Are Mental Health Apps Making Self-Care Unequal?
Analysis reveals 9 key thematic connections.
Key Findings
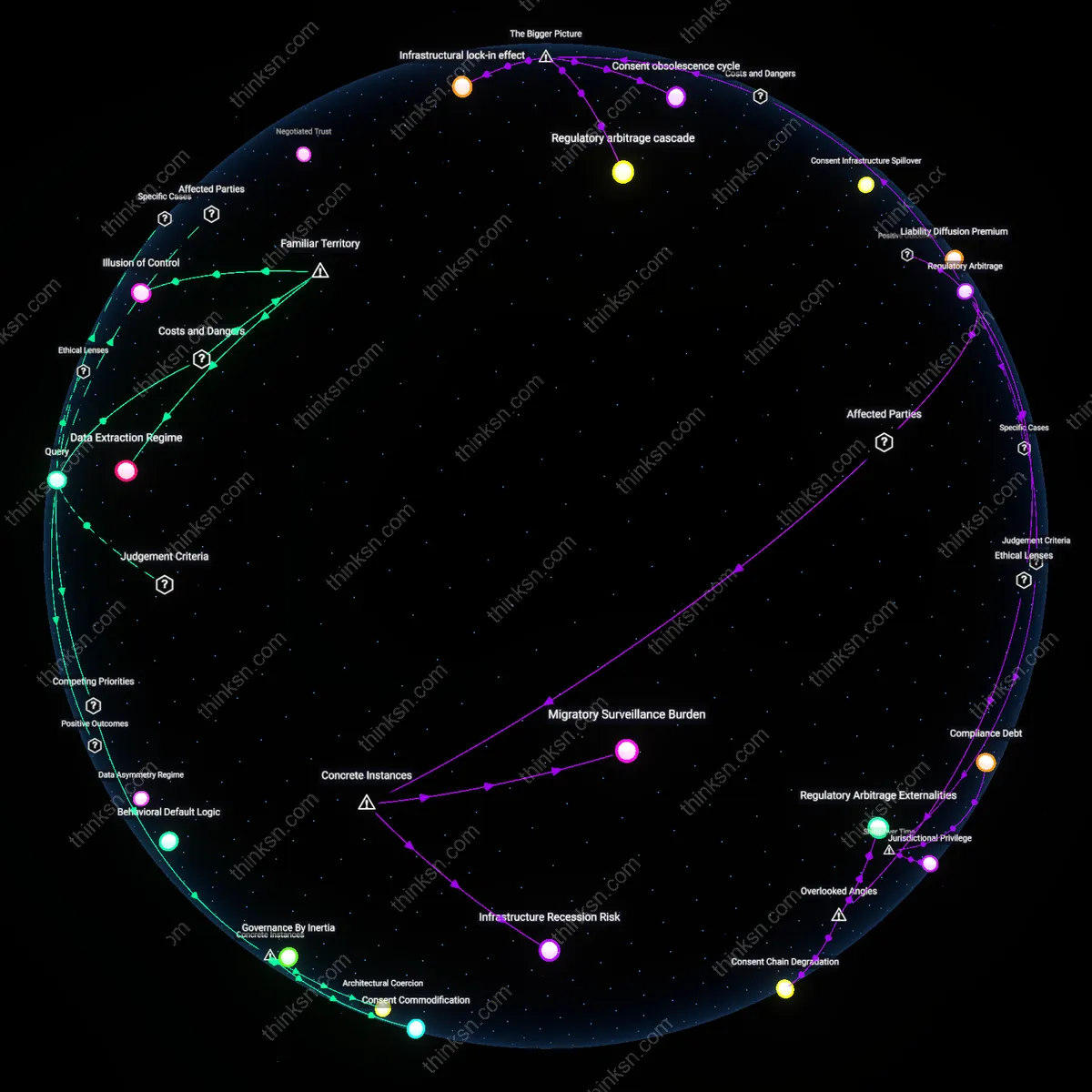
Marketized Care
The 2015 launch of Talkspace, backed by Silicon Valley capital and marketed through corporate wellness partnerships, shifted mental health access toward subscription-based digital platforms, positioning therapy as a productivity tool rather than a medical good; this reframing caters to salaried workers with employer-covered subscriptions while excluding gig workers and the uninsured, thereby institutionalizing a tiered system of psychological care. The non-obvious consequence is not just unequal access but the redefinition of mental health itself into a commodified, performance-enhancing service available only to those whose labor is formally recognized and compensated.
