Refusing Abortion Care: EMTALA Conflict in Hospitals?
Analysis reveals 4 key thematic connections.
Key Findings
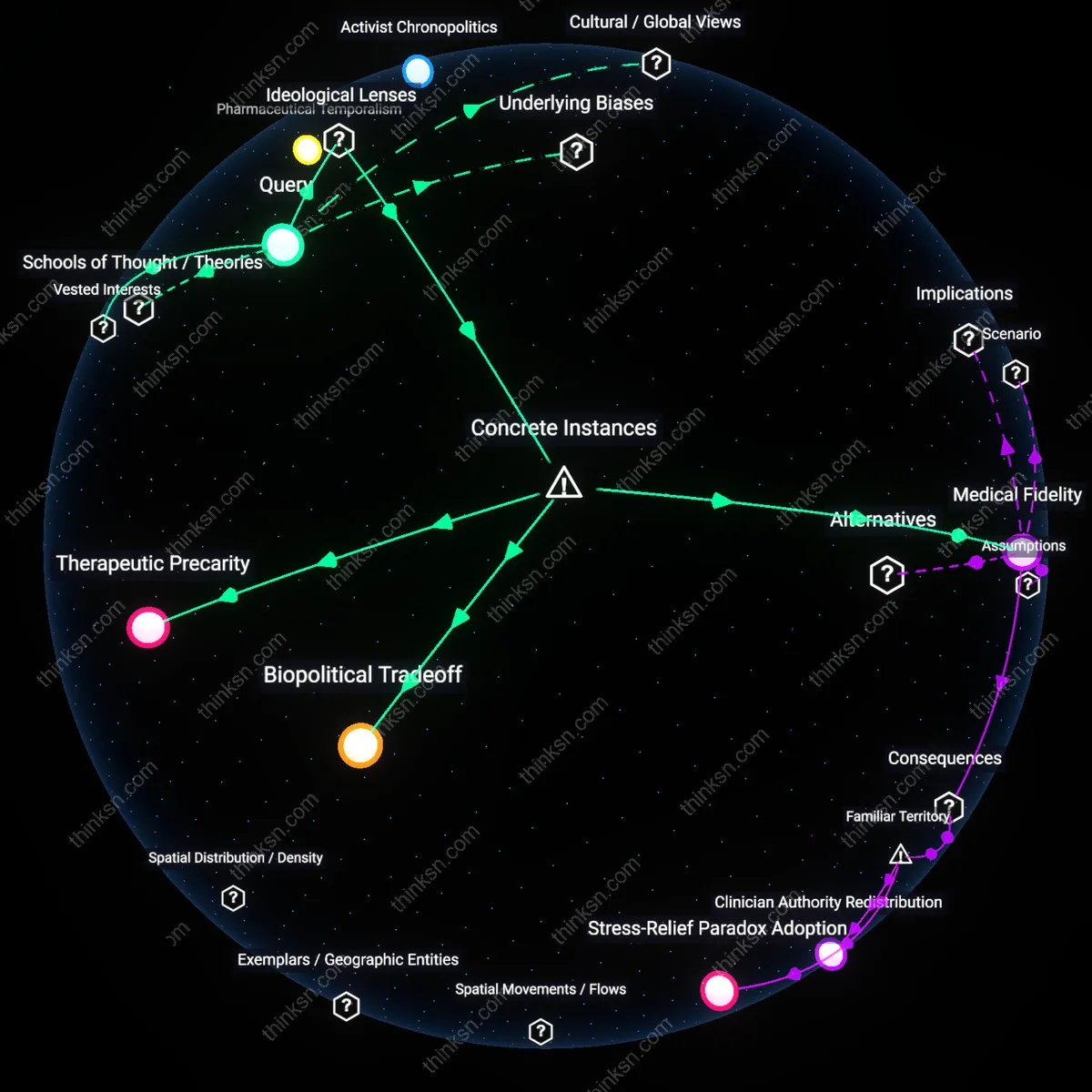
Patient Dispossession
Hospital policies that deny abortion care after a gestational limit directly violate EMTALA’s mandate to provide stabilizing treatment by transferring the clinical burden of decision-making from medical judgment to bureaucratic compliance, thereby disempowering pregnant patients facing emergent complications; this shift treats the patient’s body as a site of institutional risk management rather than a subject of emergency care, which disproportionately impacts low-income women and people of color who rely on public hospitals—revealing that the law’s enforcement failure is not an oversight but a structural outcome of prioritizing administrative uniformity over clinical discretion.
