Formulary Leverage
Insurers steer patients toward older, generic disease-modifying antirheumatic drugs (DMARDs) like methotrexate in rheumatoid arthritis rather than biologics, due to formulary restrictions that require step therapy and prior authorization—mechanisms administered by pharmacy benefit managers (PBMs) that enforce cost containment through delayed access. This steering persists despite evidence that early biologic use can reduce long-term joint damage and disability, because the financial burden of biologics falls disproportionately on insurers in the short term, creating a misalignment between clinical timing and reimbursement incentives. The non-obvious consequence is that insurers effectively shape treatment sequencing not through explicit denial but through procedural friction, transforming clinical pathways into financial triage systems.
Reimbursement Arbitrage
In type 2 diabetes, insurers increasingly cover SGLT2 inhibitors and GLP-1 receptor agonists only after patients demonstrate cardiovascular or renal comorbidities, privileging drugs with secondary risk reduction labels over glycemic control alone, even when newer agents like tirzepatide show superior hemoglobin A1c reduction. This preference is driven by CMS reimbursement models that tie insurer payments to hospitalization rates and chronic complication outcomes, making drugs that defer end-stage renal disease or heart failure more economically valuable in value-based care contracts. The underappreciated dynamic is that insurers are not merely cost-avoidant but are actively gaming risk-adjusted payment systems, selectively adopting innovations that offset downstream liabilities rather than optimize immediate metabolic health.
Clinical Pathway Capture
Insurers collaborate with integrated delivery networks to embed coverage rules directly into electronic health record (EHR) decision support tools, making treatment recommendations for diabetes and rheumatoid arthritis appear clinically autonomous while being shaped by behind-the-scenes payer-provider data-sharing agreements influenced by UnitedHealth’s Optum and similar vertically integrated entities. These pathways default to insurer-preferred therapies by flagging non-preferred options as ‘high-cost’ or ‘non-formulary’ at the point of prescribing, effectively outsourcing rationing to clinicians under time pressure. The overlooked mechanism is that clinical autonomy is being subtly redistributed—not through overt denial, but through the algorithmic framing of choice, where payer logic becomes indistinguishable from medical judgment.
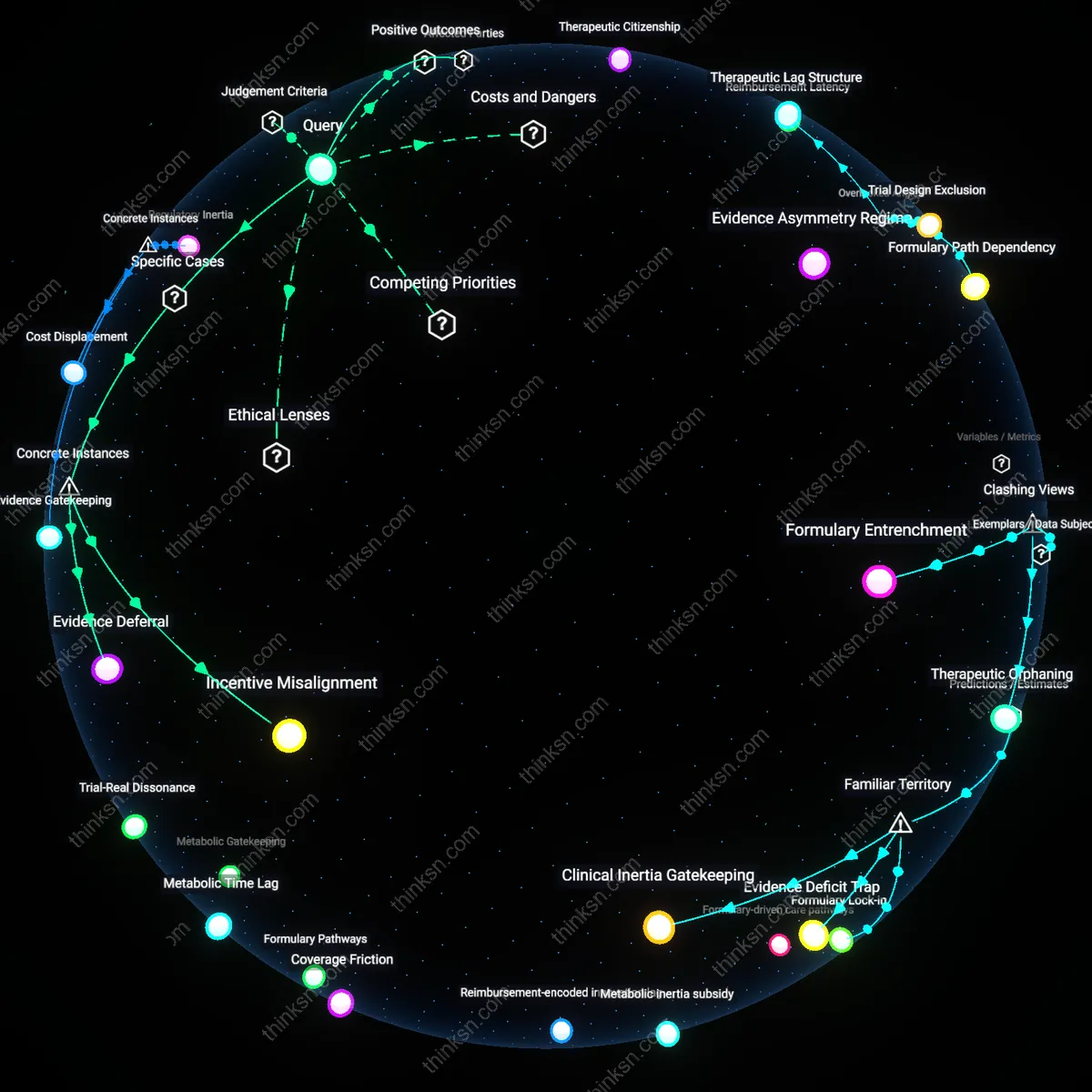
Formulary-driven care pathways
