Quality Signaling Spiral
Hospitals would artificially inflate quality metric performance to secure top-tier placement, triggering a self-reinforcing cycle of metric gaming that distorts actual care improvements. Insurers, bound by regulation to use these metrics, would amplify the signal despite its decoupling from patient outcomes, privileging institutions skilled in data presentation over those delivering equitable care. This dynamic would replicate existing access disparities under a more legitimate façade, exposing how transparency mandates can harden informational asymmetries when metrics become high-stakes currency rather than diagnostic tools. The non-obvious consequence is not greater accountability but the systemic overproduction of audit-ready quality data at the expense of unmeasured but essential aspects of care.
Network Cartel Reconfiguration
Insurers would collude around narrow interpretations of quality metrics to collectively down-classify high-cost safety-net hospitals, effectively blackballing them from top tiers despite strong community health outcomes. By anchoring tiering to technically compliant but clinically narrow benchmarks—like readmission rates or HCAHPS scores—payers would exploit regulatory ambiguity to maintain cost control under the guise of quality enforcement. This shift would preserve insurer pricing power by reframing network exclusion as objective quality management, revealing how regulatory mandates for transparency can be co-opted to legitimize exclusionary practices when enforcement lacks equity safeguards.
Access Arbitrage
Patients would face increased geographic and socioeconomic barriers as tiered networks concentrate top-tier status in affluent urban centers with robust data infrastructure, leaving rural and under-resourced hospitals systematically downgraded regardless of care quality. Insurers would leverage the new tiering framework to steer enrollees toward consolidated health systems capable of meeting metric thresholds, effectively transferring access decisions from price negotiation to structural data capacity. This realignment would deepen fragmentation in care access not through overt rationing but through the uneven distribution of administrative capability, uncovering how metric-based equity can exacerbate spatial inequalities when infrastructure is unevenly distributed.
