Do Partial Drug Coverage Deals Benefit Patients or Insurers?
Analysis reveals 5 key thematic connections.
Key Findings
Insurer Gatekeeping
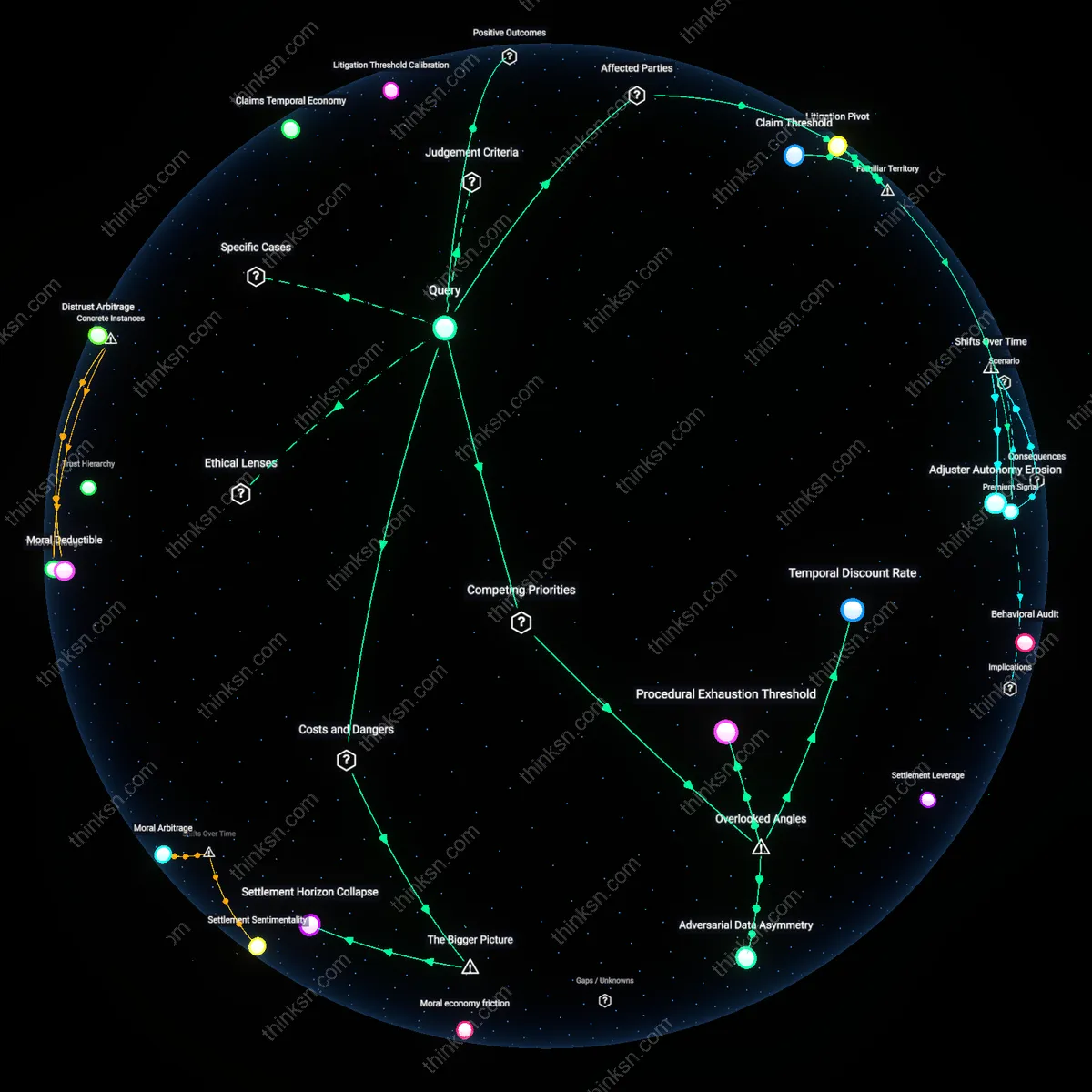
A financially stressed patient should reject partial drug coverage that cedes decision-making to insurers, as seen in prior authorization requirements under UnitedHealthcare’s 2022 Medicare Advantage plans, where algorithm-driven denials delayed lifesaving cancer treatments; this mechanism substitutes clinical judgment with administrative protocols, revealing how insurers exert hidden rationing through procedural friction rather than explicit exclusion.
