Should Side Effects Outweigh Reduced Heart-Failure Risks?
Analysis reveals 9 key thematic connections.
Key Findings
Clinical Inertia
It is rational for primary care physicians in underresourced U.S. safety-net clinics to prioritize short-term hospitalization reductions over long-term survival because systemic underfunding and patient turnover make adherence to complex, long-term risk metrics impractical. These clinicians face institutional pressure to demonstrate immediate outcomes, leading them to accept higher side-effect burdens as a calculable trade-off for reducing observable, near-term events like heart-failure admissions. This reveals that apparent clinical irrationality often reflects rational adaptation to structural constraints in care delivery—where reliability of follow-up is weaker than pharmaceutical risk, diminishing the utility of survival-focused guidelines.
Pharmaco-Social Contract
It is rational for elderly patients in high-isolation demographics, such as rural Appalachia, to accept more side effects for marginal hospitalization gains because the social cost of hospitalization—loss of independence, disruption of kinship networks, and erosion of self-worth—exceeds the abstract benefit of uncertain longevity. For these individuals, avoiding institutionalization is a primary survival goal in itself, one not captured in clinical trial endpoints. This exposes a hidden alignment between patient autonomy and pharmaceutical risk-taking when medical outcomes serve as proxies for social continuity.
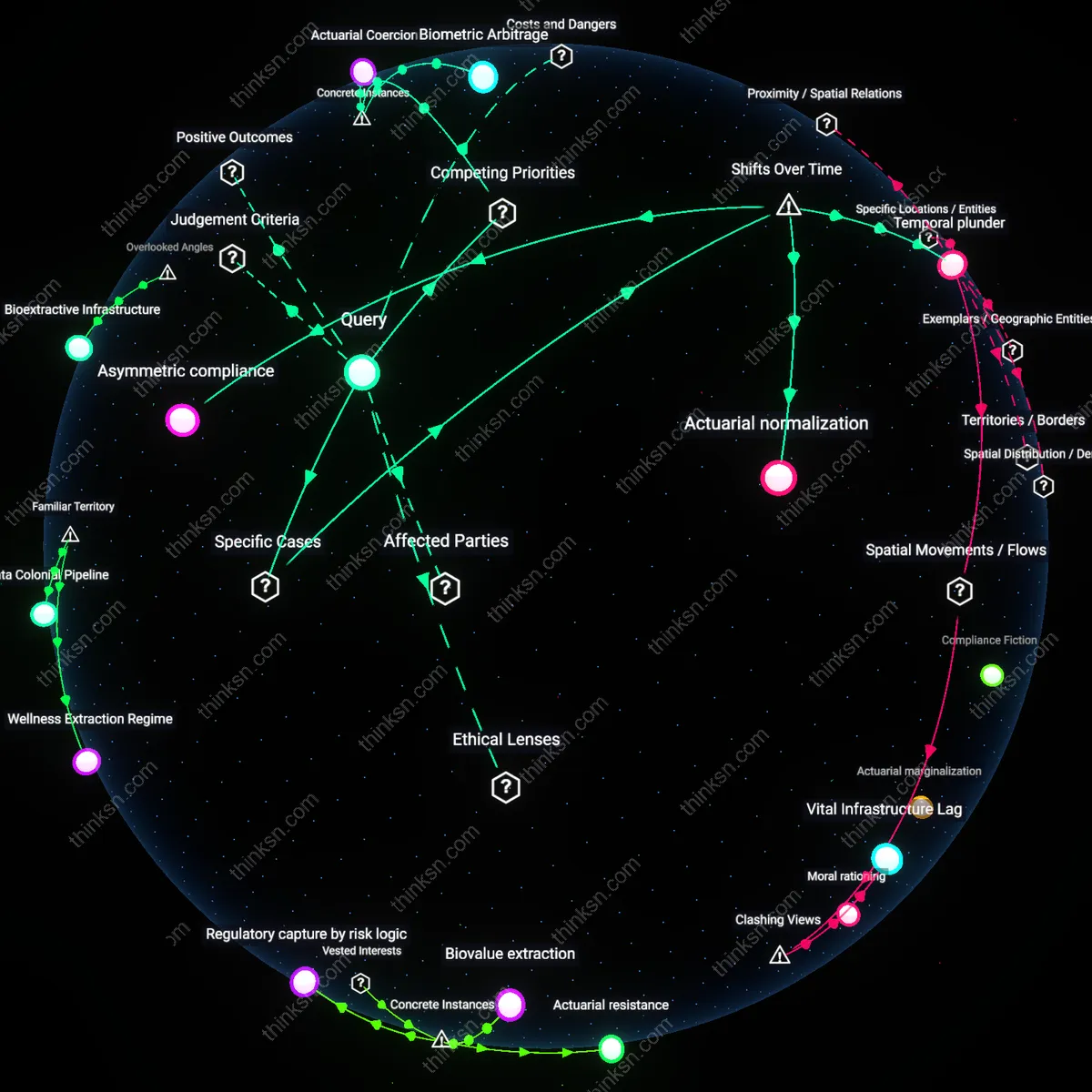
Regulatory Arbitrage
It is rational for pharmaceutical firms to promote side-effect-heavy antihypertensives with minor hospitalization benefits because regulatory frameworks reward reductions in specific event rates more consistently than overall mortality improvements, enabling favorable formulary placement and litigation shielding. By designing trials that optimize for FDA-recognized endpoints while excluding long-term mortality follow-up, companies exploit a loophole where marginal clinical utility becomes a compliance asset. This demonstrates that drug risk-benefit assessments are not purely medical but strategically shaped by regulatory footprinting.
Risk Tradeoff Heuristics
