Is Upgrading Disability Insurance Worth Risk of Denial?
Analysis reveals 9 key thematic connections.
Key Findings
Claims Adjudication Culture
The added cost of higher-coverage disability insurance is justified when the insurer’s internal claims adjudication culture systematically applies stricter interpretive standards to ambiguous medical evidence, disproportionately affecting neuroatypical or chronic-pain claimants. This mechanism operates through regional claims processing centers where unwritten norms—such as favoring objective biomarkers over patient-reported outcomes—develop independently of corporate policy, leading to higher denial rates for conditions like fibromyalgia or long COVID, even when coverage appears inclusive. Most risk models use aggregate denial statistics without accounting for these procedural microclimates, which means actuarially sound policies can still expose vulnerable enrollees to de facto exclusion, altering the value proposition of higher coverage for precisely those who need it most.
Provider Documentation Burden
Purchasing higher-coverage disability insurance is less justified when the insurer's historical data reflects denial patterns driven not by policy exclusions but by inconsistent medical documentation practices among primary care providers in under-resourced clinics. Because these providers—especially in rural or safety-net settings—face time and staffing constraints, they often fail to submit the longitudinal clinical narratives insurers later demand during claims review, resulting in technical denials despite legitimate disability. The overlooked dependency here is that coverage value depends not only on insurer behavior but on the capacity of third-party clinicians to produce bureaucratically legible records, meaning higher premiums may primarily reward patients treated in well-resourced systems rather than those with greater medical need.
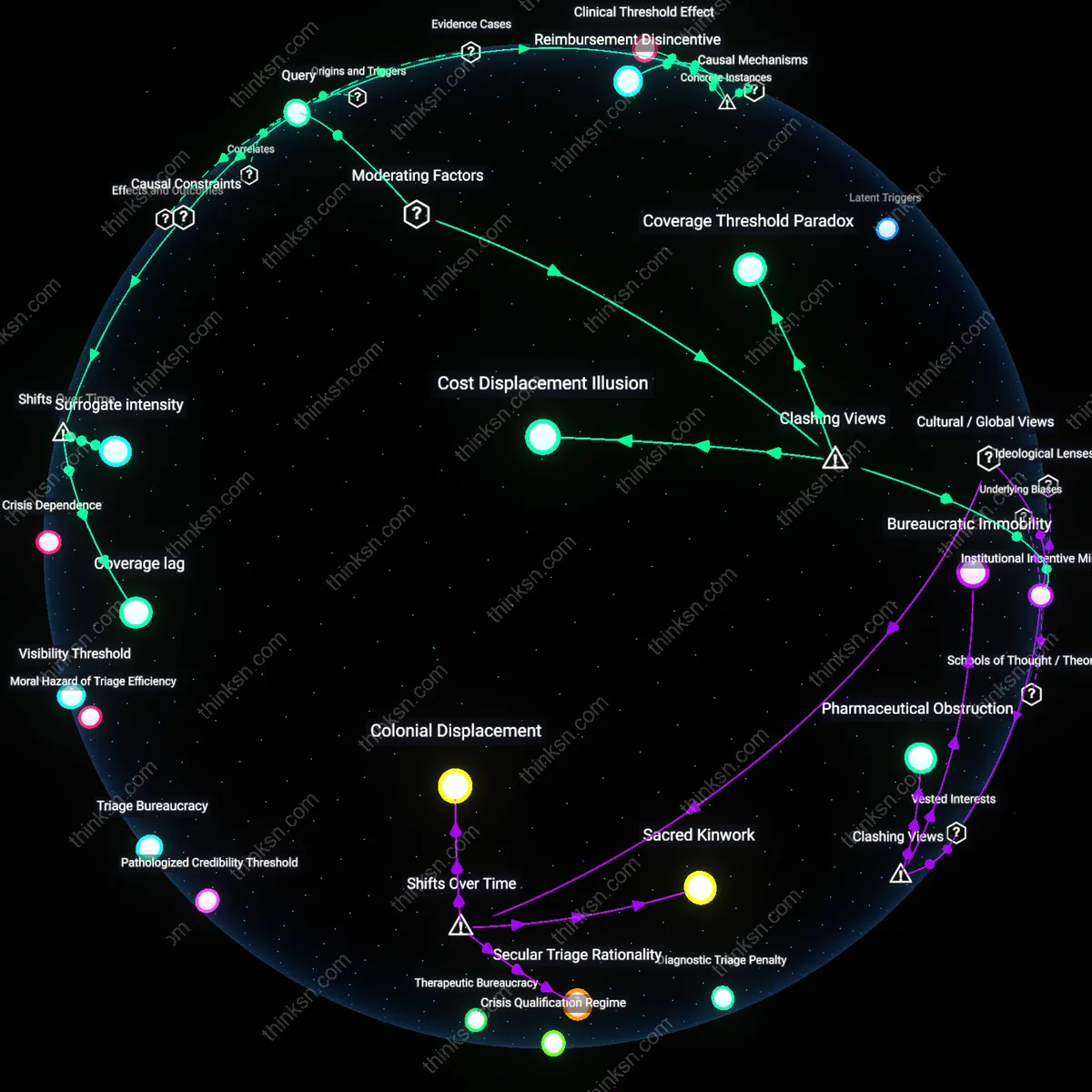
Temporal Coverage Gaps
