How to Honor a Parents Wishes While Protecting Family Wealth?
Analysis reveals 8 key thematic connections.
Key Findings
Intergenerational equity
Siblings should prioritize long-term care funding over estate preservation because doing so upholds intergenerational equity, a principle of distributive justice that weights the moral claims of dependent elders and future familial generations equally. This judgment rests on the practical reality that aging parents have already borne the cost of raising children and transferring initial wealth, and systemic underfunding of public elder care shifts moral and financial responsibility to families. The non-obvious implication is that protecting wealth at the expense of care reproduces a covert transfer of risk from state to kin, undermining the very solidarity wealth is meant to sustain. The residual concept this reveals is intergenerational equity—how obligations across age-cohorts recalibrate fairness within family financial decisions.
Fiscalization of care
Siblings should restructure asset management to treat care spending as a necessary fiscal outlay rather than an estate threat, applying economic efficiency principles that treat parental care as human capital maintenance essential to family stability. This approach operates through mechanisms like pooled sibling trusts or Medicaid-compliant annuities, which exploit gaps between private cost burdens and public eligibility rules, revealing that the U.S. healthcare-financing system actively incentivizes wealth depletion as a condition for care access. The underappreciated reality is that long-term care financing functions as a de facto means-tested welfare system that penalizes asset retention, making strategic disbursement not just pragmatic but systemically coerced. The residual concept this uncovers is the fiscalization of care—how caregiving becomes a regulated financial transaction embedded in bureaucratic eligibility structures.