Yes, it is rational to accept more side effects for fewer heart-failure hospitalizations because patients and clinicians routinely prioritize immediate, tangible harms over uncertain long-term outcomes. This occurs through shared decision-making in outpatient cardiology settings, where tools like risk calculators frame side effects as manageable nuisances compared to the highly salient burden of hospitalization—especially among older adults managing multiple medications at home. What is underappreciated is that this habit aligns with ingrained cognitive heuristics that weigh visible, near-term crises more heavily than statistical survival gains, making the tradeoff feel proportionate even when evidence on mortality is absent.
Clinical Momentum Preservation
Yes, it is rational because continuing or intensifying medication maintains momentum in chronic disease management, reinforcing patient trust in the treatment trajectory within primary care systems where discontinuity raises anxiety. Doctors in community health centers rely on stable regimens to signal control over illness, and reducing hospitalizations—regardless of survival—serves as a publicly reported quality metric that validates care quality. The overlooked insight is that this reflects a system-level preference for visible markers of progress, where avoiding hospitalization becomes a proxy for overall success, even when hard endpoints remain unclear.
Pharmaceutical Symmetry Assumption
Yes, it is rational because the public implicitly assumes that medications producing measurable clinical benefits, such as reduced hospitalizations, are likely to eventually demonstrate survival improvement—a belief reinforced by decades of post-marketing data for drugs like ACE inhibitors. This assumption operates through media narratives and pharmaceutical branding that equate 'heart protection' with longevity, shaping patient expectations in pharmacy waiting lines and telehealth visits. The unexamined core is that people treat side-effect tolerance as proof of efficacy, borrowing from antibiotic-era logic where stronger treatment implies stronger benefit, despite incomplete evidence in chronic disease.
Prescription Debt
It is irrational to accept increased side effects for uncertain survival gains because each additional side effect accumulates prescription debt—where managing drug-induced symptoms leads to further medication, creating cascading polypharmacy. This dynamic is especially pronounced in elderly patients on multiple chronic therapies, where a single side effect like hyponatremia from a diuretic triggers diagnostic chases and new prescriptions, overloading physiological resilience. The oversight lies in treating side effects as isolated incidents rather than systemic liabilities that propagate downstream clinical burden, distorting the perceived benefit of the original drug by embedding hidden treatment inertia.