The cost of elevated disability coverage is unjustified when historical denial data conceals a pattern of deliberate delay tactics that convert short-term disabilities into de facto long-term exclusions through procedural exhaustion. Insurers with high approval rates after two years, for example, may still dissuade claims by requiring repeated appeals and psychological evaluations that drain claimants’ financial and emotional reserves, effectively filtering out those without external support networks. This dynamic renders historical approval rates misleading because they reflect attrition rather than medical eligibility, privileging resilience over need and undermining the assumed link between coverage level and protection—especially for low-wealth applicants whose capacity to endure bureaucratic friction is lowest.
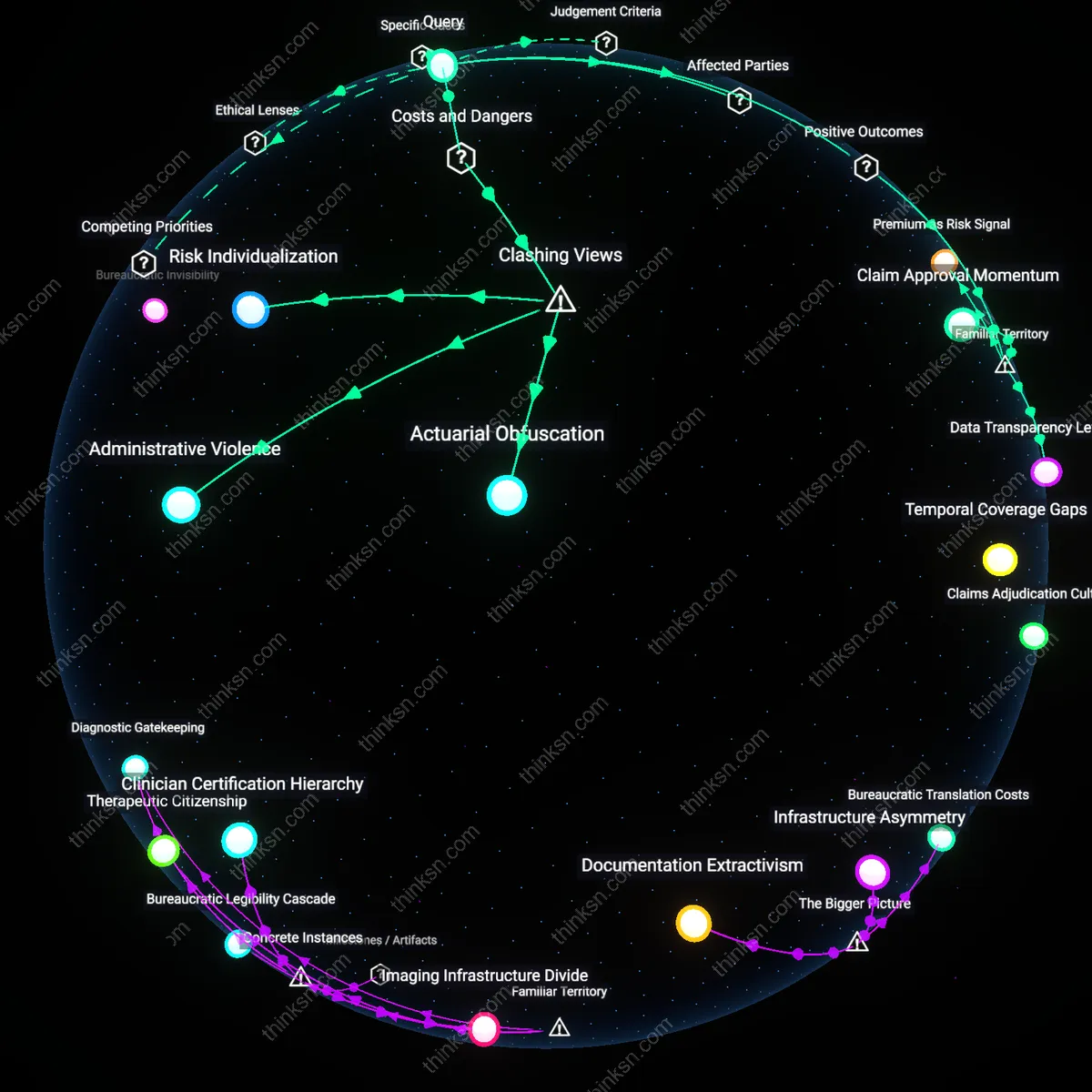
Claim Approval Momentum
Purchasing higher-coverage disability insurance is justified because insurers with historically low denial rates create a self-reinforcing pattern where claimants experience faster, more consistent approvals due to established internal protocols and precedent. This momentum reduces psychological and financial strain on policyholders during critical recovery periods, particularly among middle-income professionals in regulated sectors like healthcare or education, where return-to-work timelines are predictable and documentation is standardized. The underappreciated aspect is that claim success isn’t just about individual policy terms but about the insurer’s systemic inertia toward honoring claims once a track record is set, which most consumers overlook when focusing narrowly on premium cost.
Premium as Risk Signal
