Why Do EEOC Complaint Success Rates Hint at Healthcares Systemic Issues?
Analysis reveals 10 key thematic connections.
Key Findings
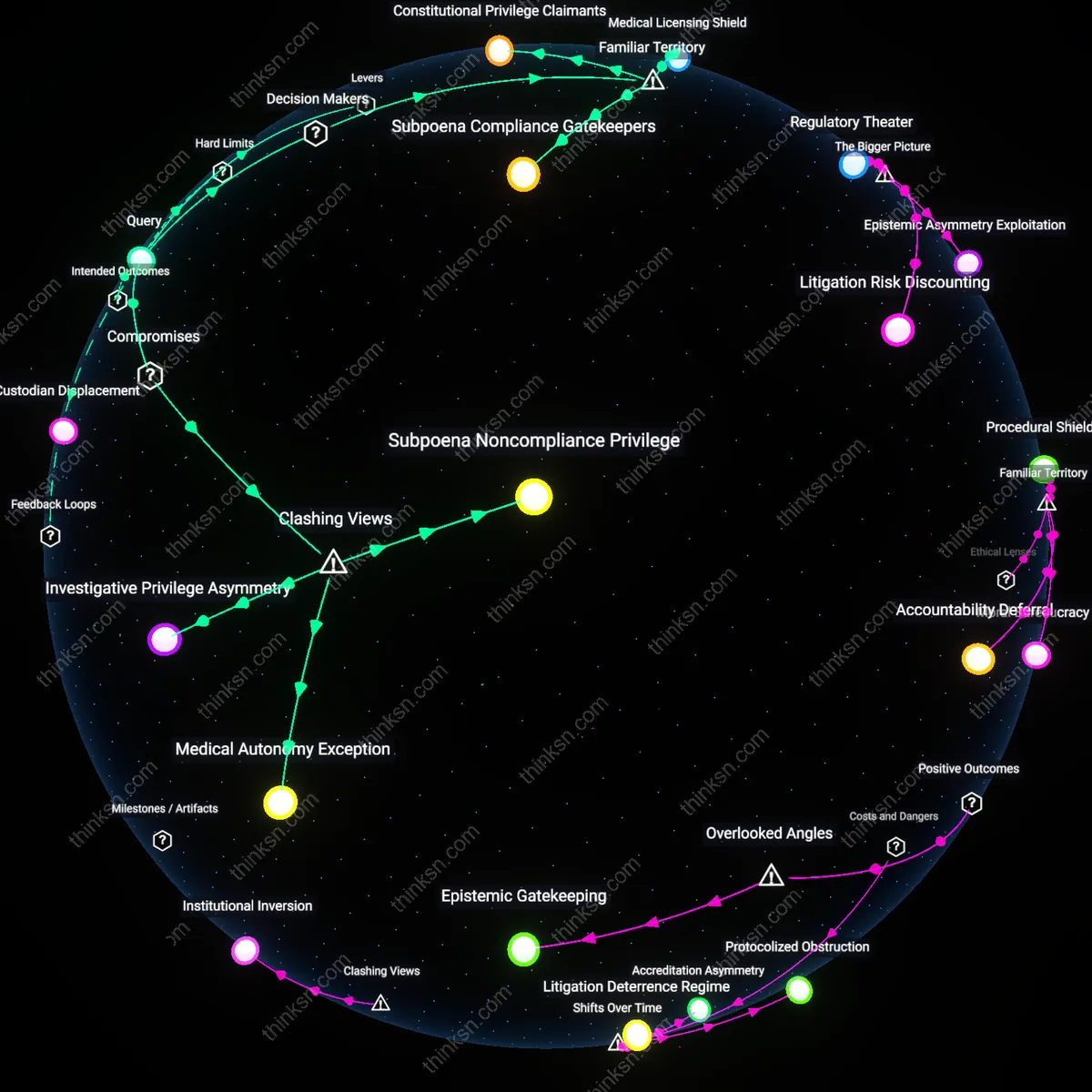
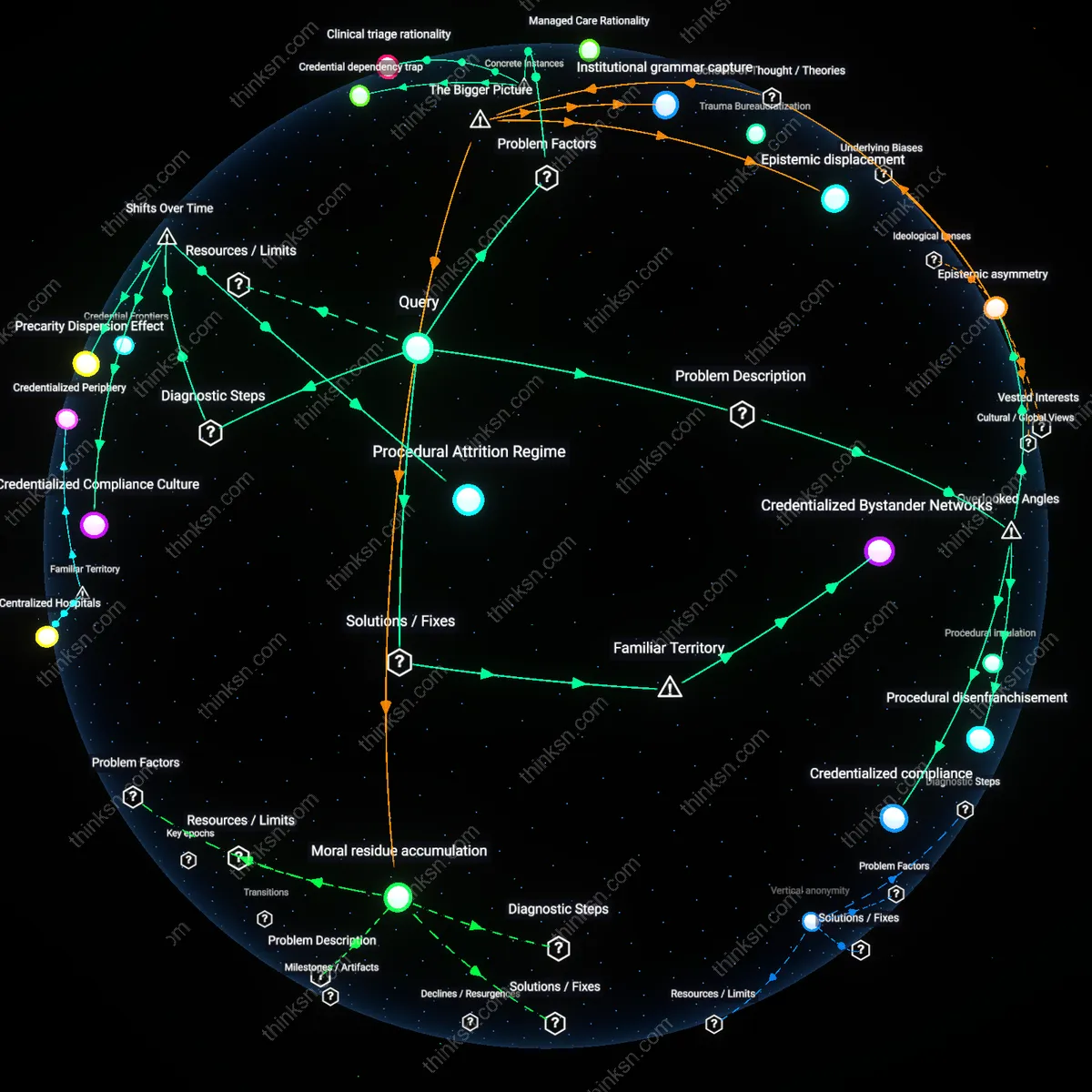
Procedural disenfranchisement
Low EEOC success rates in healthcare reflect how procedural disenfranchisement—workers' systematic exclusion from navigating complaint processes due to time poverty and administrative complexity—undermines formal protections, particularly for low-wage clinical support staff who lack union representation or managerial advocacy. These workers often face inflexible scheduling, lack paid leave to attend EEOC proceedings, and rely on transient managers who avoid involvement in long-term disputes, rendering legal rights functionally inaccessible despite their statutory existence. This reveals that the system assumes an availability of time and institutional support that most frontline healthcare workers do not have, exposing a hidden procedural barrier that invalidates access to justice even when outcomes are legally warranted. Unlike overt discrimination, this mechanism operates through neutral administrative routines that cumulatively disable claimants, a dynamic rarely captured in equity assessments focused on intent or outcome alone.
Epistemic asymmetry
Low EEOC complaint success rates in healthcare are sustained by epistemic asymmetry—where institutional actors like hospital HR departments and risk management teams systematically document, reinterpret, and preempt employee claims using clinical governance frameworks that external adjudicators defer to, even when those frameworks obscure workplace bias. Because EEOC investigators rely heavily on employer-generated personnel files, incident reports, and performance evaluations—documents shaped by internal norms that medicalize or depoliticize conflict—worker narratives of discrimination are often reframed as issues of 'clinical competency' or 'interpersonal communication,' stripping them of their civil rights dimension. This creates a credibility gap not due to worker dishonesty but because the healthcare system produces more authoritative and technically legible records than employees can match, a structural advantage rarely considered in discussions of workplace equity that assume evidentiary neutrality.
