Kinship sovereignty
Communities must legally codify elder care as a familial jurisdiction resistant to state oversight through municipal charters. This requires recognized kinship networks—such as extended clans in Navajo Nation chapters or Amish district bishops—to establish binding care protocols that align with local law and are preemptively exempt from mandatory reporting thresholds. The mechanism operates through layered legal pluralism, where tribal or religious legal systems are granted deference under federal frameworks like the Indian Child Welfare Act, extended analogously to elders. What’s underappreciated is that existing legal precedents tolerate parallel care regimes when cultural sovereignty is formally institutionalized, not just informally practiced.
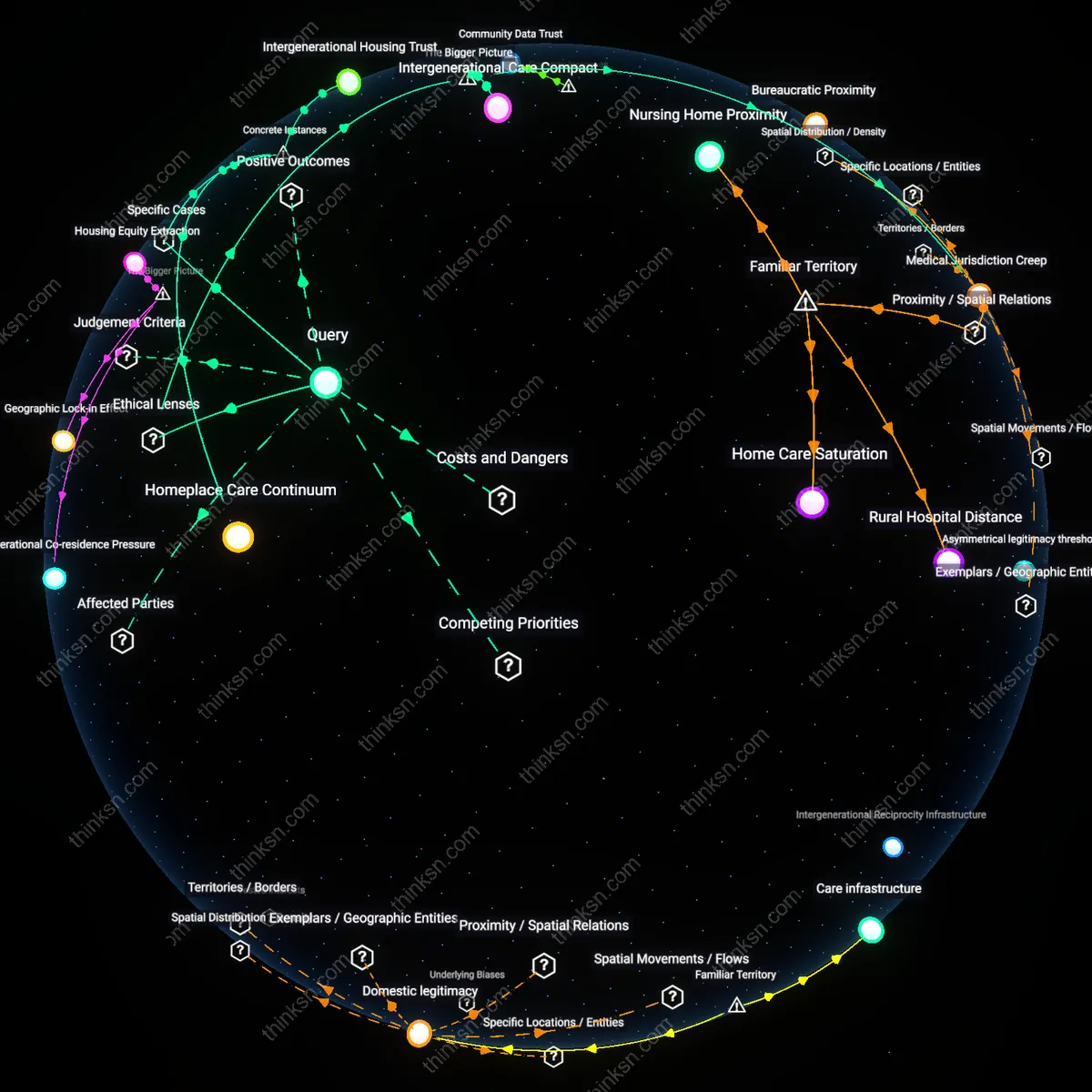
Domestic legitimacy
Families must transform elder care into a publicly verifiable practice through community-recognized caregiving covenants. Neighborhood councils in places like Appalachia or rural Puerto Rico could witness and certify home-based elder support arrangements—documenting safety, consent, and continuity—using locally trusted figures such as pastors, midwives, or retired nurses. This system shifts legitimacy from state compliance to social accountability, activating the underappreciated role of communal trust as a regulatory substitute. The non-obvious insight is that state intervention often follows suspicion, not harm, and visible, socially embedded care neutralizes that perception without external supervision.