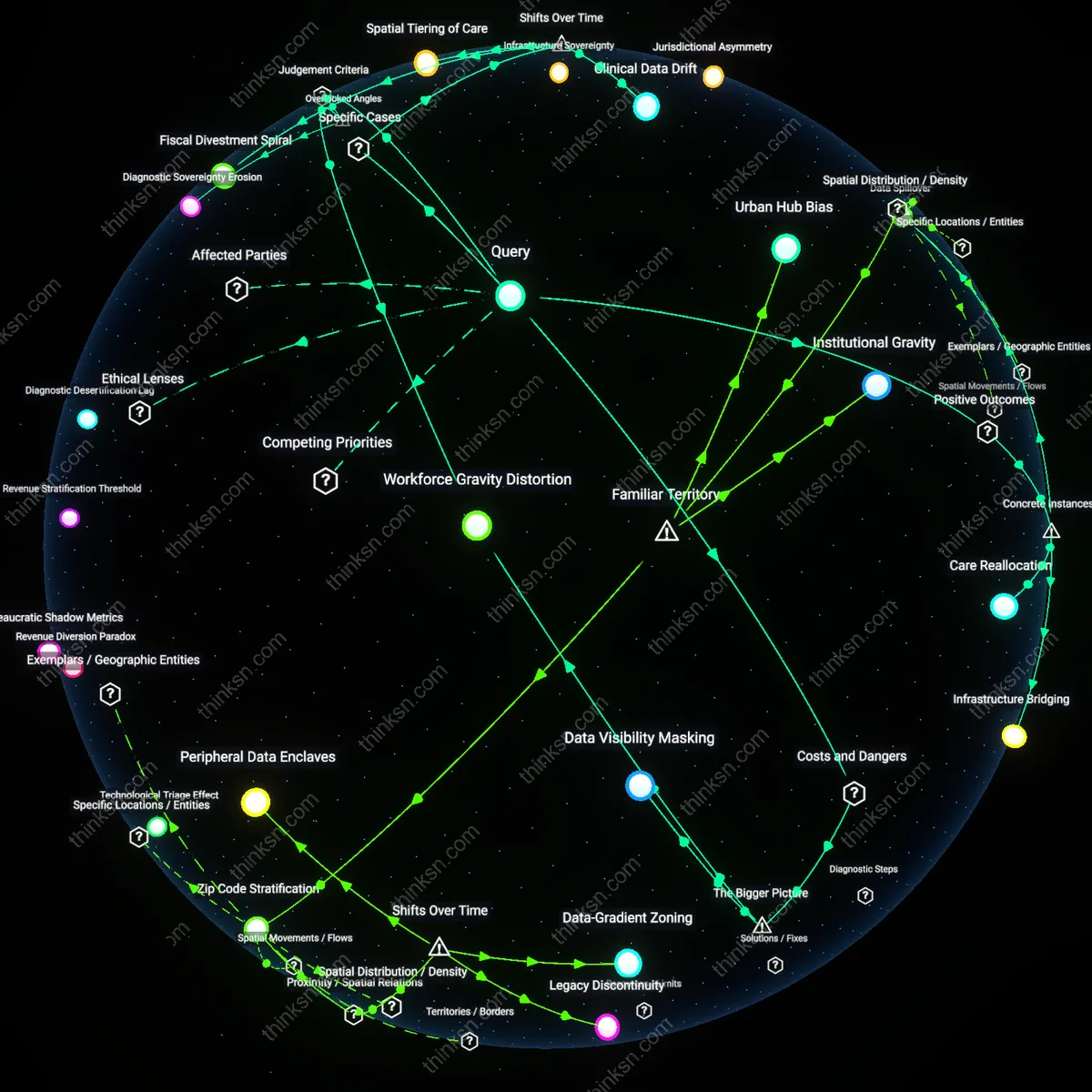
Data Stratification
In 2020, India’s National Tele-Mental Health Programme was scaled amid the pandemic, prioritizing smartphone app integration over localized, multilingual outreach, which led to overrepresentation of urban, English-speaking users in national mental health databases while rural populations remained invisible despite higher distress indicators. This technical bias reinforces structural neglect by rendering marginalized groups statistically absent in policy decisions, revealing how digital infrastructure can deepen exclusion through the illusion of universal reach.