Credentialized compliance
Persistent failure of EEOC complaints in healthcare stems from credentialized compliance—the way institutions satisfy legal expectations through the symbolic adoption of DEI training, accreditation standards, and policy manuals, allowing them to appear legally defensible even when internal practices contradict those policies, particularly in decentralized settings like regional health networks. Because enforcement agencies often equate the presence of anti-discrimination policies with genuine adherence, facilities can leverage certifications from bodies like The Joint Commission as proxies for equity, even as supervisors in surgical units or long-term care wards maintain exclusionary norms unaddressed by top-down modules. This decoupling of policy performance from actual practice creates a compliance mirage that protects institutions from remediation, exposing how the very markers used to assess fairness become instruments of deflection, a phenomenon obscured in analyses that treat policy implementation as monolithic.
Supervisory retaliation infrastructure
Supervisory retaliation in California’s Kern County hospital system directly suppresses EEOC complaints by leveraging informal disciplinary channels that circumvent formal oversight. In 2018, registered nurses at Kern Medical reported filing harassment complaints only to face reassignment to night shifts, exclusion from scheduling inputs, and peer isolation—tactics that exploited ambiguities in whistleblower protections and relied on decentralized managerial discretion. This reveals how localized power structures weaponize job design and workflow control to punish dissent without triggering legal accountability, exposing a gap between anti-retaliation statutes and their enforcement within hierarchically dense clinical environments.
Credential dependency trap
The reliance on professional licensing bodies in Texas hospitals creates a parallel adjudication pathway that displaces EEOC recourse, as seen in the 2021 case of nurse Lydia Tan at Baylor St. Luke’s, whose racial discrimination complaint was diverted to the Texas Board of Nursing amid allegations of ‘unprofessional conduct’ in response. Because healthcare roles require active licensure, employers and affiliated regulators can initiate disciplinary proceedings that jeopardize employment stability without formally terminating contracts, thereby deterring federal complaints through risk escalation. This illustrates how the dual dependence on both employment and licensure enables institutional actors to outsource coercion to third-party credentialing systems, rendering EEOC protections functionally irrelevant.
Clinical triage rationality
At New York-Presbyterian Hospital in 2019, staff grievances related to pregnancy discrimination were deprioritized during staffing shortages under the justification of ‘patient care continuity,’ which administrators formalized through shift-allocation algorithms that privileged seniority and availability metrics insensitive to ADA or Title VII accommodations. This operational prioritization embeds equity concerns as secondary to clinical workflow demands, transforming legal mandates into negotiable administrative preferences. The case reveals how performance-driven operational doctrines—like triage rationality—recursively define legitimate organizational attention, systematically excluding identity-based harms from intervention thresholds despite statutory requirements.