Care infrastructure
Households must be equipped with decentralized medical and monitoring tools that make traditional care clinically transparent without state intrusion. Programs like federally subsidized home telehealth kits—distributed through Federally Qualified Health Centers in regions like the Mississippi Delta—enable blood pressure tracking, medication dispensing, and emergency alerts that generate evidence of competent care. This operates through technical intermediation, where data becomes proof-of-care for insurers and regulators without triggering investigations. The overlooked reality is that state intervention often stems from information asymmetry, not cultural conflict, and technology can satisfy regulatory appetites while preserving familial autonomy.
Kinship-adjacent credentialing
Certify non-biological kinship roles as state-recognized care providers through municipal adaptation of health oversight bylaws. A city health department can designate trained neighbors or godparents as legal co-stewards of elder wellbeing, creating a parallel track to familial care rights — this bypasses the assumption that only blood or marital ties legitimate domestic care, and resists institutionalization by embedding trusted outsiders in elder oversight without triggering 'neglect' flags; it is non-obvious because most reform efforts focus on expanding state services rather than diluting biological kinship as the sole basis for care legitimacy, yet many traditional societies rely on ritual kin whose authority evaporates under legal scrutiny.
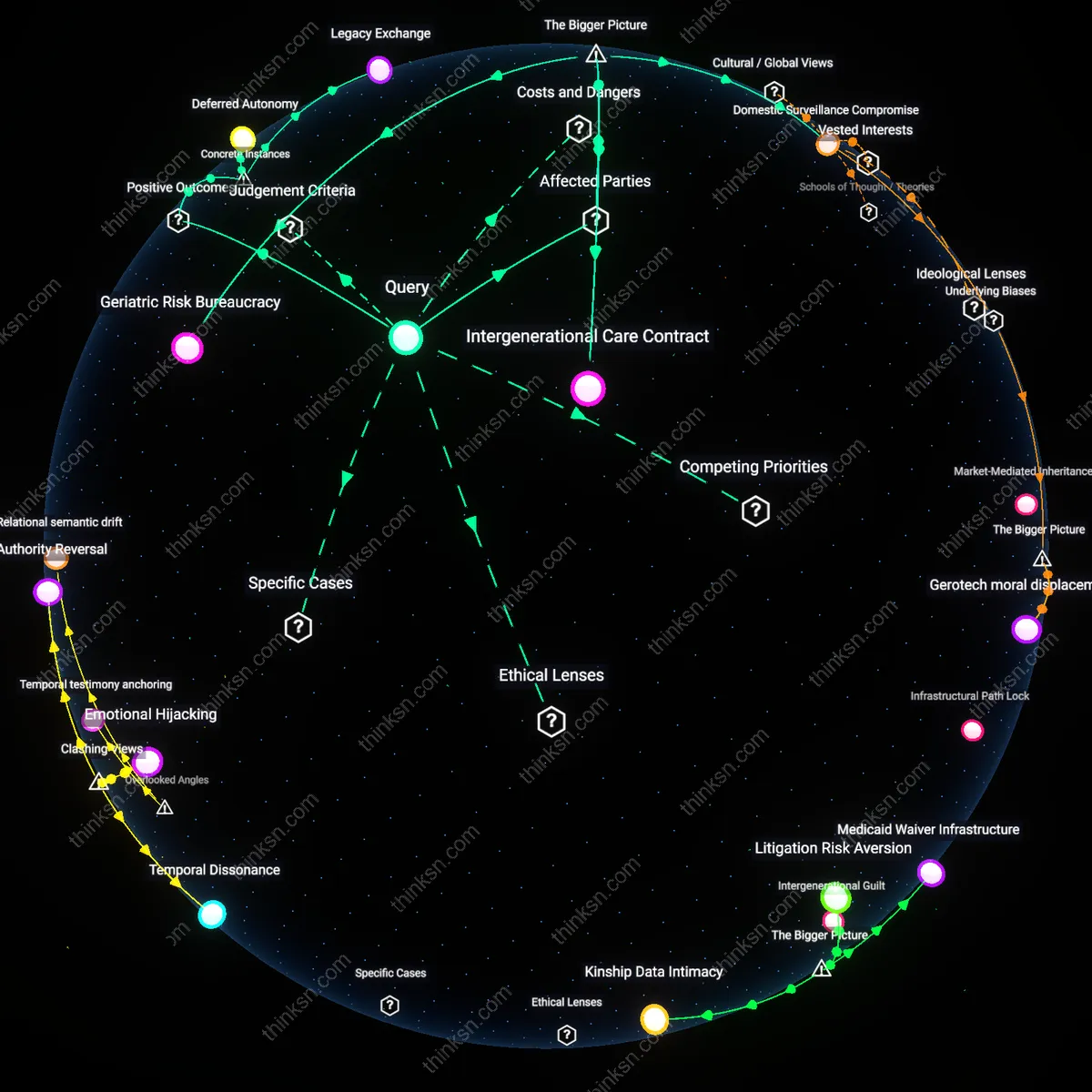
Cultural Legitimacy Threshold
Families can sustain elder care through traditional practices without state intervention only if communal caregiving norms achieve legally tacit recognition by consistently aligning with child protection and elder welfare benchmarks in state-monitored jurisdictions. This occurs when intergenerational caregiving networks maintain health, safety, and dignity outcomes at levels indistinguishable from state-validated models, thereby reducing triggers for mandatory reporting; the mechanism operates through feedback between community accountability and institutional non-interference, where successful outcomes reinforce tolerance for cultural deviation. What is non-obvious is that the state’s withdrawal is not passive neglect but a conditional equilibrium dependent on invisible, community-enforced compliance with implicit regulatory thresholds.
Intergenerational Reciprocity Infrastructure
Sustainable traditional elder care persists where younger family members are reliably assured future benefits from current caregiving, creating a self-reinforcing cycle of obligation and return supported by kinship economies that bind labor, housing, and inheritance across generations. This feedback loop depends on functioning systems of reciprocal exchange—such as lineage-based property transfer or community labor rotation—that transform care into an investment rather than a burden, embedded within rural or diasporic networks where formal elder services are under-resourced. The underappreciated dynamic is that these systems deter state intervention not through secrecy but through functional resilience, making external oversight appear redundant to local actors and officials alike.