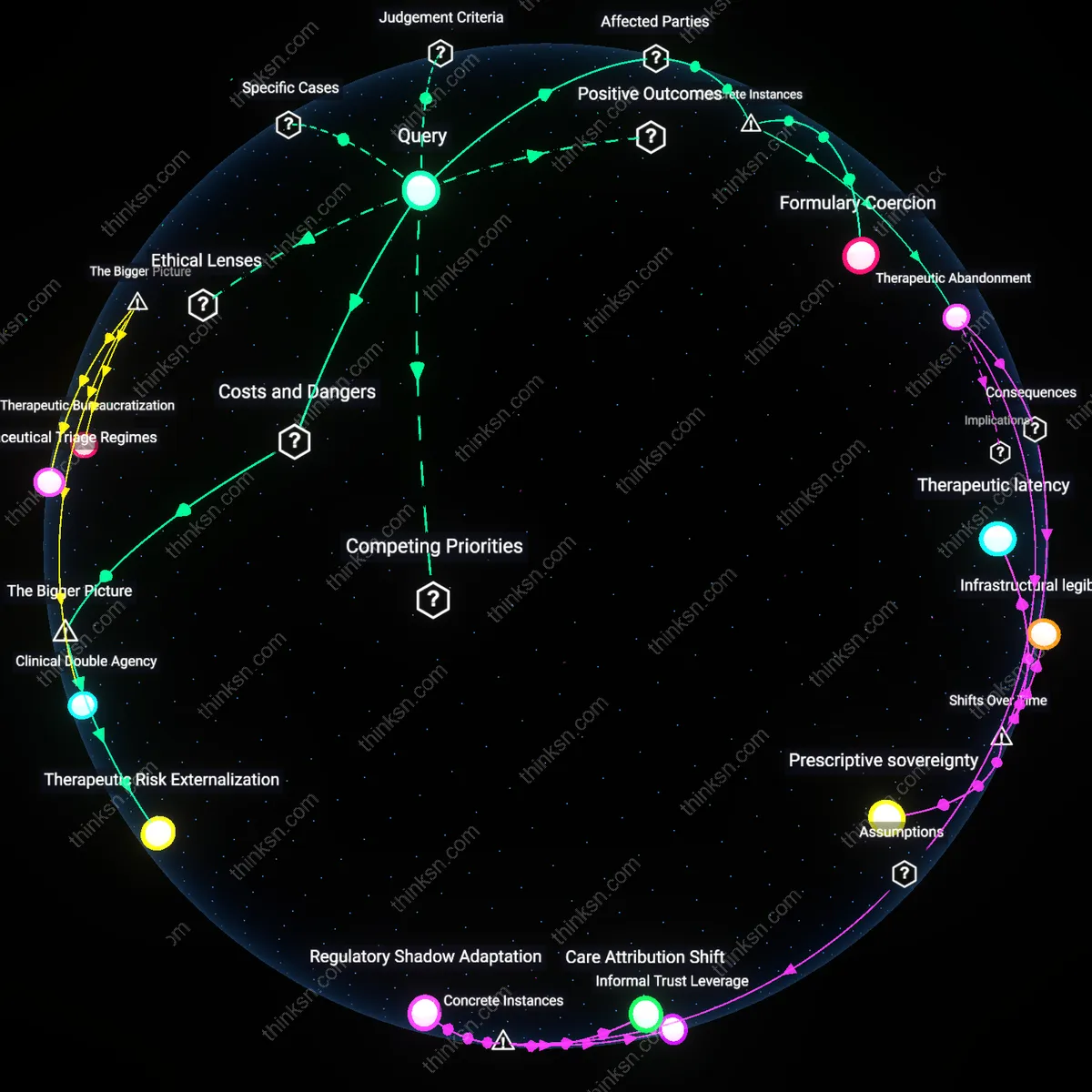
Therapeutic Abandonment
A financially stressed patient should accept partial drug coverage even with insurer control, as occurred in Tennessee’s 2018 Medicaid waiver application that restricted opioid addiction medications to insurer-approved providers, where access to any buprenorphine was better than none for rural patients facing withdrawal; this illustrates how marginalized patients endure diminished agency to avoid total therapeutic collapse, exposing a survival logic beneath apparent compliance.
Formulary Coercion
A financially stressed patient should resist partial coverage that shifts treatment authority to insurers, exemplified by the 2019 EpiPen placement on CVS Caremark’s restricted formulary, which forced schools and families to use insurer-favored generics with unproven efficacy in anaphylaxis emergencies; this dynamic reveals how formulary design exploits financial desperation to normalize untested substitutions, leveraging economic pressure to reshape medical norms.
Coverage-Conditional Authority
A financially stressed patient should reject partial drug coverage that transfers formulary control to insurers because it surrenders clinical decision sovereignty to third-party payers whose risk-pooling logic prioritizes population-level cost containment over individual therapeutic need. Insurers exercise this authority through prior authorization, step therapy, and tiered co-pays—bureaucratic frictions that delay or block access even when a drug is medically indicated, creating systemic risk of therapeutic degradation. This shift is non-obvious because patients perceive immediate cost relief while underestimating how insurer governance embeds long-term clinical path dependency, where treatment trajectories are shaped not by biomarkers or physician judgment but by actuarial calculus grounded in population averages.
Therapeutic Risk Externalization
Partial drug coverage that delegates gatekeeping to insurers enables the systemic externalization of clinical risk onto vulnerable patients, who absorb the adverse outcomes of delayed or denied treatment while insurers retain financial savings from restricted access. This transfer operates through asymmetrical accountability—insurers face no liability for denial-induced complications, whereas patients bear the morbidity cost and physicians carry ethical distress. The dynamic is invisible in cost-benefit analyses that treat denials as administrative events rather than medical harms, allowing the system to scale risk displacement under the guise of fiscal responsibility, particularly in Medicaid managed care and ACA marketplace plans where regulatory oversight prioritizes premium stability over care continuity.