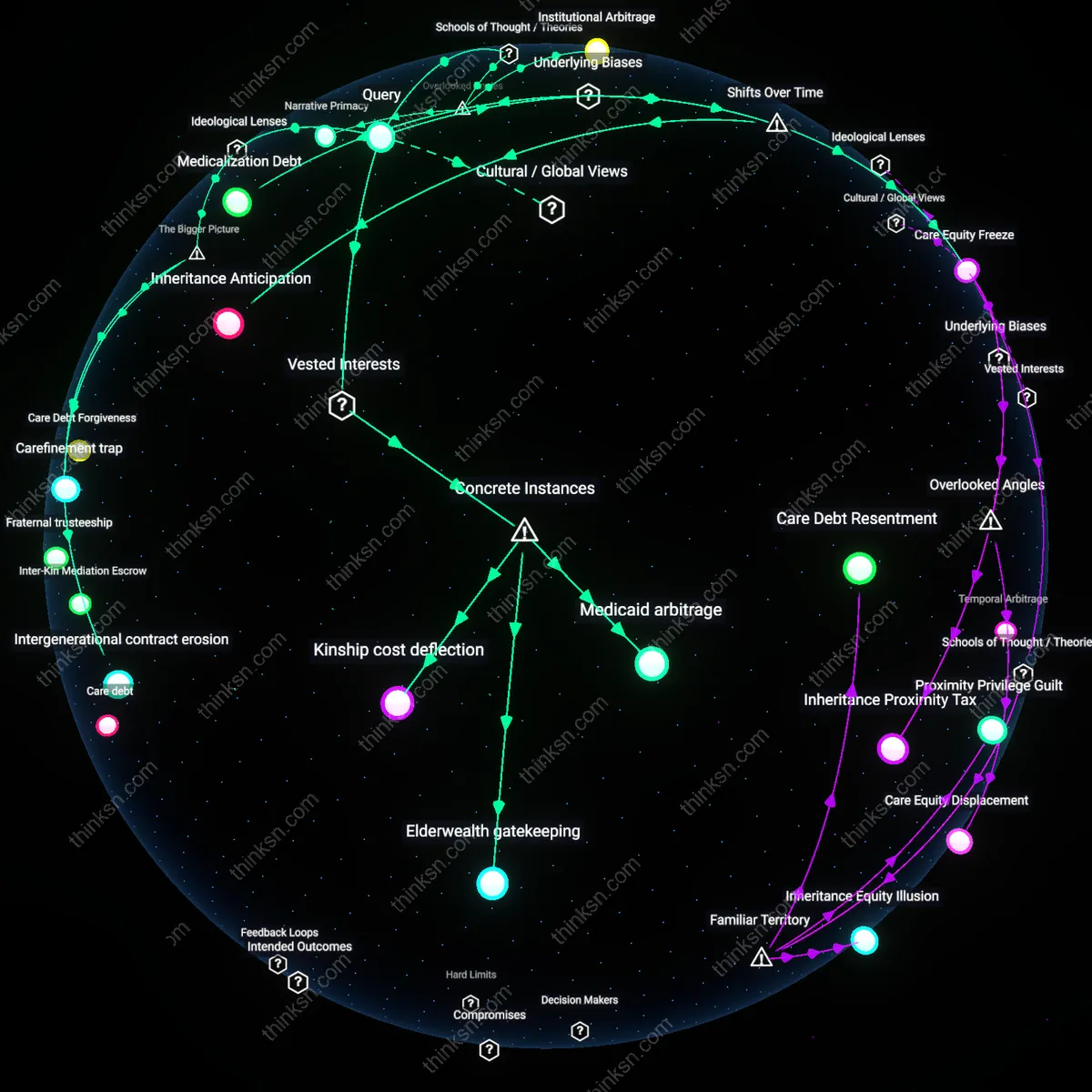
Kin-based risk absorption
Siblings should accept partial erosion of family wealth as the necessary cost of fulfilling their role as primary risk absorbers within a privatized eldercare regime, where practical autonomy for parents depends on familial financial sacrifice due to systemic underinvestment in public support infrastructure. This claim emerges from the structural reality that U.S. social policy defaults to kin networks when formal safety nets fail, placing siblings in the position of de facto insurers who internalize costs that macroeconomic trends—rising healthcare inflation, stagnant wages, and regional care deserts—have externalized onto households. The non-obvious insight is that estate depletion is not a failure of planning but an expected outcome of policy design that subsidizes family absorption of systemic risk. This reveals kin-based risk absorption—the mechanism by which informal family units stabilize broader economic instabilities through unpaid or under-resourced care labor and asset surrender.
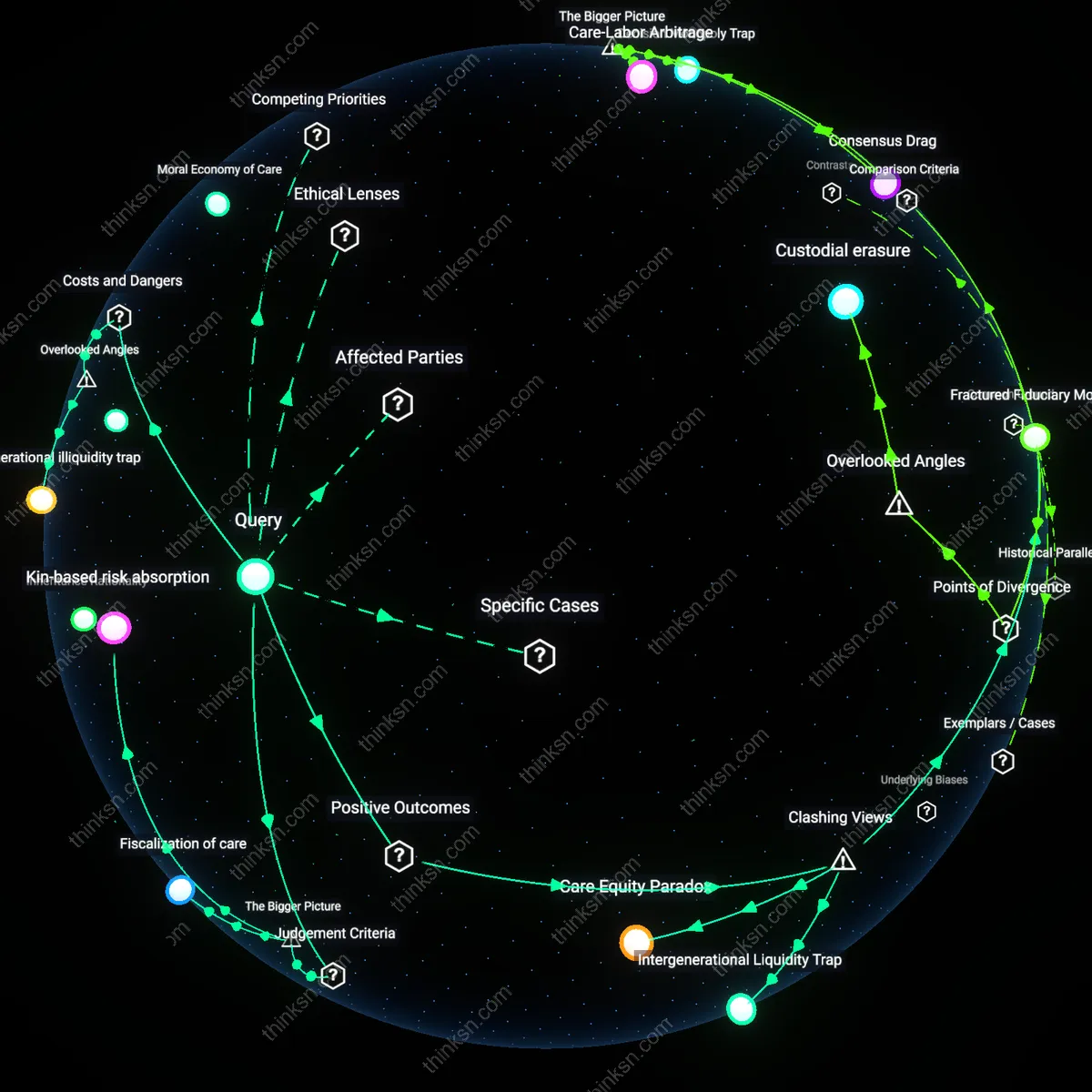
Care Equity Paradox
Siblings should prioritize transparently allocating care responsibilities over equal financial division to preserve both dignity and wealth, because unequal but need-based caregiving contributions prevent resentment and free up resources. When one sibling provides daily care while others contribute capital, the system functions more efficiently than equal financial cost-sharing, yet this asymmetry is culturally misread as unfair—revealing how equity in outcome is mistaken for equity in input. The non-obvious insight is that protecting family wealth does not require cost minimization, but rather the strategic redistribution of obligations to match capacities, which sustains both care quality and familial cohesion.
