The Medicaid Spend-Down Race Straining Family Bonds?
Analysis reveals 9 key thematic connections.
Key Findings
Caregiver Burden Multiplier
Medicaid eligibility requires seniors to deplete assets like savings and property before qualifying, forcing families to spend down resources on extended nursing home care, which transfers financial responsibility onto adult children—especially women—triggering role reversals, intergenerational conflict, and emotional strain that mirrors elder abandonment even when care is provided diligently; this burden is amplified because the system incentivizes impoverishment as a condition of support, making responsible caregiving feel indistinguishable from financial self-sabotage, a tension most families expect but are unprepared to endure. The non-obvious reality is that the ritual of spending down assets doesn't just reflect economic stress—it actively constructs the caregiver’s identity through sacrifice, making overwork and personal loss feel like moral obligations rather than systemic impositions.
Kinship Financial Shadowing
When one family member must liquidate assets to meet Medicaid’s resource thresholds—such as selling a home or closing a retirement account—other relatives often reallocate their own budgets silently to cover the gap, creating informal financial networks that absorb risk without documentation or recognition, operating through unspoken expectations among siblings and cousins to 'step in' when state thresholds force individual destitution; this produces cascading adjustments in homebuying, retirement plans, and educational investments across the kin group, which remain invisible to policymakers but are highly predictable in working-class and rural communities where collective survival norms persist. The underappreciated effect is that Medicaid’s asset rules don’t just target individuals—they draft entire extended families into covert fiscal partnerships, reinforcing the familiar idea that 'family helps family' while eroding the financial autonomy of those who never formally consented to the arrangement.
Elderhood Poverty Pathway
