Who Profits as Clinics Cut In-Person Care for Anxiety?
Analysis reveals 9 key thematic connections.
Key Findings
Insurance Reimbursement Arbitrage
Private equity-owned telehealth platforms benefit financially by aligning service delivery with insurer reimbursement structures that favor short, video-based consultations over longer in-person visits, which triggers a shift in clinical protocols toward faster patient turnover. This mechanism operates through contractual leverage between large mental health chains and commercial payers, where telehealth codes are easier to standardize and bill at scale, reducing administrative friction and increasing margin. The non-obvious consequence is that clinical workflows adapt to billing efficiency, not therapeutic need, particularly disadvantaging anxiety patients who require longer stabilization periods that are less profitable under this model.
Urban Real Estate Divestment
Mental health systems that replace physical clinics with telehealth infrastructure reduce overhead by liquidating urban real estate holdings, transferring capital gains to institutional investors and hospital-affiliated financial trusts. This shift is sustained through municipal zoning incentives and deferred maintenance costs, allowing providers to recoup sunk property investments while reclassifying care delivery as 'low-footprint.' The underappreciated dynamic is that this geographic withdrawal destabilizes continuity for anxiety patients in dense, low-income neighborhoods where broadband access and private digital space are scarce, effectively rationing care through spatial disinvestment rather than clinical triage.
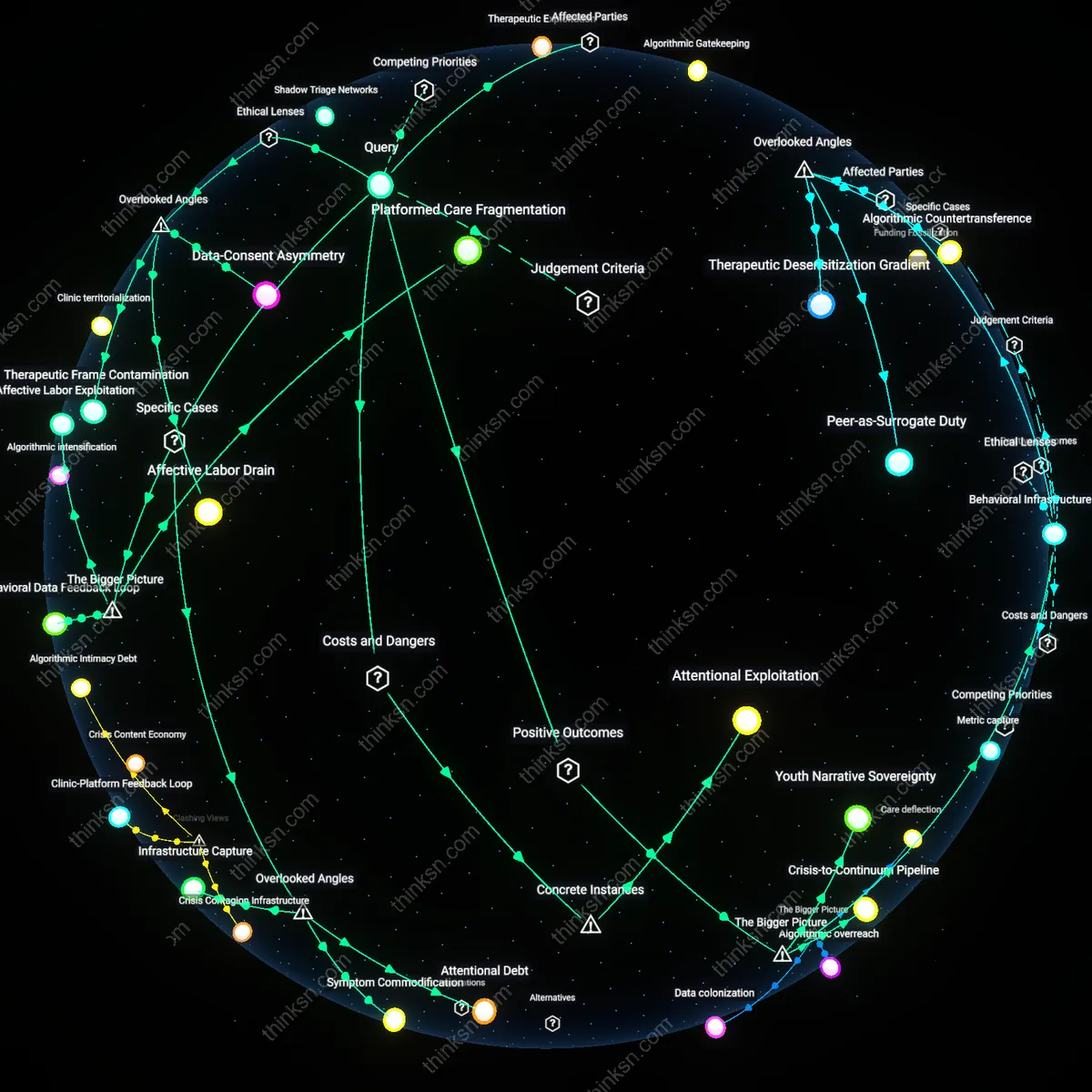
Algorithmic Triage Escalation
Digital health vendors profit from telehealth expansion by embedding proprietary intake algorithms that classify mild anxiety as 'telehealth-appropriate,' increasing patient volume while offloading severe cases to public systems. This mechanism functions through integration with electronic health records and employer-based wellness contracts, where success metrics emphasize throughput and cost avoidance, not remission rates. The overlooked systemic effect is that anxiety conditions requiring nuanced, embodied therapeutic cues—like micro-avoidance behaviors—are misclassified as manageable remotely, reinforcing a feedback loop where platform profitability depends on under-detection of complexity.
Billing code elasticity