Therapeutic Individualism
Following the 2017 opioid crisis peak in West Virginia, mental health apps like myStrength were introduced as low-cost behavioral supplements in lieu of expanding Federally Qualified Health Centers, shifting responsibility onto individuals to self-manage trauma and addiction through algorithmic prompts instead of guaranteed treatment access; this offloads public health obligations onto personal discipline, normalizing austerity through the rhetoric of empowerment. The hidden mechanism is the substitution of systemic investment with app-mediated coping, masking systemic abandonment as self-care.
Digital Pareto Fix
The rise of mental-health apps entrenches a cost-shifting logic in public health by enabling governments and insurers to outsource care to low-cost digital tools while maintaining coverage mandates. This substitution disproportionately affects low-income users, who face structural barriers like spotty internet, outdated devices, and competing survival demands that limit app engagement—turning a purported solution into a tiered system where the affluent receive human-led care and the poor are funneled into under-resourced digital alternatives. The mechanism operates through fiscal austerity policies and public-sector contracting incentives that reward 'innovation' over equity, making this shift appear progressive while deepening care deserts. What’s underappreciated is how these apps become alibis for disinvestment, allowing institutions to claim responsiveness without expanding access, thereby naturalizing inequality under the guise of technological democratization.
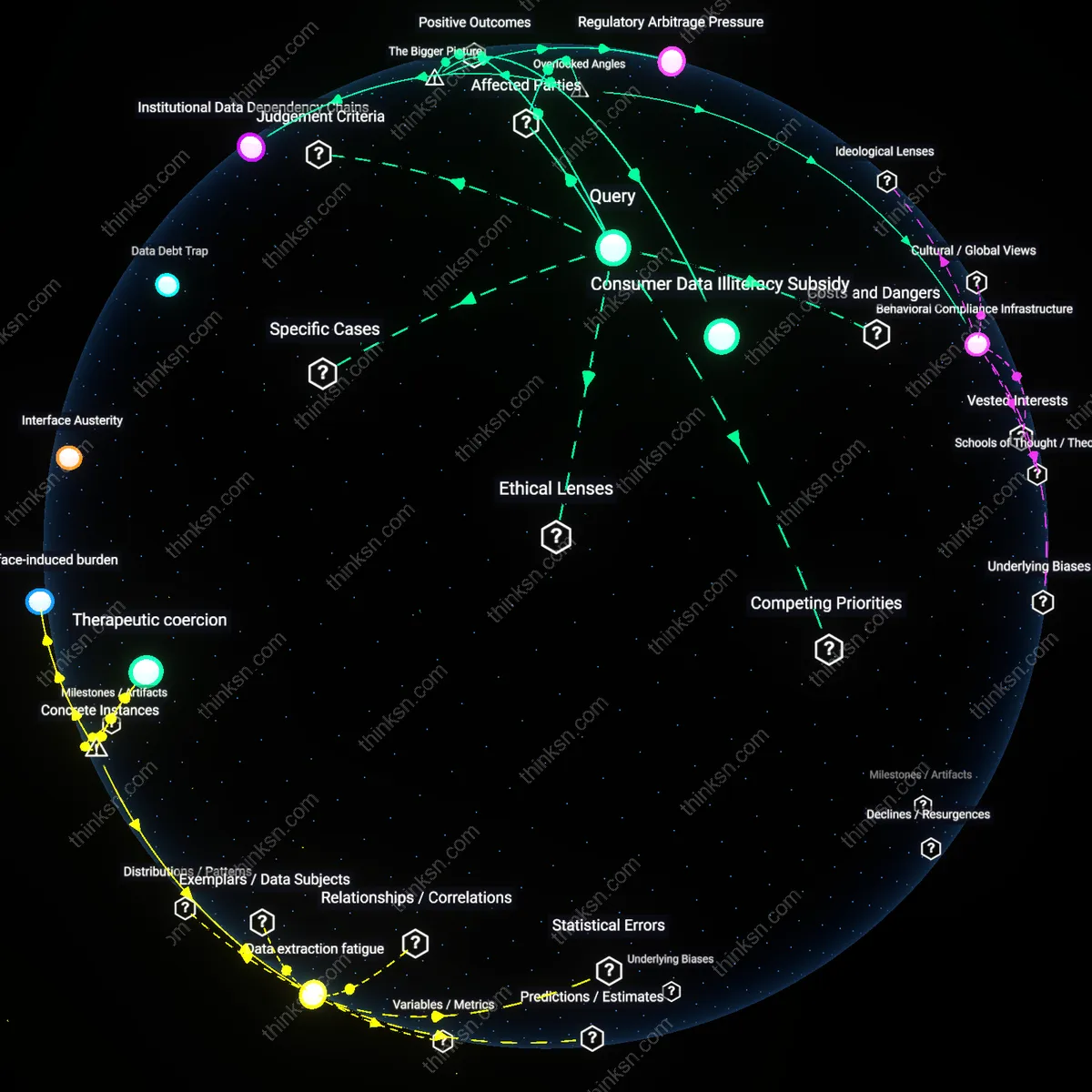
Therapeutic Data Imperative
Mental-health apps amplify societal demands for self-management by redefining psychological well-being as a matter of personal data tracking and behavioral optimization, driven by Silicon Valley’s fusion of clinical language and productivity culture. This reframing pressures users—especially those in precarious employment or welfare systems—to continuously monitor moods, log triggers, and demonstrate self-improvement, often