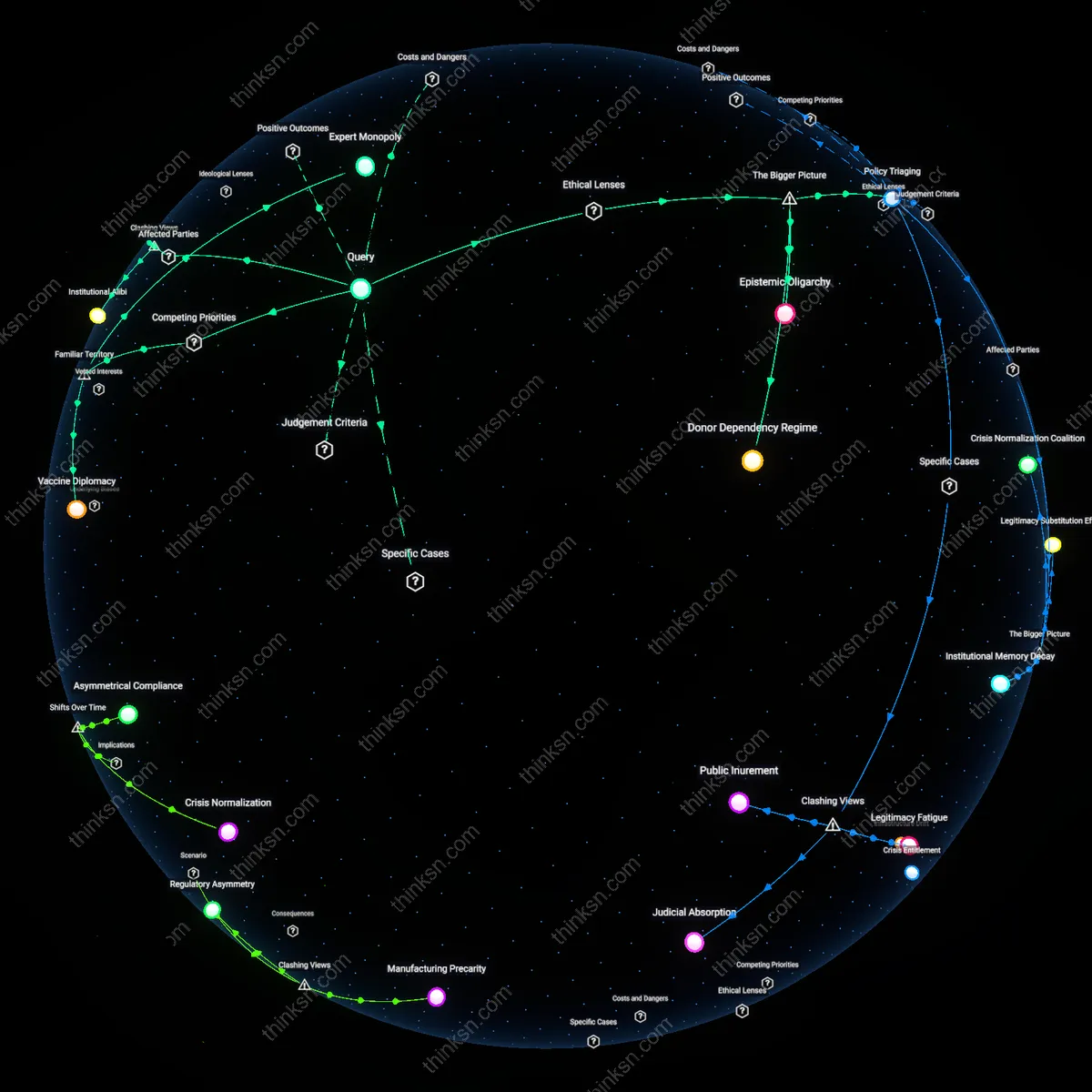
Regulatory Shielding
EMTALA is weaponized by hospitals to justify gestational cutoffs not because the law permits such denials but because non-enforcement of EMTALA’s reproductive health provisions creates a de facto legal shield, allowing institutions to align with state abortion bans under the guise of regulatory compliance; this dynamic positions hospitals as strategic interpreters of federal law in ways that override emergency care obligations, privileging institutional liability avoidance over patient survival—exposing how ambiguity in federal enforcement enables healthcare entities to become autonomous arbiters of life-threatening care.
Bureaucratic Delay Hazard
A hospital in South Carolina denying dilation and evacuation for a septic abortion at 22 weeks due to gestational limits directly caused prolonged infection and preventable organ stress, because administrative adherence to state-specific gestational cutoffs delayed emergent intervention despite EMTALA’s mandate to stabilize. The mechanism—prioritizing legal compliance over clinical urgency—reveals a systemic flaw where federal emergency care guarantees are nullified by state abortion laws, a risk often obscured by framing EMTALA as universally protective. This instance exposes how procedural rigidity amplifies physiological harm even when federal law appears to safeguard care.