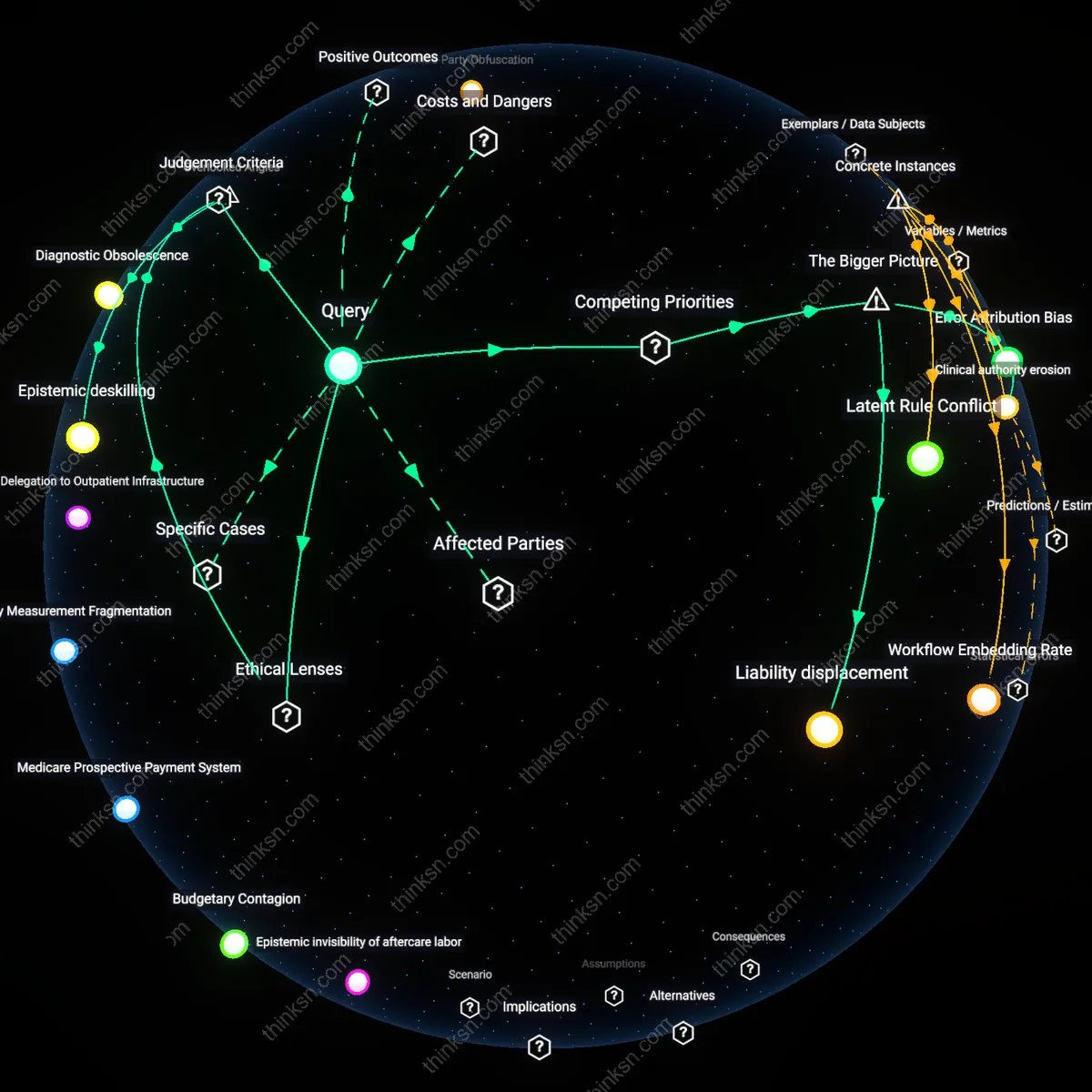
Diagnostic Attribution Failure
It is irrational because side effects from blood pressure drugs are frequently misattributed to aging or comorbidities rather than the medication, leading to delayed discontinuation and prolonged harm. In primary care settings, symptoms like fatigue or orthostasis are often coded as ‘general malaise’ or ‘geriatric decline,’ shielding the true cost of treatment from clinical audit and decision-making loops. This misattribution systematically underreports drug burden, distorting risk-benefit assessments in guidelines that rely on incident hospitalization data while ignoring the diffuse suffering embedded in daily functioning lost to poorly captured adverse effects.