to qualify for benefits or workplace accommodations, thus turning introspection into a performative duty. The system functions through algorithmic feedback loops and gamified UX design that reward compliance, making emotional regulation a metricized skill rather than a socially embedded experience. The non-obvious consequence is that this datafication pathologizes structural distress—like poverty or isolation—by recasting them as individual data gaps, obscuring collective remedies behind a veneer of self-driven progress.
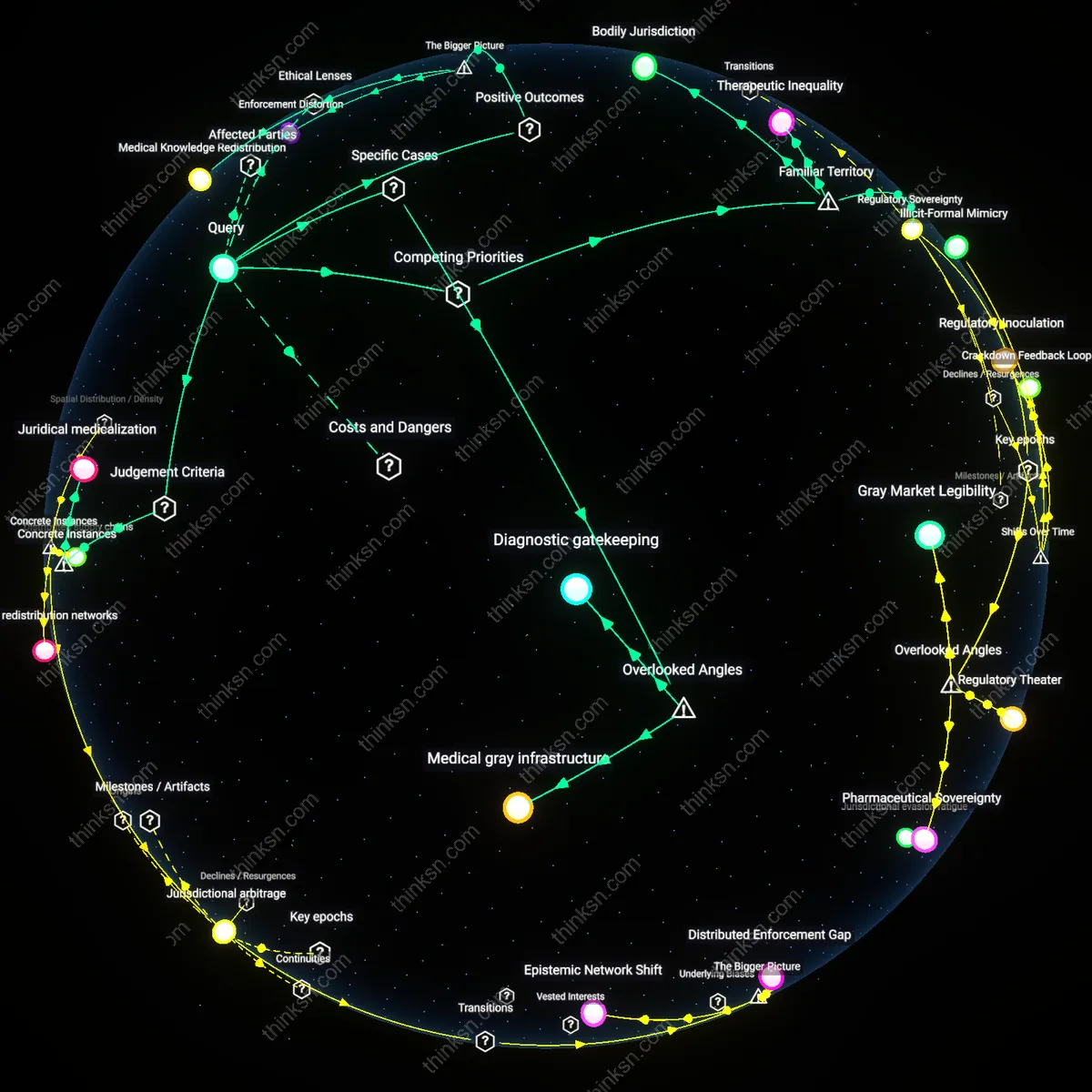
Clinical Attention Gradient
The proliferation of mental-health apps reshapes professional care hierarchies by redirecting clinician time and institutional resources toward supervising and integrating app-generated patient data, privileging patients who can afford devices, understand digital interfaces, and engage consistently—typically higher-income users. This creates a clinical feedback loop where therapists spend disproportionate time interpreting app outputs for compliant users, while those unable to participate digitally are labeled 'non-adherent' and deprioritized, accelerating their exit from care networks. The dynamic is sustained by value-based healthcare models that incentivize outcomes tied to measurable engagement, reinforcing an attention economy in which visibility in digital systems determines access to human care. The overlooked effect is that technology doesn’t merely supplement treatment—it actively filters who counts as a 'treatable' subject within modern mental health systems.
Therapeutic Burden Shift
The rise of mental-health apps since 2010 has transferred responsibility for clinical monitoring from institutional healthcare providers to individual users, particularly visible in Medicaid expansion states like Oregon where public insurers began covering app-based interventions such as Talkspace by 2018. This shift replaced scarce in-person therapy slots with self-directed app usage, leveraging digital tools to manage growing patient loads amid flat public health funding—revealing a post-2008 policy turn where