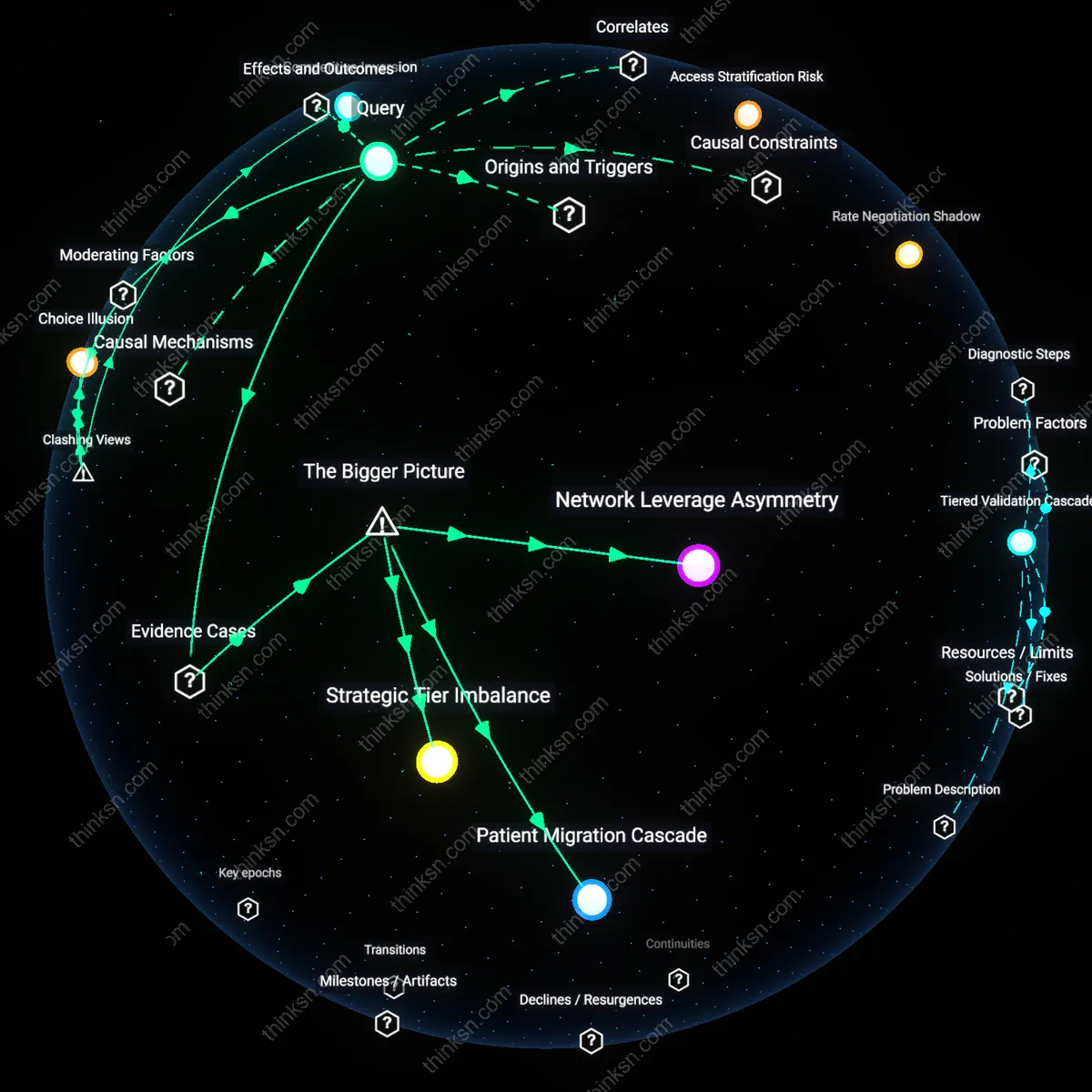
Tiered Validation Cascade
Hospital pricing would align with clinical outcomes data because tier placement would depend on audited performance metrics like readmission rates and infection scores. Insurers, such as UnitedHealthcare or Aetna, would rely on CMS-collected data or third-party certifications to assign hospitals to tiers, shifting leverage from billing departments to quality improvement units within hospitals; this reorients financial incentives around sustained care excellence rather than payer-side negotiation power. The underappreciated shift is that hospitals currently compete on rate discounts, not care consistency—making quality a pricing determinant forces operational transparency even in markets with little payer competition.
Access Stratification Risk
Patient access would concentrate in high-tier urban academic centers because quality metrics favor institutions with specialized reporting infrastructure and lower patient complexity. Safety-net hospitals and rural providers, often penalized by risk-adjustment gaps and underresourced data systems, would fall to lower tiers despite serving vulnerable populations. The intuitive link between 'quality' and 'better care' obscures how standardized metrics can replicate inequities—patients in underserved areas may face narrower networks under the guise of quality assurance, effectively limiting mobility under a technically rational framework.
Rate Negotiation Shadow
Insurers would embed hidden price adjustments through tier design loopholes, such as manipulating the threshold for 'high quality' or controlling appeal processes for tier placement. Even with transparent metrics, carriers like Cigna or Blue Cross Blue Shield could delay data incorporation or weight less disadvantageous indicators, preserving negotiated pricing influence within a seemingly objective structure. The non-obvious reality is that transparency in criteria does not eliminate discretionary control—regulatory compliance can be met formally while preserving the substantive power to shape network costs behind administrative gates.