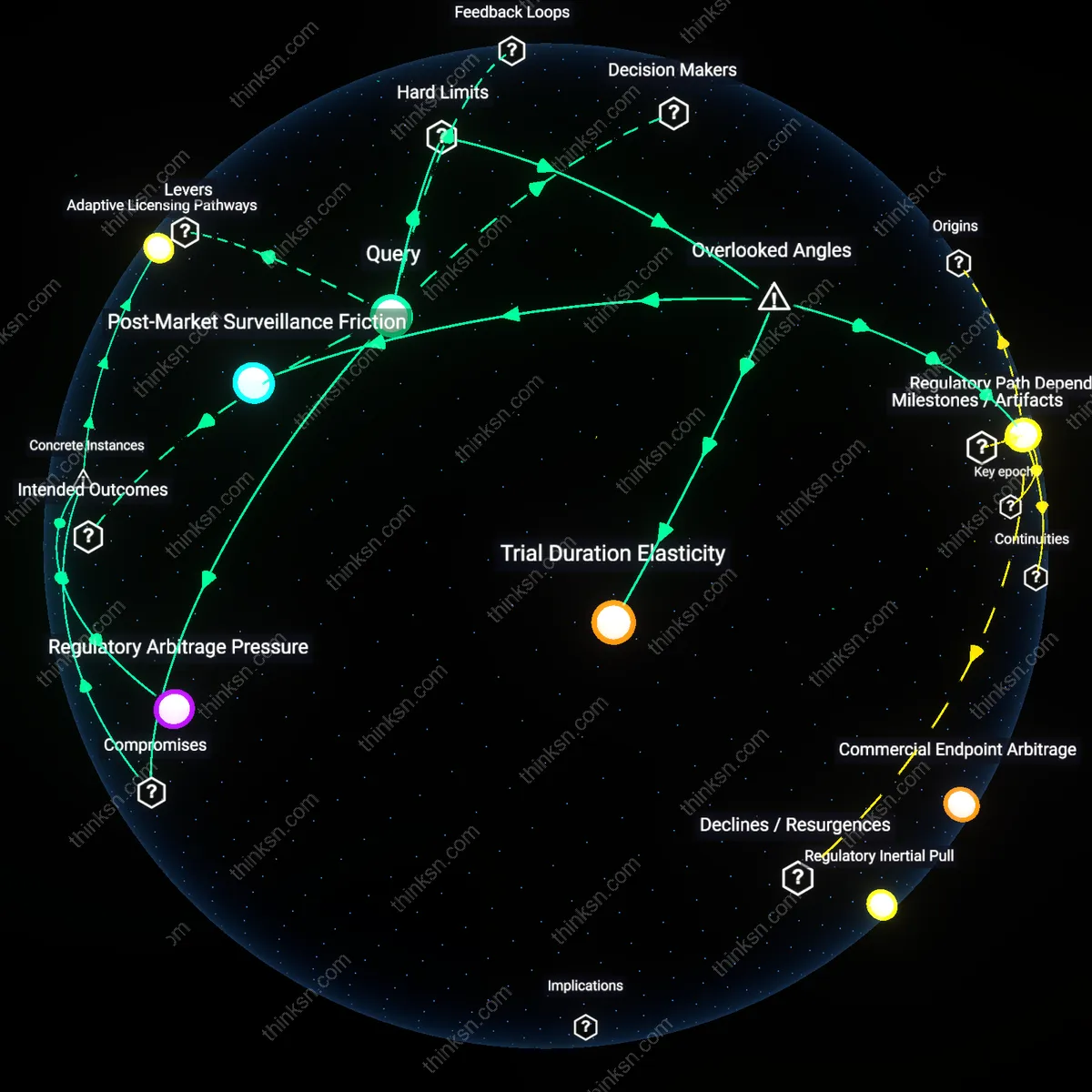
Trial-Time Fugue
It is irrational because the short duration of clinical trials masks the divergence between transient trial efficacy and long-term real-world harm, creating a temporal illusion of benefit. Trials measuring heart-failure hospitalizations over 12–24 months cannot capture the cumulative impact of side effects that erode adherence or cause subclinical organ damage over decades, such as renal decline from chronic hypotension. The overlooked issue is that regulatory and clinical cognition operates in trial-time fugue—privileging narrow, time-bound outcomes while discounting the nonlinear accrual of harm that only emerges in extended patient trajectories, thus privileging statistical significance over biological consequence.