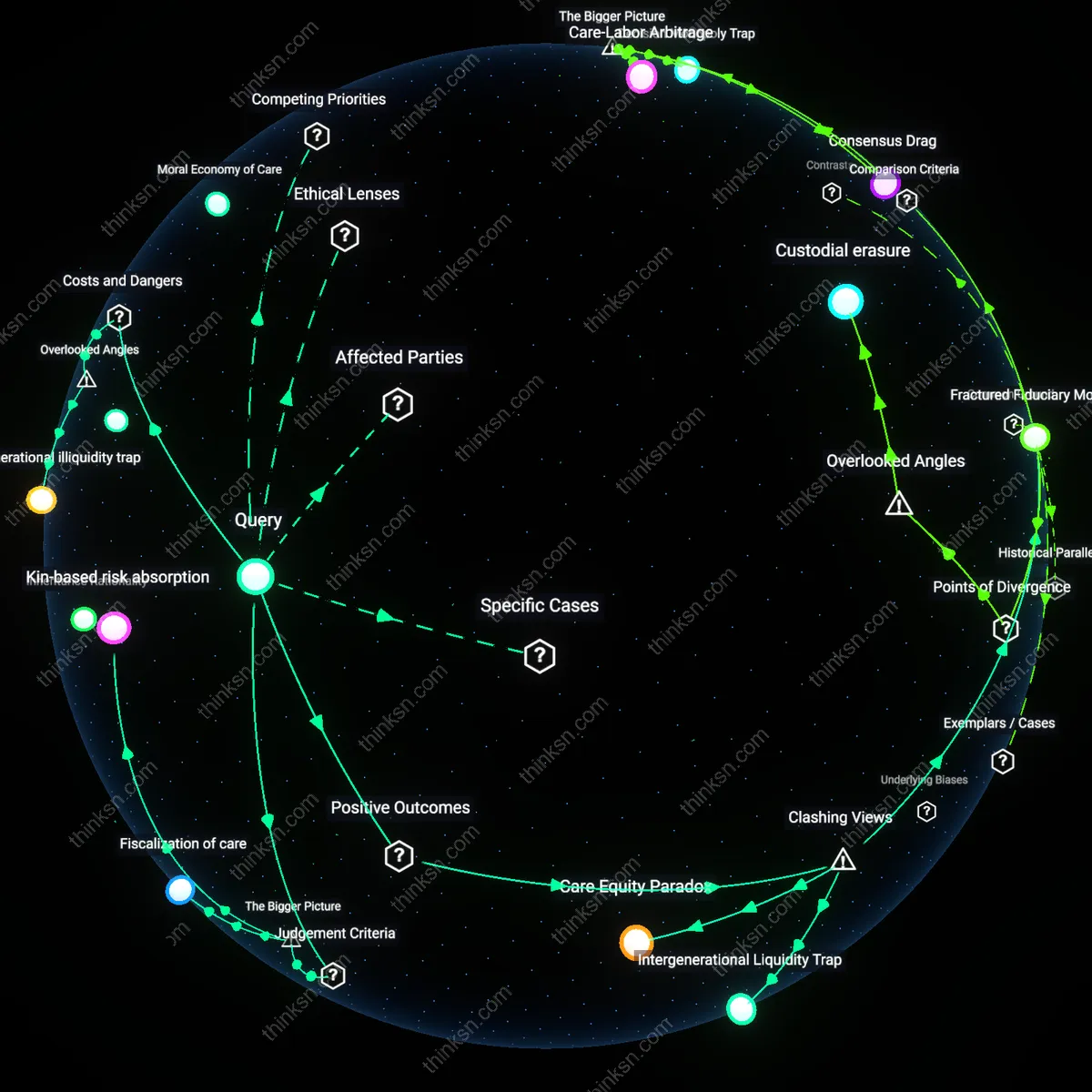
Regulatory Arbitrage Capacity
Families avoid state intervention in elder care when they can exploit jurisdictional variation in elder protection enforcement, enabling traditional practices to persist in regions where bureaucratic reach is low or cultural pluralism is formally acknowledged. This balancing loop emerges in federal or decentralized states—such as in Indigenous reserves or geographically remote municipalities—where local authority absorbs oversight functions and redefines compliance criteria, allowing traditional models to operate under differentiated regulatory standards. The non-obvious insight is that sustainability does not stem from cultural resistance alone, but from a systemic loophole where localized governance becomes a de facto enabler of cultural continuity under national legal frameworks.