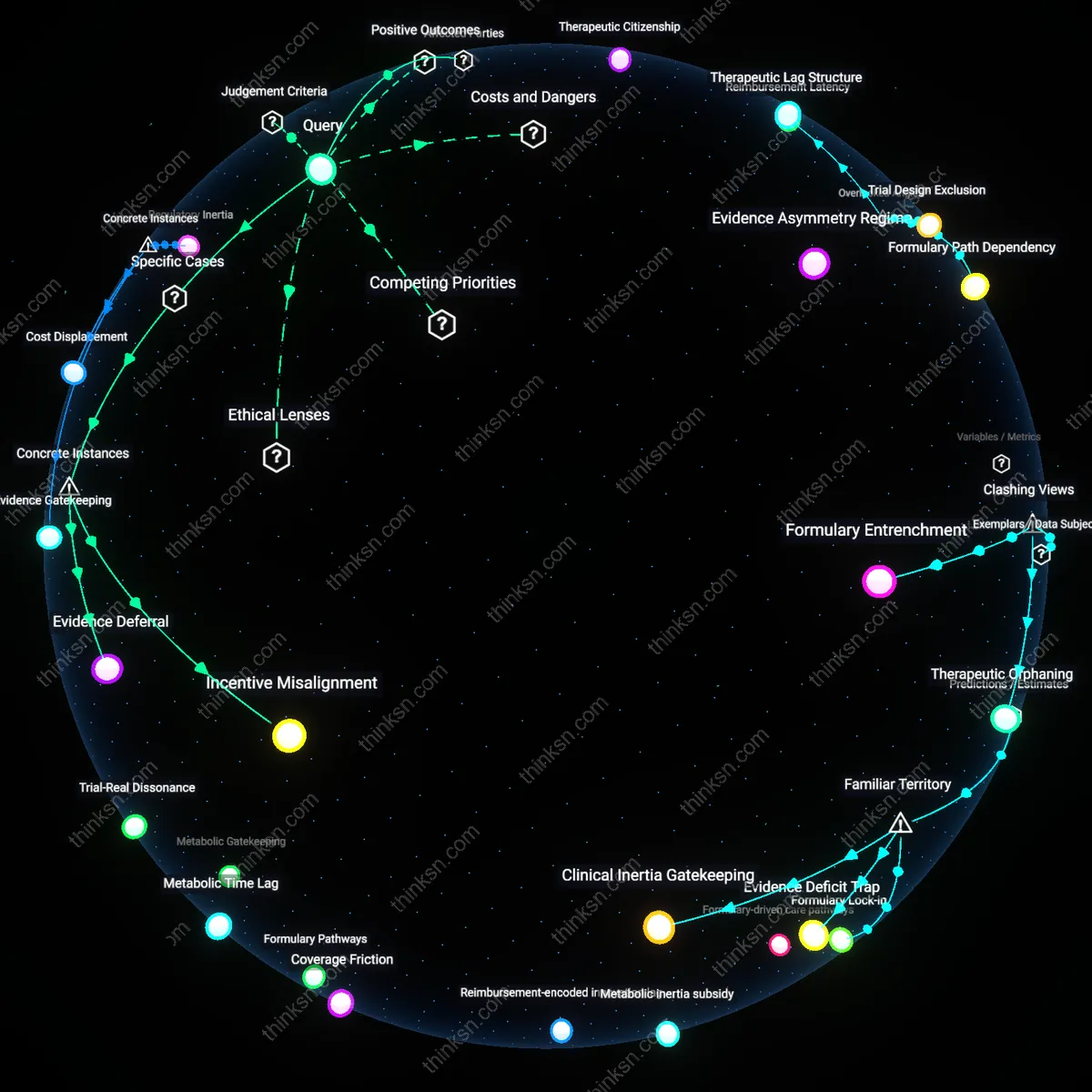
Tiered Yield Compression
Payers would reconfigure hospital tiering to prioritize facilities with historically high procedure volume over those with favorable negotiated rates, because transparent quality metrics would favor institutions with lower readmission rates and complication counts, which correlate strongly with experience rather than cost efficiency. As a result, high-volume academic medical centers in urban corridors like Boston and New York would consolidate tier-1 positioning, narrowing patient access to these centers while eroding insurer leverage to extract rate concessions, a shift that surfaced clearly after the 2015 Medicare Value-Based Purchasing rollout revealed how quality metrics systematically advantaged incumbents with reporting capacity. The non-obvious consequence is not improved care but a structural bias in favor of institutions already embedded in outcome-reporting infrastructure, which enables them to 'quality-wash' higher prices.