Paying more for higher-coverage disability insurance is justified because the premium difference serves as a market signal that aligns the policyholder with a lower-risk cohort, often automatically routed to streamlined claims processing within the same insurer. In practice, carriers like Guardian or Northwestern Mutual segment their underwriting tiers by premium class, where higher-paying customers receive preferential treatment in claim review due to perceived financial reliability and lower fraud indicators, effectively buying access to a faster, more lenient adjudication pipeline. What’s rarely acknowledged is that the added cost functions less as a coverage upgrade and more as a social sorting mechanism—elevating the policyholder into a trust-weighted category where denial becomes institutionally disfavored.
Data Transparency Leverage
The added cost of higher-coverage disability insurance is justified when the insurer publishes granular historical claim denial data, enabling employers and financial advisors to negotiate group policy terms with measurable confidence in payout reliability. For example, firms like Principal Financial disclose multi-year claims acceptance rates by occupation and diagnosis, allowing corporate HR departments to justify premium increases as risk-mitigating investments that enhance employee retention and productivity during medical leave. The overlooked insight is that public claims data doesn’t just inform individual choice—it transforms insurance into a strategic human capital tool, where coverage level becomes a lever for organizational stability rather than mere personal protection.
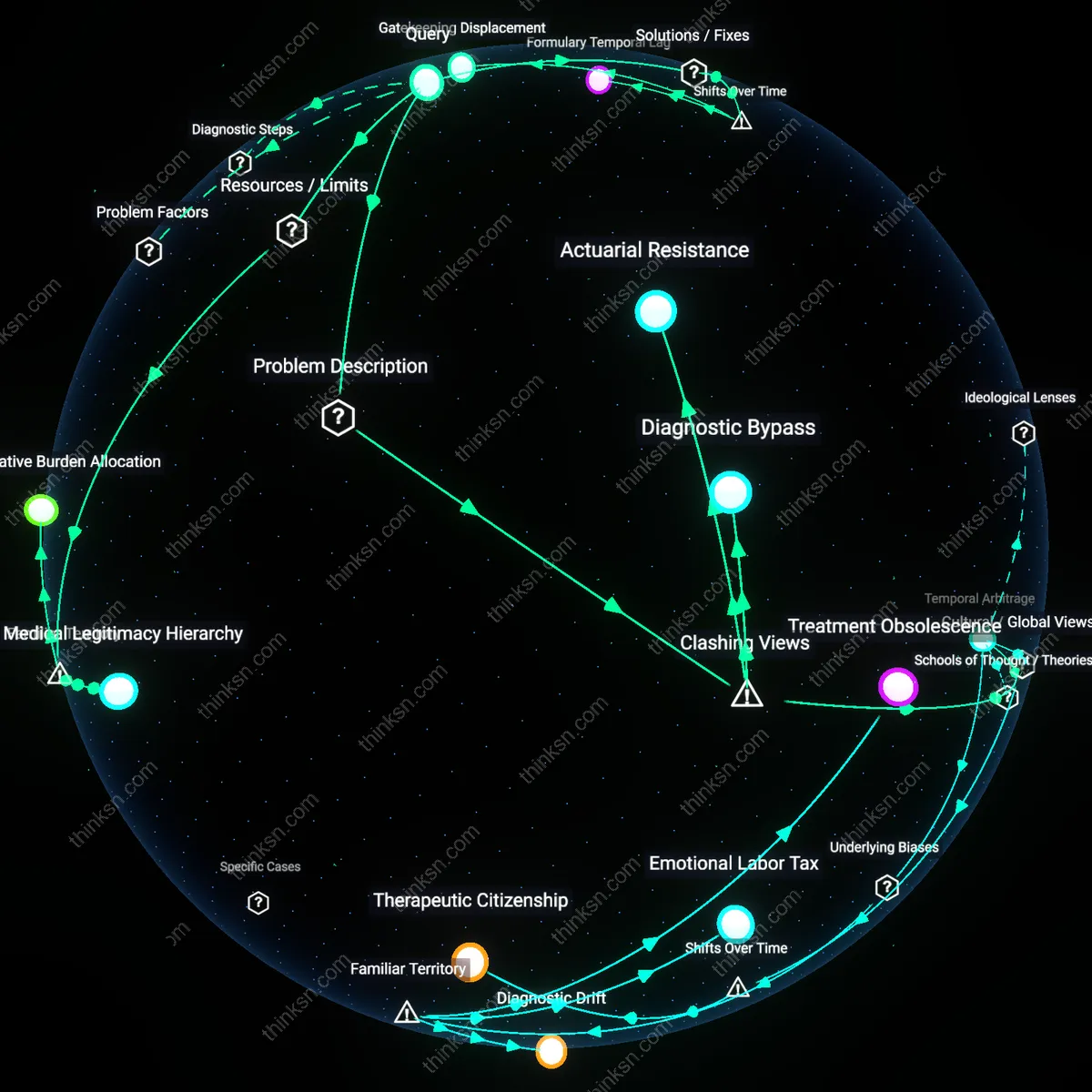
Actuarial Obfuscation
The higher cost of a higher-coverage disability insurance policy is not justified by claim denial rates because insurers systematically exploit historical data opacity to exaggerate actuarial risk, thereby inflating premiums under the guise of statistical prudence. Insurers retain control over how claim denial metrics are defined, categorized, and reported—adjusting for 'pre-existing conditions' or 'subjective symptom reporting' in ways that amplify perceived risk without transparent validation. This creates a feedback loop where policyholders pay more for coverage that appears rationally priced by historical outcomes, but those outcomes are shaped by discretionary, non-audited adjudication practices. The non-obvious reality is that denial rates are not neutral statistics but instruments of cost extraction masked as risk management.