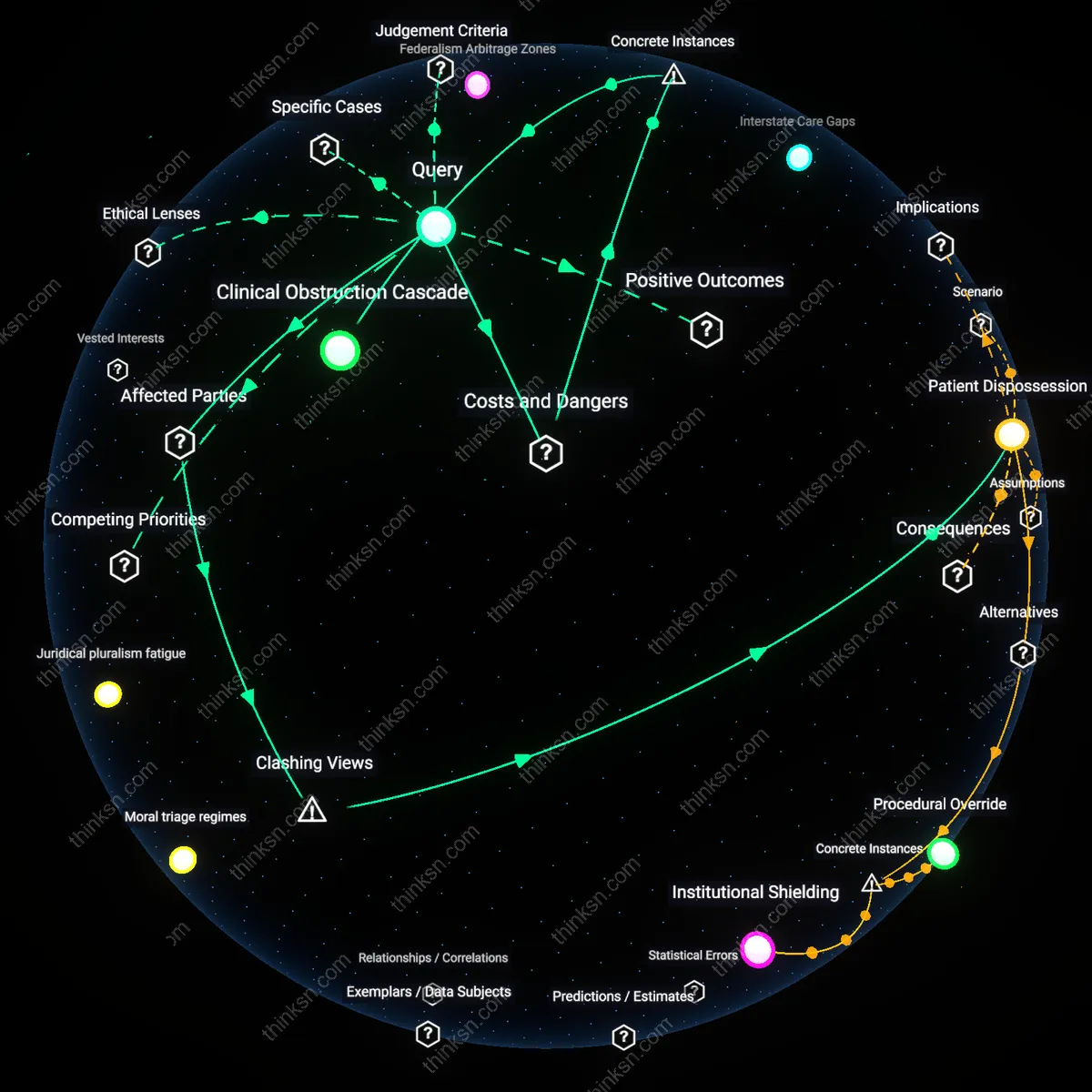
Clinical Obstruction Cascade
At a Catholic-affiliated hospital in Michigan, a woman experiencing incomplete miscarriage at 17 weeks was denied standard surgical management due to institutional policy aligned with religious directives, necessitating multiple failed medication attempts that led to hemorrhage and ICU admission, because the hospital’s formal affiliation with the Ethical and Religious Directives for Catholic Health Care Services restricted care despite EMTALA’s stabilization requirements. This case illustrates how third-party institutional frameworks—distinct from state law—can operationalize gestational denials that indirectly but predictably escalate emergency risk, a seldom acknowledged vector of non-compliance embedded in privatized health systems.