Metric Arbitrage Regimes
Hospitals in suburban and rural markets would invest in metric-optimized care pathways focused narrowly on the indicators that determine tier status—such as 30-day pneumonia readmissions or SCIP compliance—rather than broad improvements in patient outcomes, because the regulatory regime would incentivize technical adherence to reportable metrics over holistic care. This phenomenon intensified during the shift from volume- to value-based reimbursement post-2010, when public reporting revealed that selective metric performance could be gamed without altering underlying clinical capacity, producing a new form of regulatory compliance that mimicked quality without requiring it. The underappreciated dynamic is that transparency in quality metrics does not eliminate gaming—it redirects organizational effort toward visibility, creating a class of 'metric-fit' institutions that thrive under audit without transforming care delivery.
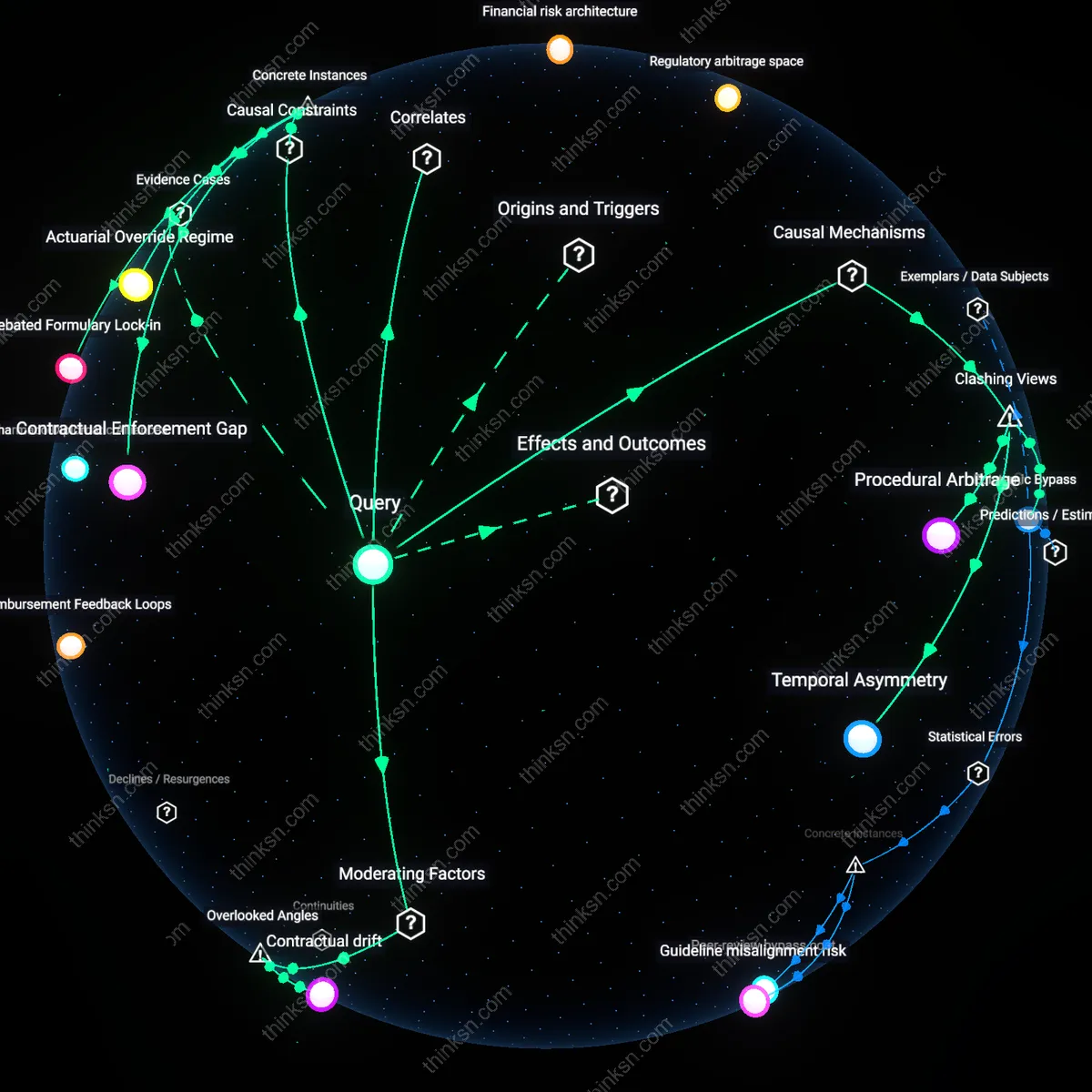
Negotiation Shadow Market
Insurers would resurrect de facto rate-based tiering by embedding price adjustments within quality improvement agreements, shifting rebates and bonuses off public rate schedules and into private contracts contingent on unreported benchmarks, because historically, transparency mandates like those in the 2007–2012 state all-payer claims databases triggered parallel systems of undisclosed risk-sharing to preserve negotiating flexibility. As occurred with Medicare Advantage plan networks post-2010, when quality star ratings drove access decisions, the formal rejection of price as a tiering factor would amplify informal pricing mechanisms in the interstices of oversight, revealing a persistent regulatory duality. The overlooked insight is that when public criteria constrain visible levers, market actors innovate behind the scenes—preserving economic hierarchies under a façade of quality equity.