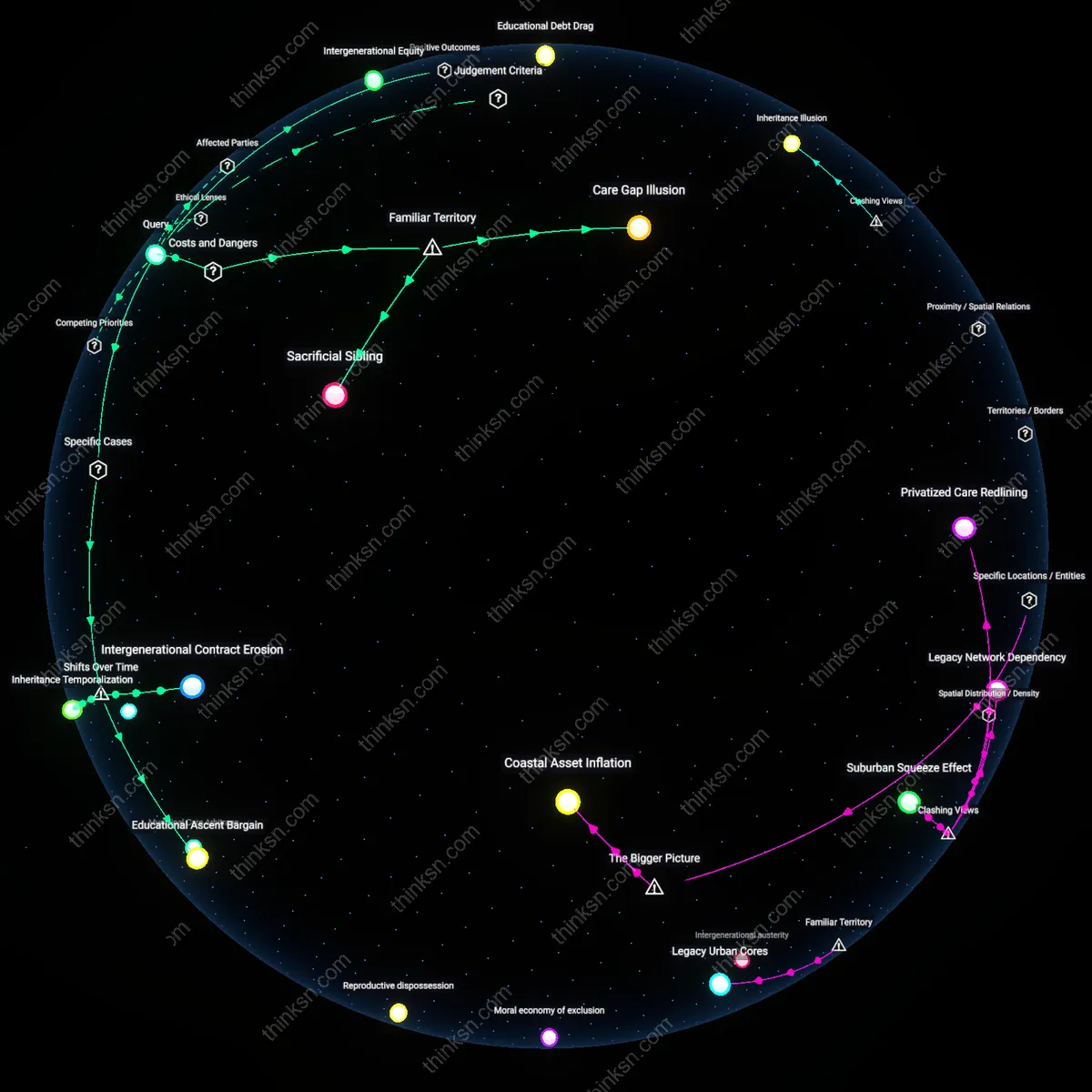
Intergenerational Liquidity Trap
Treating the parent’s home as an untouchable asset to be preserved for inheritance ensures its eventual forced liquidation under crisis conditions, whereas proactively monetizing it to fund high-quality care generates better outcomes for all. Many families cling to property as symbolic of legacy, but this deferral of liquidity often leads to rapid, low-value sales during medical emergencies—undermining both care and wealth. The counterintuitive mechanism is that controlled, early conversion of illiquid assets into care funding prevents wealth dissipation through inefficient late-stage spending, exposing the trap of sentiment-driven asset preservation.
Fractured Fiduciary Model
Appointing a single sibling as the legal and financial decision-maker—vested with sole authority over care spending—produces more disciplined resource use and higher care quality than consensus-based group management. Contrary to the expectation that shared control prevents abuse, sibling committees often devolve into avoidance, denial, or escalation due to conflicting emotional stakes, while a designated fiduciary internalizes long-term accountability. This structured concentration of power reduces transaction costs in care decisions and prevents passive wealth erosion through indecision—revealing that distributed moral responsibility enables financial drift.
Intergenerational illiquidity trap