In Louisiana, Medicaid’s prescription drug program restricts coverage of biologic DMARDs for rheumatoid arthritis to patients who first fail on multiple older, cheaper agents like methotrexate and sulfasalazine, steering patients toward a step-edition protocol rooted in cost containment. This sequential logic embeds insurers’ financial logic into clinical timelines, delaying potent therapies despite evidence indicating earlier biologic use can reduce long-term joint damage and disability. The mechanism—insurer-mandated treatment ladders—reveals how coverage policies function as de facto clinical guidelines, prioritizing fiscal durability over disease modification speed, a tension often obscured by claims of evidence-based care.
Metabolic inertia subsidy
In Ohio, certain private insurers affiliated with regional Blue Cross Blue Shield plans maintain lower copay tiers for metformin and insulin while applying high cost-sharing for SGLT2 inhibitors and GLP-1 receptor agonists in type 2 diabetes care, even for patients with comorbid heart failure where newer agents show superior outcomes. This pricing architecture sustains reliance on older medications despite real-world data from the Cleveland Clinic showing faster HbA1c reduction and lower hospitalization rates with newer agents among high-risk subgroups. The underappreciated effect is that insurers indirectly subsidize metabolic instability by preserving outdated therapeutic norms under the guise of tiered cost efficiency.
Reimbursement-encoded innovation lag
In Massachusetts, Tufts Health Plan’s prior authorization requirements for certolizumab pegol in rheumatoid arthritis demand documented failure on at least three TNF-alpha inhibitors before approval, a policy that extends disease activity duration despite research consistently showing differential efficacy across biologics due to unique pharmacokinetics and immune evasion mechanisms. This creates a systematic delay in matching the right biologic to the right patient, as seen in Brigham and Women’s Hospital rheumatology follow-up data where delayed access correlated with higher progression scores on musculoskeletal ultrasound. The structural insight is that reimbursement design, not clinical complexity, becomes the rate-limiting step in therapeutic optimization.
Coverage Friction
Insurers steer patients toward older, lower-cost biologics in rheumatoid arthritis not because they are clinically inferior but because they sit at the intersection of rebate-driven formulary positioning and patent cliffs, allowing pharmacy benefit managers to extract greater rebates from manufacturers even when clinical guidelines suggest earlier use of newer agents; this creates a systemic preference for entrenched drugs despite emerging evidence of superior disease modulation with interleukin inhibitors, revealing that cost-containment logic actively resists—not responds to—therapeutic innovation, which challenges the assumption that insurance steering reflects clinical conservatism or risk aversion.