Insurance reimbursement structures that assign equivalent or higher relative value units to telehealth CPT codes amplify provider adoption of virtual care irrespective of clinical appropriateness. This financial mechanism—tied to Medicare’s temporary 2020 telehealth flexibilities later preserved in commercial plans—means clinics generate more revenue per clinician hour by scheduling back-to-back telehealth sessions without accounting for travel or facility overhead, creating a margin drift toward efficiency over therapeutic fidelity. The non-obvious factor is that anxiety treatment degradation isn't due to telehealth's inherent inadequacy but to a reimbursement-induced compression of session length and clinician availability, which erodes exposure therapy dosing and rapport continuity—dimensions rarely tracked in quality audits.
Digital choreography burden
Patients with generalized anxiety disorder experience increased pre-session cognitive load when required to troubleshoot unstable broadband, manage platform permissions, or secure private physical space—conditions that amplify somatic arousal before therapeutic engagement. This invisible labor, unmeasured in clinical outcomes but structurally enforced by telehealth’s technical dependencies, shifts part of the treatment burden onto the patient’s self-regulatory capacity, which is precisely the function impaired by anxiety. What escapes standard cost-benefit analyses is that telehealth’s economic efficiency for clinics is partially subsidized by the patient’s environmental and executive stability—an asymmetry that disproportionately degrades care quality for low-income or household-saturated demographics.
Telehealth Capital Formation
Investors in digital health infrastructure financially benefit from mental-health clinics prioritizing telehealth, because venture capital and private equity increasingly channeled funds into scalable, data-extractive therapy platforms after the 2020 virtual care surge, a shift enabled by regulatory loosening during the pandemic that transformed reimbursement models—this financialization has progressively decoupled service delivery from long-term therapeutic continuity, especially for anxiety patients who require stable, embodied rapport; what is underappreciated is how this era of emergency improvisation became institutionalized into a profit-centered care logic that treats sporadic virtual access as equivalent to sustained treatment efficacy.