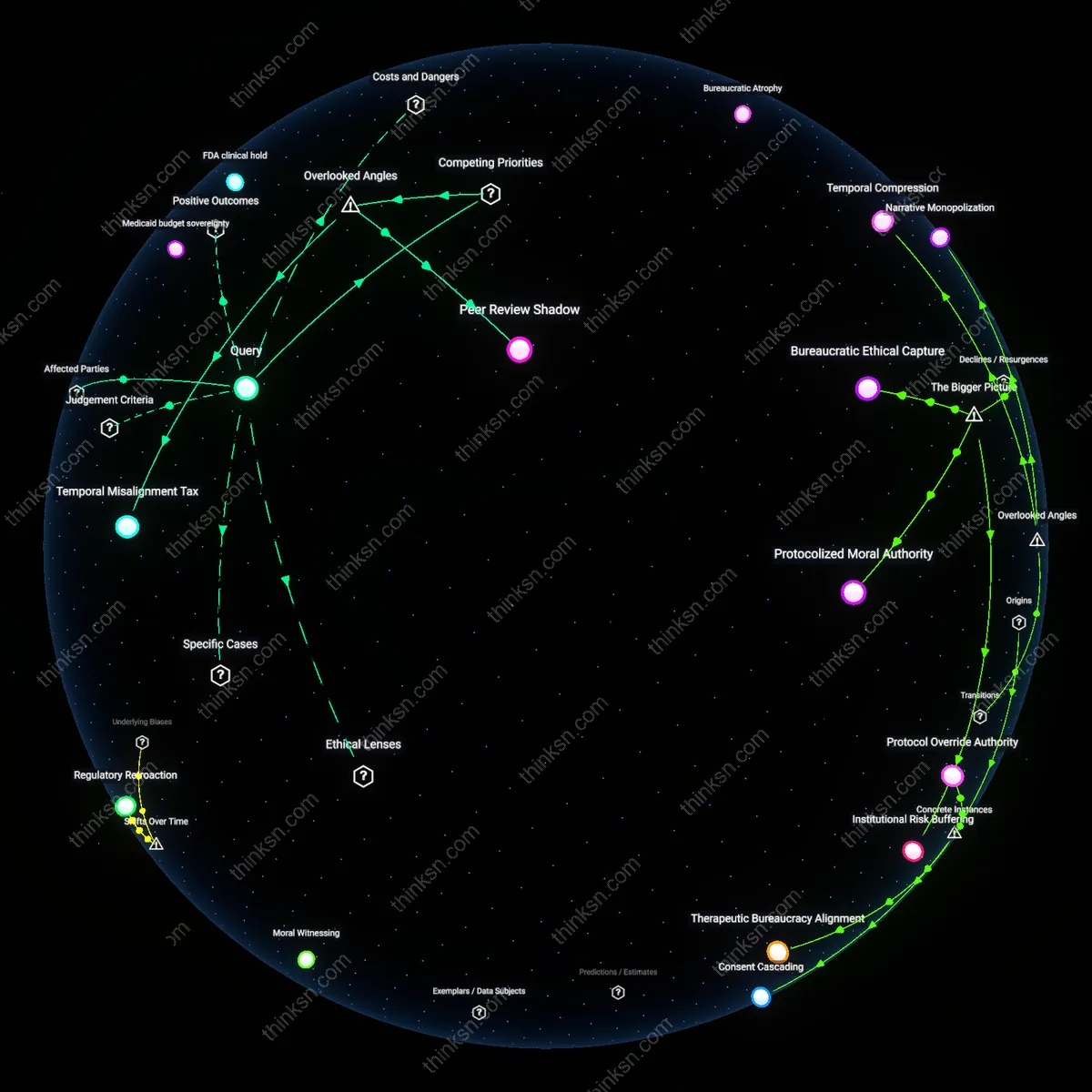
Procedural Attrition Regime
Declining EEOC complaint success rates since the 1990s reflect a shift from overt discrimination to procedural dismissal, where formal legal access remains but evidentiary thresholds and administrative delays filter out claims before adjudication; this mechanism operates through case backlog management and summary dismissal protocols in federal intake offices, privileging employer documentation over worker testimony. The non-obvious insight is that the system did not regress—it evolved toward efficiency metrics that equate case closure with resolution, making attrition a feature, not a flaw, of modern civil rights enforcement.
Credentialized Compliance Culture
The rise of institutional compliance frameworks after the 2000s transformed healthcare workplaces into environments where anti-discrimination policies are visibly codified but functionally insulated from employee redress, shifting the barrier from legal absence to performative accountability; hospitals and clinics now deploy mandatory training and internal review boards that substitute procedural compliance for substantive change. The overlooked consequence is that this shift neutralized regulatory pressure by making documentation of action—rather than outcomes—the benchmark of equity, thereby depoliticizing worker grievances into administrative errors.
Precarity Dispersion Effect
Since the 2010s, the fragmentation of healthcare labor through subcontracting, gig staffing platforms, and part-time roles has decentralized employment relationships, shifting systemic vulnerability from workplace-specific discrimination to structural invisibility in EEOC eligibility; workers employed via third-party agencies fall outside direct employer liability, making claims technically nonviable despite identical working conditions. The underappreciated dynamic is that legal protections have not eroded—they have been spatially bypassed by employment architectures that predate liability by design, rendering traditional civil rights mechanisms obsolete for growing segments of the workforce.
Credentialized Bystander Networks
Mandate union-credentialed peer advocates on every hospital floor trained to document and co-sign discrimination incidents before formal EEOC filing. These advocates—experienced technicians or senior CNAs—use standardized field logs accepted as preliminary evidence by state labor boards, transforming the familiar image of coworker solidarity into a procedural checkpoint that disrupts the isolation of targets. The underappreciated element is that trust resides not in institutions but in occupational kinship, and by formalizing informal support, the system leverages existing relational infrastructure instead of replacing it with top-down oversight.