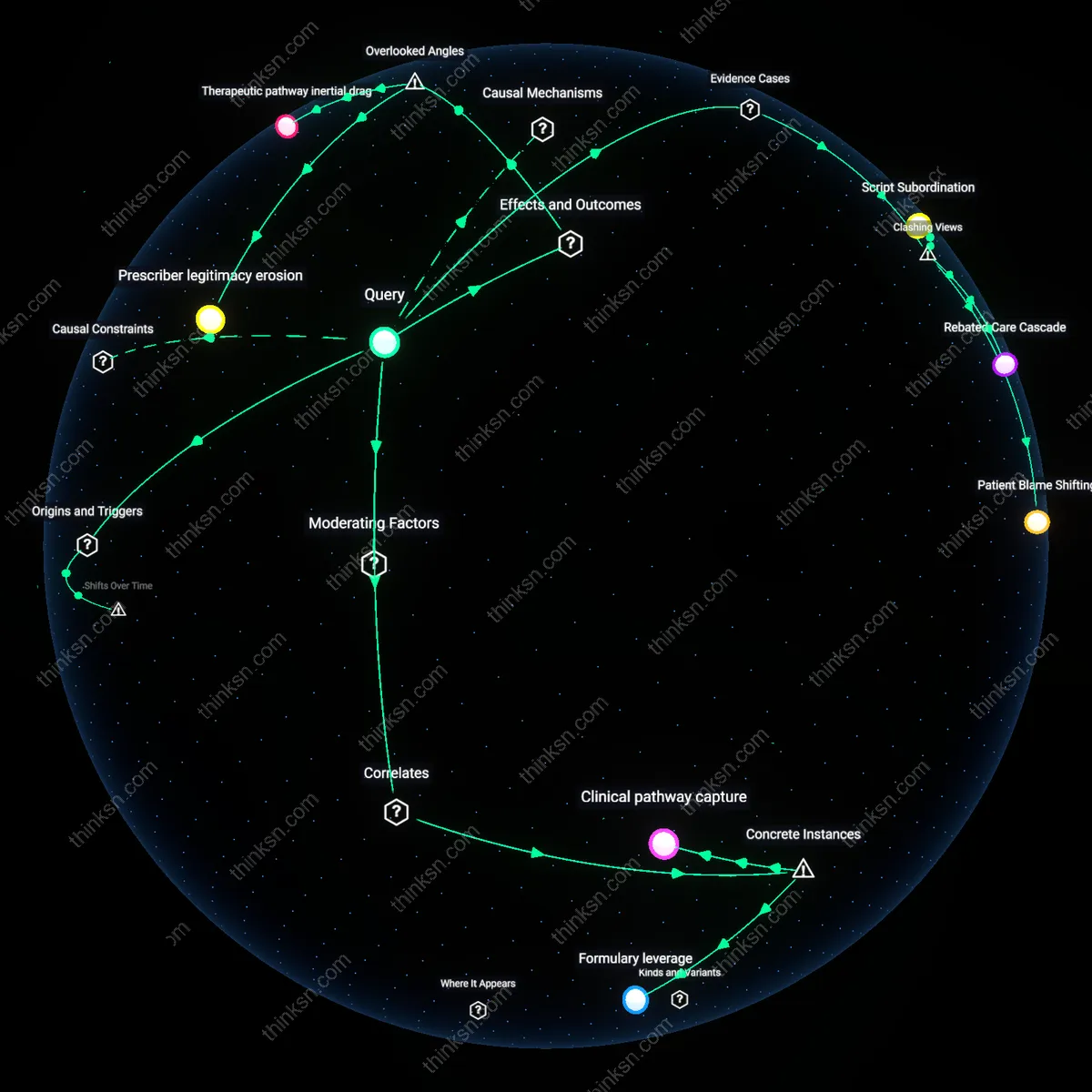
Referral pathway inertia
Doctors would route patients to high-tier hospitals even when clinically unnecessary, because transparent quality metrics rarely capture appropriateness of care, shifting costs without improving outcomes. This happens because physician referral patterns are shaped more by habit, malpractice risk, and patient expectations than by real-time quality data, especially for low-acuity conditions—so even if networks tier hospitals based on mortality or readmission rates, clinicians may still default to familiar academic centers. This undermines the policy’s goal of cost containment and reveals that referral decision-making is governed less by quality transparency and more by latent institutional trust and defensive practice norms—a dynamic absent in most regulatory impact models.
Infrastructure justification trap
Hospitals in rural or underserved areas would lose tier status not due to poor clinical performance but because their patient populations generate outlier data on risk-adjusted metrics, reinforcing geographic disparities in access. This occurs because quality metrics like 30-day readmissions are calculated using models trained on urban, insured populations, so safety-net and rural hospitals face statistical penalties for factors beyond their control—transportation deserts, housing instability, or fragmented follow-up. As a result, these institutions get downgraded to lower tiers or excluded, reducing reimbursement and making reinvestment in quality improvements impossible, thereby cementing a self-fulfilling decline that most policy discussions ignore by assuming metric neutrality.
Data governance asymmetry
Insurers would gain disproportionate influence over which quality data streams count as valid, allowing them to shape tiers through technical standards rather than negotiation, ultimately preserving pricing power. This arises because establishing transparent metrics requires centralized validation, auditing, and certification of data—functions that would likely be delegated to private health