Metabolic Time Lag
In type 2 diabetes, insurers disproportionately favor metformin and GLP-1 agonists over newer dual glucose sensors paired with automated insulin delivery systems, not due to outright denial but through deliberate reimbursement delays and coverage fragmentation across multiple prior authorization gatekeepers—endocrinologists, primary care providers, durable medical equipment suppliers—thereby embedding inertia into treatment escalation pathways; this administrative friction obscures a deeper structural misalignment between clinical trajectory and payment cycles, where reimbursement systems fail to recognize that metabolic control is time-sensitive, not cost-cumulative, challenging the view that access barriers are merely financial rather than temporally engineered.
Trial-Real Dissonance
Evidence indicates newer, targeted oral therapies for rheumatoid arthritis show superior real-world adherence and reduced joint erosion compared to TNF inhibitors—now the default insurer-preferred class—yet insurers continue to enforce step therapy protocols that require failure on older agents first, not because of safety or cost alone but because regulatory trial design legitimizes short-term efficacy over long-term disability prevention, privileging statistical significance in twelve-week trials over functional outcomes at five years; this exposes a hidden epistemic hierarchy in which FDA-recognized endpoints dominate coverage policy even when real-world data contradicts their relevance, challenging the belief that insurers respond to 'evidence-based' medicine when they are in fact responding to trial-structured evidence.
Formulary Pathways
Insurers direct patients toward older, generic DMARDs like methotrexate for rheumatoid arthritis due to tiered formulary designs that minimize patient cost-sharing for these agents, reserving higher out-of-pocket burdens for biologics such as adalimumab. Pharmacy benefit managers structure these pathways through non-medical switching policies and prior authorization requirements that actively deter uptake of newer therapies, even when clinically indicated, creating a systemic preference for longitudinal use of entrenched treatments. This mechanism is underappreciated because public discourse equates insurance coverage with access, while in practice access is channeled through economically optimized treatment sequences that prioritize budgetary control over therapeutic novelty.
Metabolic Gatekeeping
Insurers steer diabetes patients toward metformin and insulin analogs with proven reimbursement histories, not because they outperform newer GLP-1 agonists in all cases, but because these agents occupy protected tiers in employer-sponsored plans administered by national carriers like UnitedHealthcare and Kaiser Permanente. The gatekeeping function operates through step therapy protocols that require documented failure on legacy drugs before covering alternatives like semaglutide, a process that delays effective treatment even when weight comorbidities or cardiovascular risk profiles favor newer options. The persistence of this model surprises many because the dominant cultural narrative treats diabetes management as a personal responsibility issue, obscuring how payer policies mechanically restrict which medical advancements become practically available.
Clinical Backfilling
When insurers limit coverage for high-cost biologic therapies in autoimmune conditions, rheumatologists compensate by recycling older, off-patent treatments into new clinical roles—such as using hydroxychloroquine as a primary anchor drug despite limited monotherapy efficacy—thereby backfilling gaps created by coverage denial. This adaptation occurs not through formal guideline changes but via practice-level workarounds in high-volume clinics in states like Ohio and California, where providers align treatment plans with available coding and billing pathways to avoid care delays. The concept is rarely acknowledged publicly because it contradicts the expectation that treatment evolution follows scientific progress, when in fact it often follows the path of least resistance in claims processing.