Administrative Violence
Purchasing higher-coverage disability insurance based on historical denial rates perpetuates harm by legitimizing bureaucratic mechanisms that systematically invalidate legitimate claims through procedural complexity rather than medical merit. Insurers deploy multi-tiered review processes, demand repetitive documentation, and impose narrow diagnostic criteria—practices that increase the implicit cost of claiming, even when policies are ultimately paid out. This structural friction disproportionately impacts claimants during periods of peak vulnerability, effectively punishing illness with administrative burden. The dominant view assumes denial rates reflect clear-cut statistical risk, but the real danger lies in how 'accepted' claims are eroded through delayed, contested, and partial payouts that historical data rarely captures.
Risk Individualization
Justifying the cost of higher-coverage policies via historical denial data falsely locates risk within individual policyholders rather than within the unstable labor and healthcare systems that generate disability claims. Insurers frame denial rates as indicators of personal eligibility failure, diverting attention from macro forces—precarious work, inadequate public health infrastructure, and chronic underfunding of mental health care—that increase long-term disability incidence. This individualization of systemic failure makes it appear rational to pay more for coverage as a personal hedge, when in fact the rising cost reflects a shifting of societal risk onto private balance sheets. The underappreciated consequence is that actuarial 'rationality' becomes a tool for depoliticizing structural collapse.