Bureaucratic latency
Families avoid state intervention when informal elder care operates beneath the reporting thresholds of mandatory surveillance systems like Adult Protective Services, which expanded rapidly after the 1981 Older Americans Act amendments. The critical shift occurred when risk-based assessment protocols prioritized visible harm over cultural continuity, creating a temporal lag between family action and bureaucratic response—this latency allows customary practices to persist in the shadows of underfunded systems. The underappreciated dynamic is that neglect is not always intervened upon; it is sometimes simply deprioritized.
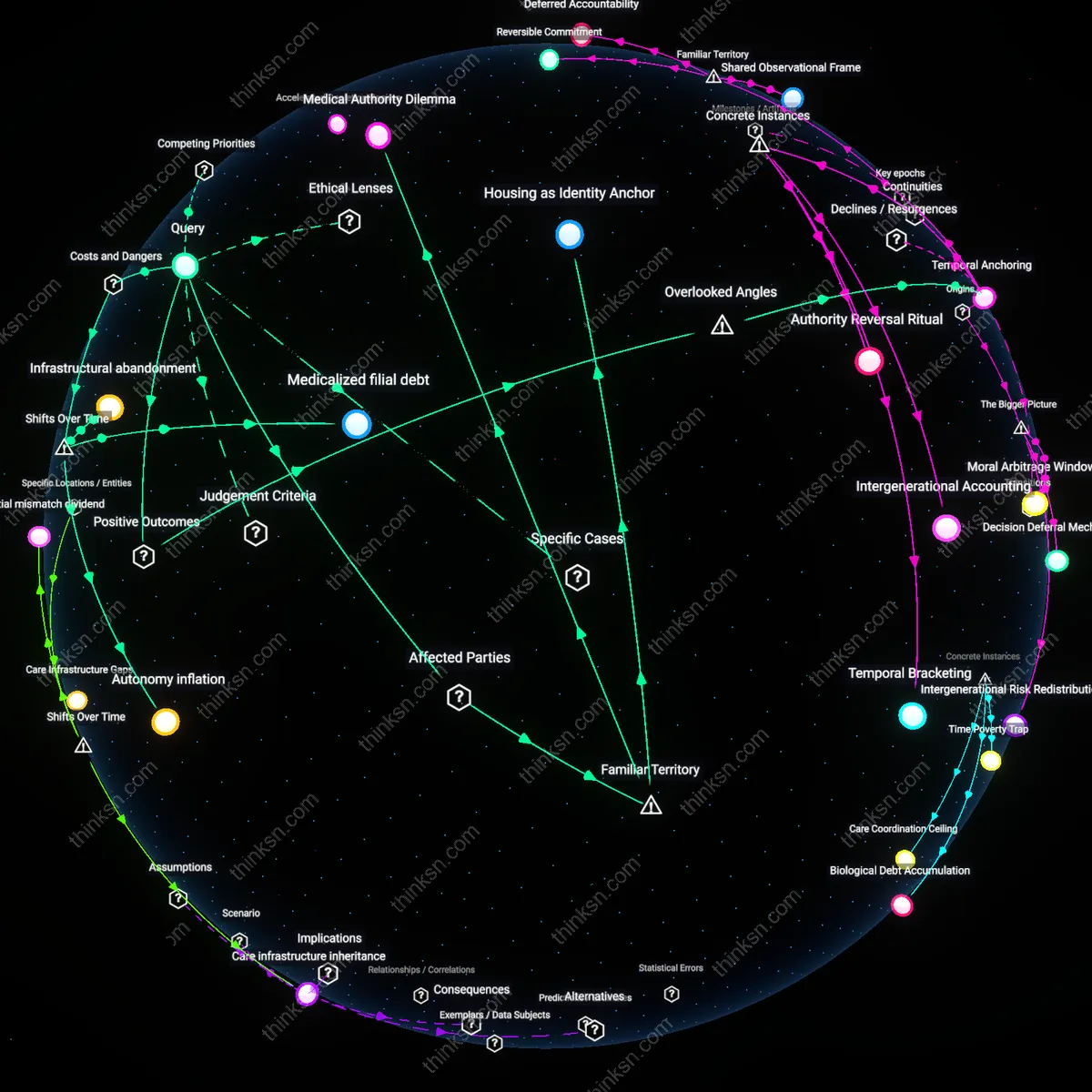
Filial debt economies
Elder care remains a family responsibility without state intrusion where intergenerational property transfers are legally binding, as seen in agrarian municipalities in southern China after the 1996 Elder Rights Law allowed local codification of filial obligations tied to land inheritance. The pivotal transition came when rural collectives devolved land-use rights to households, shifting elder security from communal to familial balance sheets—making care a precondition of ownership. This reveals that traditional practice endures not through sentiment but through enforceable economic contracts embedded in land tenure.