austerity-driven efficiency measures reframed access to care as personal accountability. The non-obvious consequence is that low-income users, while gaining nominal access, now bear the cognitive and emotional labor of navigating complex diagnostic and scheduling features without digital literacy or reliable internet—turning affordability into a new form of exclusion.
Datafied Self-Care Regime
Starting around 2015, Silicon Valley–backed apps like Headspace and Calm redefined mental wellness as a trackable, behaviorally optimized routine, coinciding with corporate adoption of these platforms in employee wellness programs at firms like General Mills and Aetna. As workplace mental health shifted from occupational hazard mitigation to individual resilience training, self-management became measured through app-logged meditation minutes and sleep scores—transforming mental health into quantified performance metrics. This historical pivot obscured structural sources of distress, such as precarious work or housing instability, and rendered low-income workers—especially in gig sectors like Uber and DoorDash—more vulnerable, since exclusion from these data-driven regimes denied them both therapeutic benefits and the reputational capital of being a 'measurable' self-manager.
Digital Triage Infrastructure
From 2020 onward, during the pandemic-driven telehealth surge, federally qualified health centers in cities like Chicago and Oakland began deploying mental-health apps such as Sanvello as front-end screening tools to prioritize in-person care. This marked a distinct shift from apps as voluntary supplements to mandatory gatekeepers within safety-net systems, where limited clinician capacity forced reliance on algorithmic risk scoring to allocate scarce resources. The underappreciated effect is that patients without smartphones or stable data plans—disproportionately low-income Black and Latino populations in public housing—were automatically deprioritized, not due to clinical need but infrastructural exclusion, revealing how crisis-driven digitization hardened existing inequities into technical protocols.