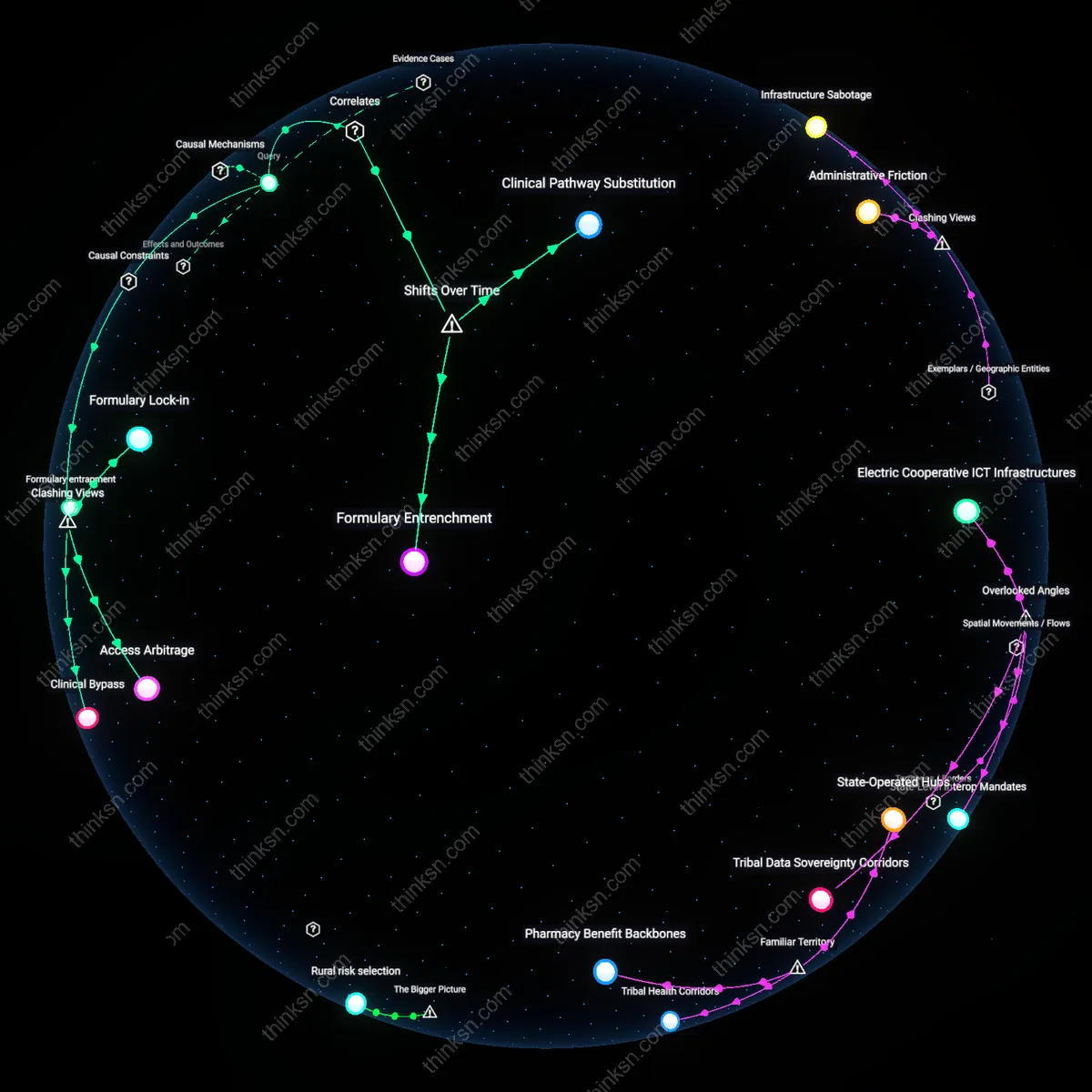
Formulary Lock-in
In the United States, insurers have systematically steered rheumatoid arthritis patients toward older TNF inhibitors like Humira and Enbrel over newer IL-6 or JAK inhibitors since the mid-2010s by placing the latter on high-tier copay structures or requiring step therapy. This shift away from unrestricted biologic access emerged as pharmacy benefit managers like Express Scripts and OptumRx consolidated formulary control, using rebate-driven contracts with manufacturers that privileged drugs with established market presence despite growing evidence of comparable or superior efficacy in newer agents. The mechanism—prior authorization mandates and tiered cost sharing—entrenches older therapies not due to superior outcomes but because of rebate-dependent profit models, revealing how post-2010 commercial insurance design prioritized financial alignment with drug makers over timely adoption of clinical innovation.
Biologic Delay Cascade
In the UK’s NHS, the transition from early methotrexate-based treatment to routine first-line biologic use for rheumatoid arthritis stalled after 2012 due to NICE cost-effectiveness thresholds that favored prolonged synthetic DMARD trials before approving TNF inhibitors, creating a treatment delay cascade that persisted even as global guidelines shifted toward early biologic use. This policy shift—driven by fiscal constraints following austerity measures—meant patients in regions like Greater Manchester experienced median delays of 18 months to biologic initiation, resulting in higher joint damage progression compared to European counterparts in Germany or Sweden where earlier access was standard. The residual effect is a structural inertia in public systems where budget caps produce therapeutic lag, revealing that post-2010 value assessment frameworks often prioritize short-term savings over long-term disability prevention.