Kinship Bureaucracy
Families must internalize state-like oversight functions to avoid state intervention, such as documenting care routines and health outcomes to prove adequacy. This transforms intimate household practices into accountable systems that mimic regulatory frameworks, revealing that traditional care persists not through resistance to state logic but by replicating its mechanisms in miniature. The non-obvious insight is that autonomy from state intervention requires families to become bureaucratic—precisely the structure they are assumed to oppose.
Vernacular Legibility
Elders must be cared for in ways that produce culturally recognizable markers of dignity that inspectors cannot dispute, such as ceremonial meal-sharing or visible mobility support, even if actual health outcomes are stable. This performance makes traditional practices legible to external evaluators without altering their substance, exposing how compliance is secured through symbolic adherence rather than structural change. The clash lies in showing that authenticity survives not by resisting inspection but by strategically conforming to its aesthetic demands.
Care Friction
Communities must institutionalize quiet enforcement of traditional norms, where neighbors and religious leaders apply social pressure that deters visible elder neglect, thereby preempting official reporting. This shifts the function of compliance from state monitoring to community policing, revealing that state non-intervention depends on informal coercion, not passive tradition. The friction emerges in recognizing that autonomy from the state is maintained through tighter local control, not freedom from regulation.
Jurisdictional carve-out
Formal recognition of Indigenous jurisdiction over elder care in Nunavut enables Inuit families to apply traditional caregiving practices without state interference, because the territorial government delegates authority for health and social services through Inuit-led institutions like Nunavut Tunngavik Incorporated. This sovereignty-based accommodation allows intergenerational co-residence, oral decision-making, and land-based care to function as legitimate forms of elder support, not neglect, revealing that state non-intervention depends not on cultural tolerance but on legally delimited self-governance.
Kinship accountability network
In rural Oaxaca, Zapotec communities maintain elder care through communal land tenure and cargo systems that obligate adult children to house and serve aging parents as part of rotational community service, making familial duty both socially enforced and economically feasible through collective resource pooling. State intervention is avoided not because authorities are absent but because observable reciprocity, witnessed by neighbors and sanctioned by community councils, produces verifiable care outcomes that preempt child protection-style oversight, exposing that informal monitoring by embedded social institutions can substitute for formal bureaucratic surveillance.
Asymmetrical legitimacy threshold
In Japan’s 2005 revision of the Long-Term Care Insurance Act, families who care for elders at home receive equivalent state benefits and legal recognition as institutional providers, but only if they adhere to clinical care protocols, thereby excluding truly traditional practices — unless conducted in designated 'cultural preservation zones' like parts of Okinawa where localized models of multi-home caregiving are accepted as valid despite diverging from national standards. This reveals that states permit traditional care not when it is effective, but when it becomes symbolically contained within policy exception zones that protect the dominance of state-defined care paradigms.