The requirement to exhaust personal assets before Medicaid eligibility creates a socially accepted pipeline from middle-class stability to state-dependent indigence in late life, conditioning families to view nursing home admission as the inevitable outcome of aging, not illness or need, but financial depletion—this narrative reshapes family planning, encouraging adult children to delay their own savings in favor of reserving liquidity for parental crises, reinforcing the belief that old age equals destitution by design. The system’s predictability makes the descent into poverty feel like a natural lifecycle stage rather than a policy artifact, with the non-obvious consequence that families emotionally prepare for loss of wealth as part of 'responsible' aging, normalizing economic decline as synonymous with dignity in elderhood.
Caregiver Surplus
The 1987 OBRA amendments, which formally recognized spousal impoverishment protections, shifted long-term care planning from institutional reliance to home-based family support, increasing informal caregiving burdens among adult children. As Medicaid allowed community-dwelling spouses to retain more assets, families reorganized intergenerational economic strategies around anticipatory asset depletion, converting liquid savings into non-countable resources like home equity. This transition embedded financial sacrifice into familial roles, transforming expected care into a de facto inheritance advance, where adult children absorbed both emotional and labor costs years before inheritance would typically transfer, revealing an intergenerational subsidy that operates outside formal accounting.
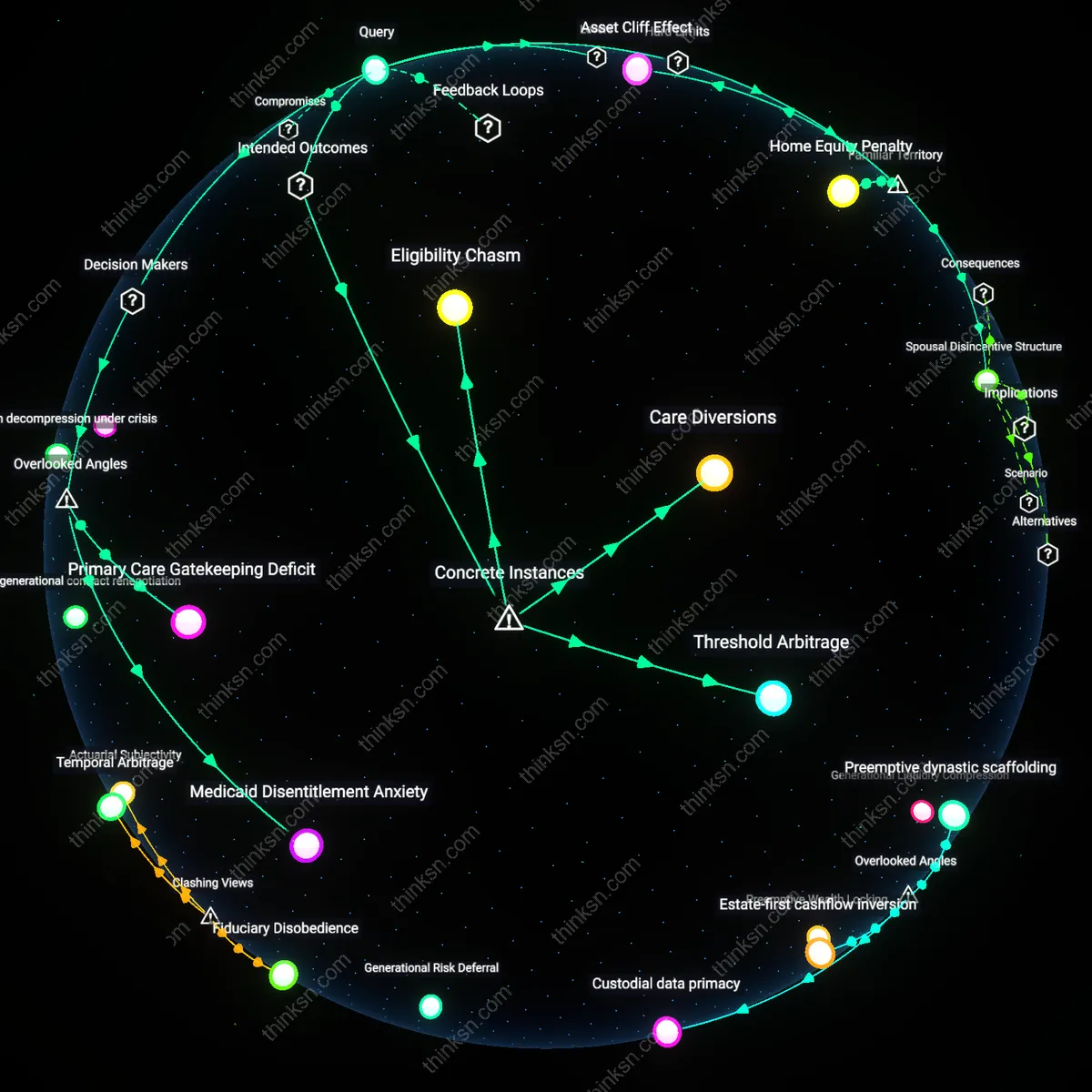
Medicalized Poverty Threshold
The expansion of Medicaid under the ACA in 2014 redefined the financial tipping point at which middle-class families must consider asset reduction to access care, altering the emotional calculus of ‘downward mobility.’ Unlike pre-2000 means-testing, which targeted entrenched poverty, post-ACA thresholds created a new liminal class—families earning above pre-ACA Medicaid limits but below cost-of-care realities—who now face deliberate impoverishment as a strategic necessity. This shift produced performative destitution, where families navigate not chronic pauperism but a procedural descent engineered to satisfy eligibility rules, intensifying intrafamilial conflict tied to staged wealth surrender rather than organic decline.