Siblings must reject the assumption that preserving family wealth and funding parental care are directly competing goals, because the real danger lies in the illiquidity of inherited assets during care crises. Most family wealth is locked in homes or retirement accounts that cannot be accessed without triggering taxation, sale, or penalties—precisely when cash is needed for in-home care or facility placement. This creates a crisis dynamic where siblings either drain liquid savings meant for their own retirement or liquidate assets under duress, increasing total systemic cost through inefficient fire sales or Medicaid spend-down maneuvers. The overlooked variable is time-bound illiquidity, not total net worth—wealth is present but inaccessible when needed most, making otherwise solvent families appear impoverished under rigid public benefit eligibility rules.
Medicalized home equity drain
Families must recognize that long-term care costs often manifest not as medical bills but as structural erosion of home equity through forced modifications, co-purchasing of adaptive equipment, or permanent renovation, which simultaneously reduces asset value for future sale while failing to qualify as tax-deductible medical expenses. When a parent requires a wheelchair ramp, stairlift, or full-bathroom retrofit, these costs are rarely covered by insurance and depreciate the home rather than enhancing market value, especially in aging neighborhoods where accessibility upgrades deter typical buyers. This creates a hidden tax on family wealth where homes are medically repurposed into semi-clinical spaces, reducing liquidity and sale appeal just as siblings anticipate recouping investment. The overlooked mechanism is the dual depreciation—functional and financial—of dwelling spaces transformed by care, a loss invisible in standard estate planning but devastating in aggregate.