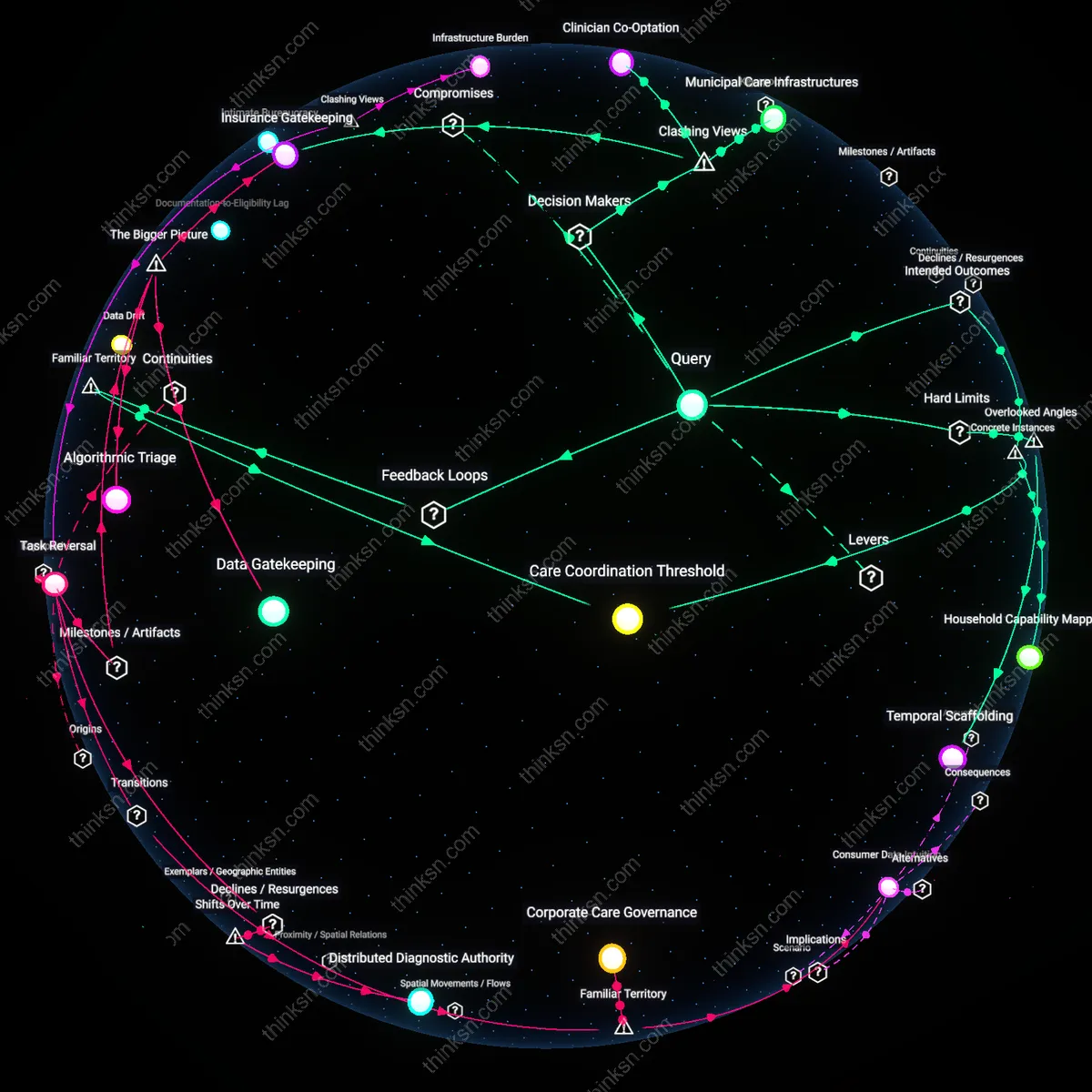
Reimbursement Realignment Regime
Insurance corporations financially benefit from mental-health clinics prioritizing telehealth, because post-Affordable Care Act shifts toward value-based billing created incentives to reimburse time-limited, metrics-driven visits that are easier to automate and monitor remotely than in-person sessions, enabling actuarial control over utilization; the transition from fee-for-service to episode-based payment models after 2014 entrenched a new bottleneck—care must be documented in discrete, billable units—which disadvantages the open-ended, process-oriented work often needed for anxiety, revealing how clinical quality became constrained by administrative legibility rather than patient outcomes.