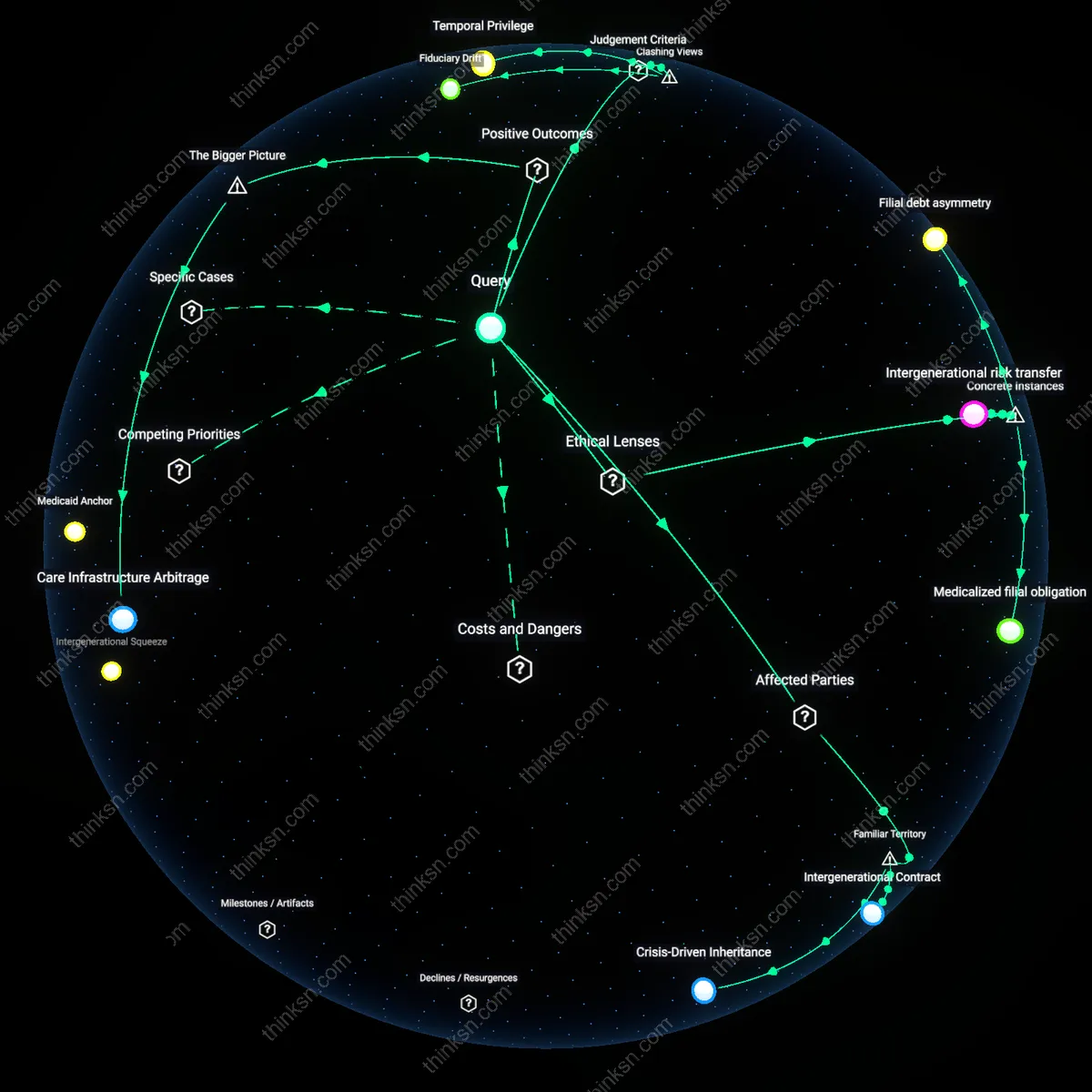
Inheritance Deferral
The 1993 federal imposition of the ‘look-back’ period for asset transfers reshaped family financial timelines by legally equating generosity with fraud, converting inter vivos gifts into probationary events subject to retrospective penalties. This created a generational time lag in wealth transmission, where parents needing care must now prove five years of financial restraint, effectively freezing customary transfers and binding children to longer periods of economic stasis. The rule turned anticipated inheritance into a suspended claim, producing intergenerational distrust when siblings interpret asset-spending plans as favoritism or miscalculation, not because of cultural shifts but because the legal timeline of eligibility now overrides familial expectations of timing.