information organizations or payer-backed entities, not public agencies. Thus, even without direct rate bargaining, insurers could exclude real-world outcomes like patient-reported experience or long-term functional recovery if they can’t integrate them into claims-based systems, making 'transparency' a gatekept construct rather than a democratized tool—something most reform proposals overlook when treating data as a neutral input.
Tiered Network Realignment
Requiring tiered networks to base tiers on transparent quality metrics would shift hospital pricing power toward institutions with independently verified outcomes, because payers would lose discretion to prioritize cost-cutting over clinical performance, and providers would compete on publicly visible value rather than behind-closed-doors rebate deals. This reorients network design around longitudinal patient outcomes tracked via federal or accredited registries, disrupting the current system where high-priced hospitals retain top-tier status through contractual exclusivity rather than efficacy. The non-obvious consequence is that regional medical centers with strong safety records but limited bargaining power could displace elite academic hospitals in network tiers, altering care access patterns in Medicare and commercial markets.
Regulatory Signal Distortion
Mandating quality-metric-based tiering would create perverse incentives for hospitals to optimize for measured indicators at the expense of unmeasured but clinically significant outcomes, as tier status directly affects patient volume and insurer reimbursement rates. Because quality metrics are inevitably incomplete—favoring process measures like readmission rates over complex care coordination—this policy could amplify gaming behaviors similar to those seen under value-based payment models in the Medicare Access and CHIP Reauthorization Act (MACRA). The broader systemic risk is that regulatory transparency, intended to empower patients, instead distorts clinical priorities through misaligned performance signals, privileging measurable over meaningful care.