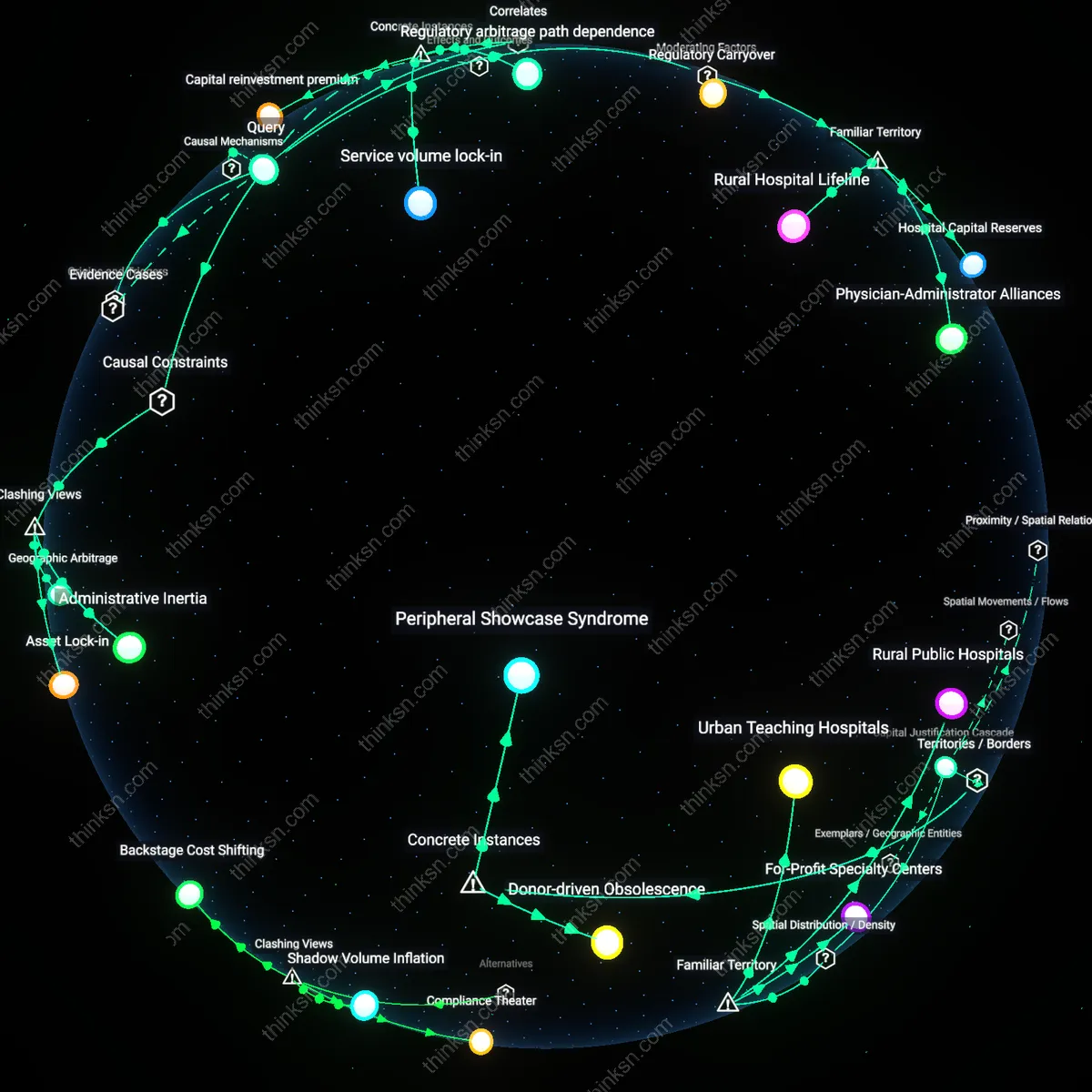
Geospatial Care Abandonment
Pharmaceutical firms financially benefit from mental-health clinics prioritizing telehealth, because the post-2010 erosion of community-based psychiatric clinics—particularly in rural and low-income urban areas—shifted treatment emphasis from relational continuity to medication management delivered via remote consultations, a transition that elevated drug adherence as the primary metric of care success; this spatial disinvestment created a bottleneck where telehealth access assumes internet reliability and self-regulation capacity, systematically disadvantaging anxiety patients with environmental instability, thus exposing a residual reliance on pharmacological solutions in the absence of embodied therapeutic support.