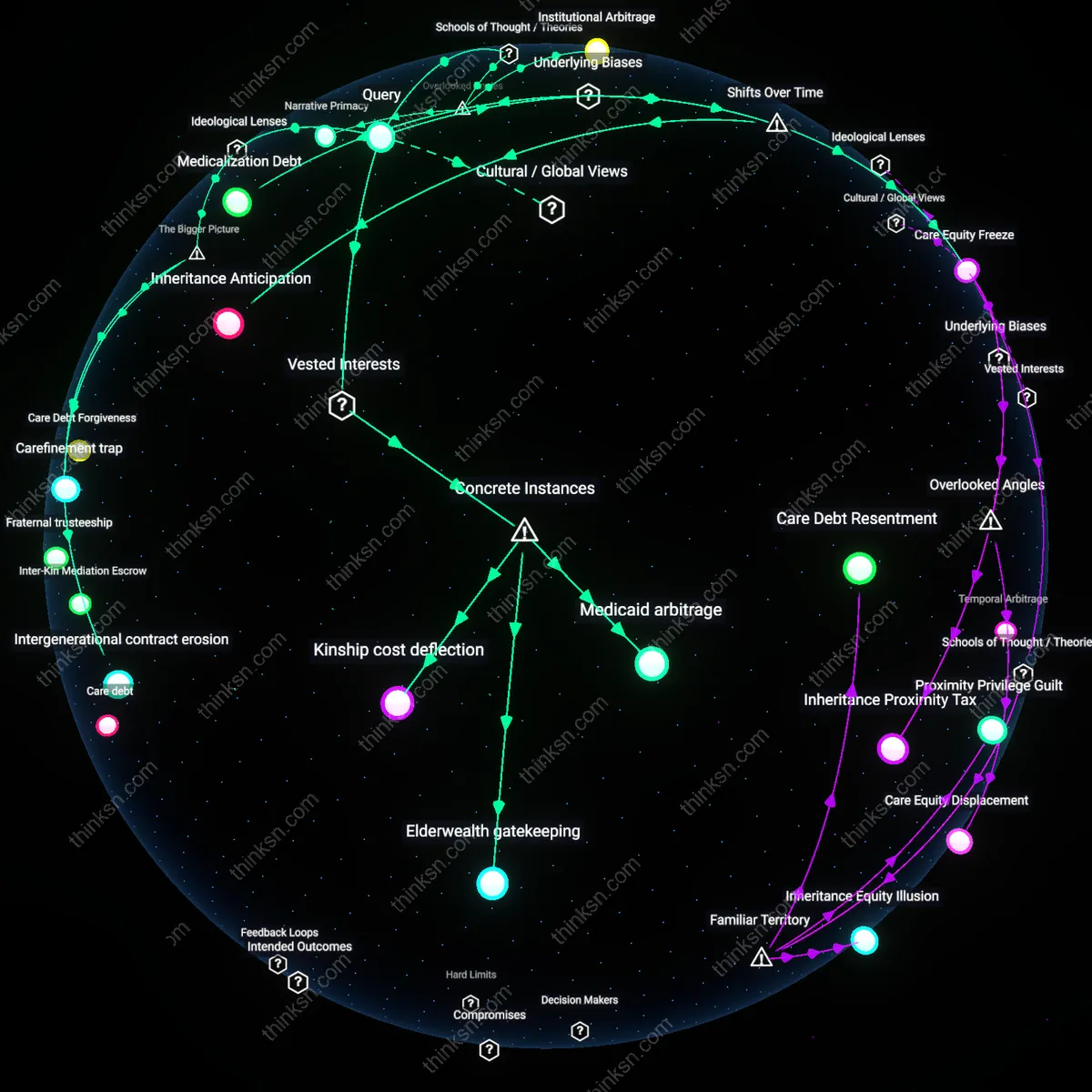
Medicaid spend-down trap
In Florida’s long-term care system, elderly patients must exhaust nearly all personal assets—such as savings, homes, or investments—before qualifying for Medicaid coverage, forcing families into state-mandated spend-downs that convert liquid wealth into non-countable resources like home renovations or prepaid burials; this artificial depletion of intergenerational wealth creates coercive financial decisions that strain familial trust, particularly when siblings disagree on allocation, revealing how eligibility rules institutionalize kinship conflict as a prerequisite for care access.
Spousal impoverishment paradox
Under Missouri’s Medicaid spousal impoverishment rules, community spouses are legally restricted in how much monthly income and assets they can retain when their partner enters nursing home care—often capped at $3,000 in liquid assets in 2015—compelling families to restructure ownership, sell property, or divert income in ways that destabilize marital economic autonomy; this bottleneck forces caretaking spouses into financial precarity as a condition of eligibility, exposing how asset limits convert marital solidarity into actuarial liability.
