systemic feature is that insurance coverage changes act not as direct price setters but as triggers for contractual recalibrations in a hidden financial layer dominated by rebate leverage, where pricing decisions serve contract competitiveness rather than market supply-demand equilibrium.
Formulary Exclusion Arbitrage
When insurers exclude a medication from preferred formulary tiers, specialized pharmacy networks and mail-order monopolies capture the resulting distribution bottleneck, enabling them to impose access surcharges and exclusive dispensing fees that manufacturers then absorb into inflated wholesale prices. This occurs through vertically integrated dispensing control points that emerge post-coverage change, where a small number of specialty pharmacies gain outsized pricing influence due to restricted patient access paths. The underappreciated dynamic is that formulary reclassification doesn't merely alter patient cost-sharing—it restructures the entire distribution chain, allowing intermediaries to extract rents that are recursively priced into the drug’s base cost, even for those outside the insurance system.
Indication Monopoly Spillover
When new insurance coverage expands for a specific indication of a multi-use drug, manufacturers strategically raise prices across all uses—including uncovered or off-label applications—leveraging the expanded payer guarantee in one segment to justify system-wide price repositioning. This works through internal corporate pricing algorithms that correlate reimbursement assurance with overall product valuation, effectively cross-subsidizing risk in uninsured markets using newly secured payer contracts. The overlooked systemic mechanism is that insurance changes function as valuation signals rather than mere demand stimulants, prompting firms to recalibrate prices across the entire product ecosystem in anticipation of elevated willingness-to-pay benchmarks, irrespective of actual usage patterns.
Regulatory Asymmetry
The expansion of Medicare Part D in 2006 intensified pricing leverage for pharmaceutical manufacturers by decoupling patient access from price sensitivity among insurers, amplifying post-coverage price surges. Prior to this, most elderly patients relied on cash payments or limited formularies, constraining price escalation; but with Medicare’s implicit coverage commitment and restricted negotiation rights, manufacturers could raise prices without losing volume, knowing that plan designs would absorb the cost shock. This created a structural incentive where price increases were functionally insulated from demand elasticity, transforming medication pricing into a game dominated by rebate-driven formulary placement rather than therapeutic value. The non-obvious insight is that regulatory design—not market scarcity—became the primary pricing escalator after 2006, as the trajectory of drug pricing shifted from supply-side rationing to access-driven extraction.
Rebate Trap
The shift from fee-for-service to value-based rebate contracts between drug manufacturers and PBMs after 2015 inverted the risk structure of drug pricing, making sharp post-coverage increases a rational response to contractual dependencies rather than demand shifts. Historically, price increases were tempered by volume loss, but under prevailing rebate models, manufacturers guarantee PBMs discounts tied to list price, incentivizing higher nominal prices to fund larger rebates and secure favorable placement. This transformed coverage expansion events—such as FDA approval or Medicare inclusion—into triggers for maximized pricing, not access democratization, because the financial benefit flowed upward through rebate capture, not downward through reduced patient cost. The underappreciated reality is that pricing now follows rebate optimization curves rather than therapeutic demand, a pivot point achieved only after rebates became the dominant PBM revenue model.
Formulary gatekeeping inertia
Insurers' delayed removal of legacy drugs from preferred tiers after patent expiry enables incumbent manufacturers to sustain price hikes despite generic availability. This occurs because pharmacy benefit managers (PBMs) retain outdated formulary structures that favor historical contracting relationships over cost efficiency, as seen in UnitedHealthcare’s continued privileging of branded esomeprazole (Nexium) listings years after generic entry, allowing Astrazeneca to raise prices without losing placement. The mechanism operates through institutional path dependence in PBM formulary design, where audit cycles and administrative habit delay therapeutic substitution signals, effectively insulating legacy brands from competitive pressure. This reveals that pricing power can persist not due to active preference but from passive bureaucratic delay, a dynamic rarely accounted for in models assuming rational, real-time formulary optimization.