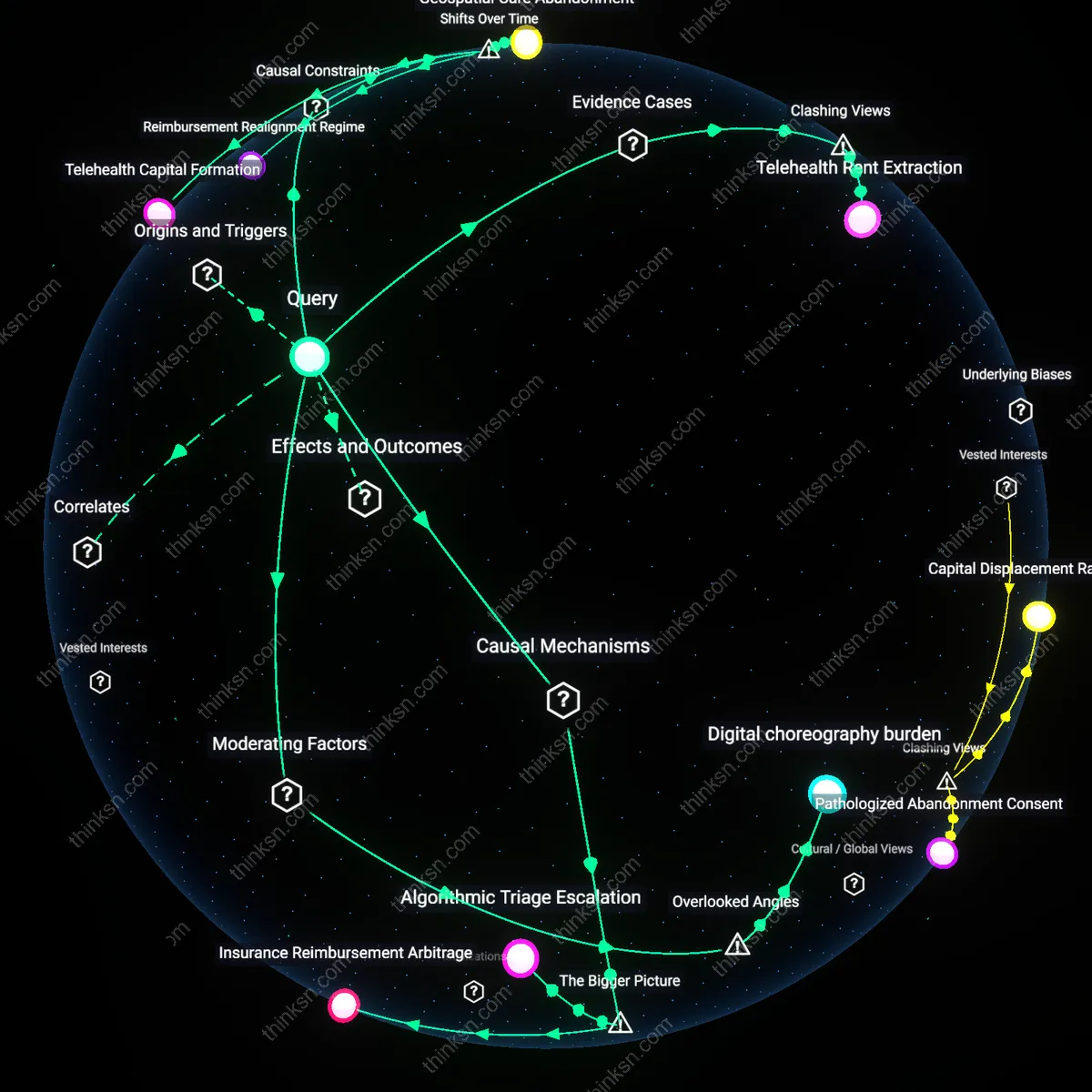
Telehealth Rent Extraction
Private equity firms like Sheridan Capital and healthcare systems such as Teladoc profit most from scaling telehealth at the expense of in-person care because they monetize patient volume through standardized, asynchronous therapy models that reduce labor costs and extend market reach. This financialization shifts treatment for anxiety toward scripted, algorithm-driven interactions that degrade therapeutic rapport—evident in the 2023 Ginger.io bankruptcy, where investor demands for growth outpaced clinical oversight, ultimately collapsing care quality under unregulated expansion. The non-obvious insight is that telehealth's economic benefit isn't primarily to insurers or platforms alone, but to distant capital allocators who treat mental health access as an arbitrage opportunity, distorting care intensity for extractive returns.