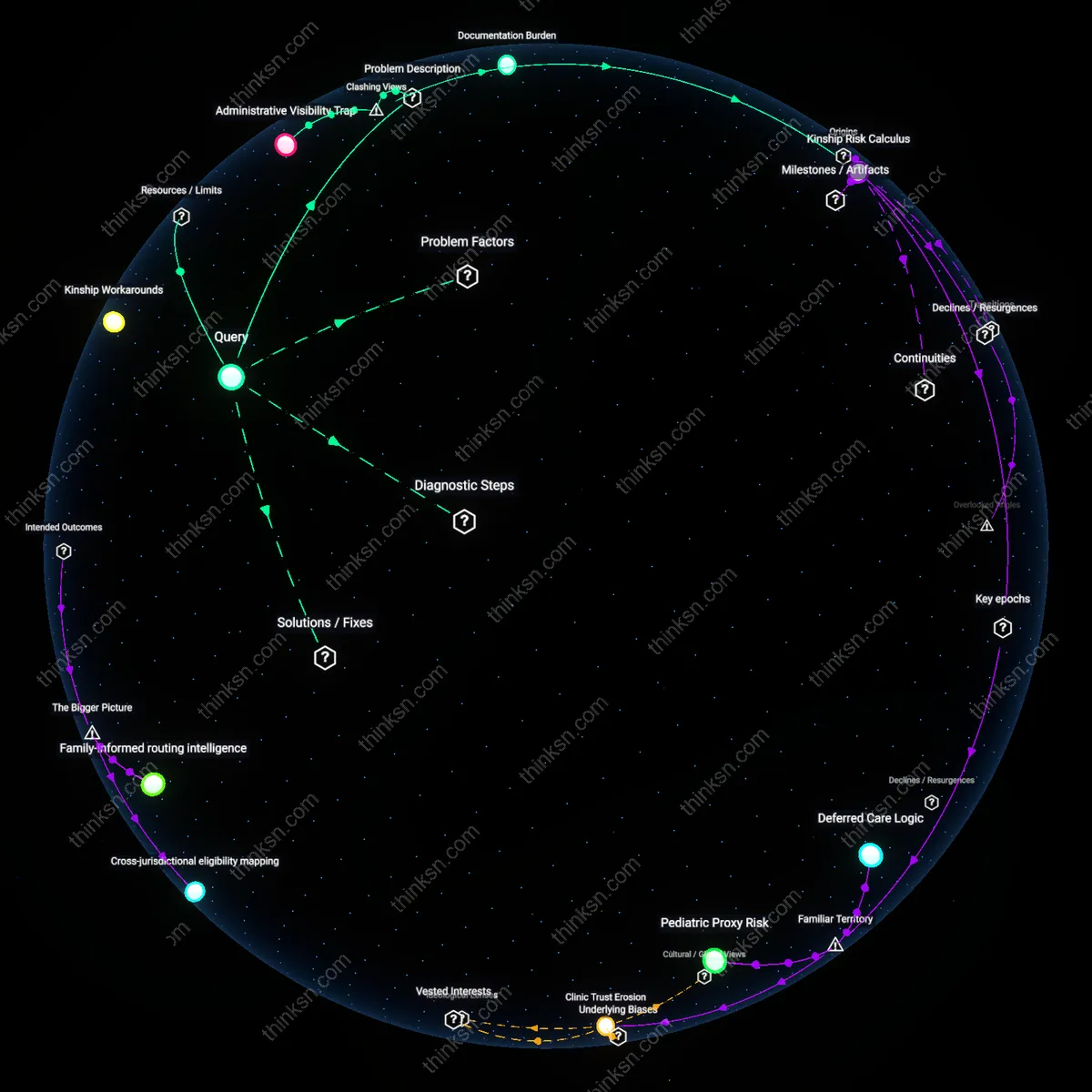
Kin-based compliance burden
When Michigan’s Department of Health and Human Services required adult children in 2018 to verify that parents had fully liquidated retirement accounts and real estate before approving Medicaid applications for home- and community-based services, family members became de facto auditors of parental wealth, entangling emotional caregiving with bureaucratic enforcement; this institutional outsourcing of eligibility verification onto relatives transforms private trust into public accountability, making familial roles instrumental to administrative compliance rather than care provision.