High Hospital Admin Staff: Whose Benefits Outweigh Patient Costs?
Analysis reveals 9 key thematic connections.
Key Findings
Administrative Rent Extraction
Salaries for non-clinical executives at HCA Healthcare have consistently exceeded those of comparable health systems, enabled by investor-pressure to increase billing efficiency, which expanded oversight staff despite stagnant patient outcomes—this illustrates how private equity-aligned hospital chains redistribute resources toward administrative roles that optimize revenue capture over care delivery, revealing that financialization creates a rent-extractive bureaucracy.
Patient Time Tax
At NewYork-Presbyterian Hospital between 2015 and 2018, patients spent an average of 82 minutes in pre-service logistics such as insurance verification and consent processing—tasks ballooned by compliance and billing administrators—demonstrating that staffing choices ostensibly ensuring regulatory compliance or financial stability impose deferred access, misallocated labor, and psychological burden on patients, making time a covert cost of administrative bloat.
Regulatory Labor Dumping
Following the 2010 Affordable Care Act’s reporting mandates, the University of Michigan Health System added 137 full-time compliance officers, a decision driven by federal audit risks rather than clinical need—this shifted labor costs from public oversight agencies to hospitals, then indirectly onto patients through higher charges and restricted access, exposing how federal policy design outsources bureaucratic burden to frontline institutions while obscuring its real cost bearers.
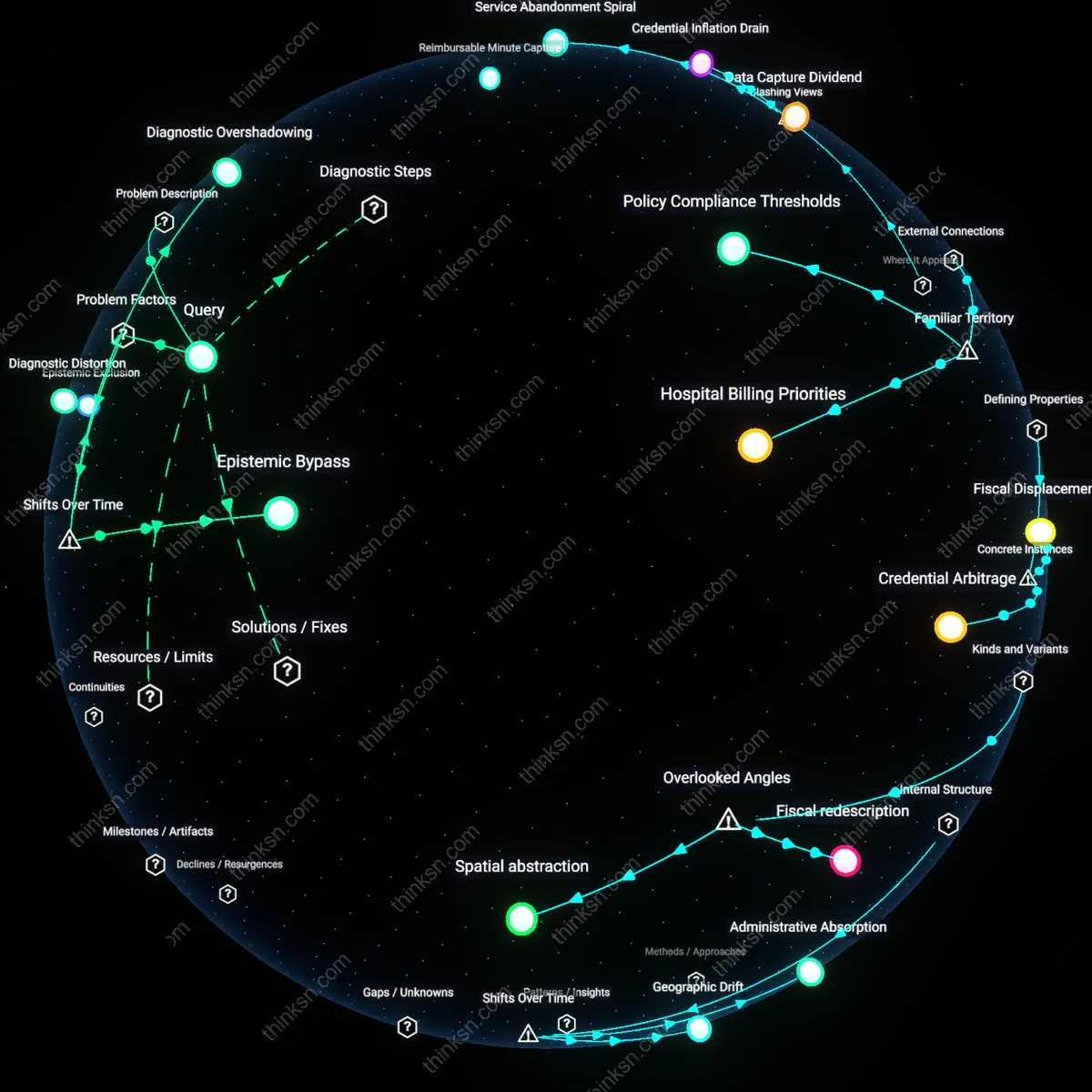
Bureaucratic Immunity
High administrative staffing in US hospitals primarily benefits hospital executives and insurers by enabling deflection of liability onto procedural compliance, where layers of documentation and coding staff shield decision-makers from malpractice exposure, creating a self-protective institutional immune system that prioritizes audit readiness over clinical agility, a dynamic underrecognized because it frames administrative bloat not as inefficiency but as a calculated risk-transfer mechanism that systematically shifts legal vulnerability from providers to patients, who absorb hidden costs through delayed care and diagnostic overshadowing.
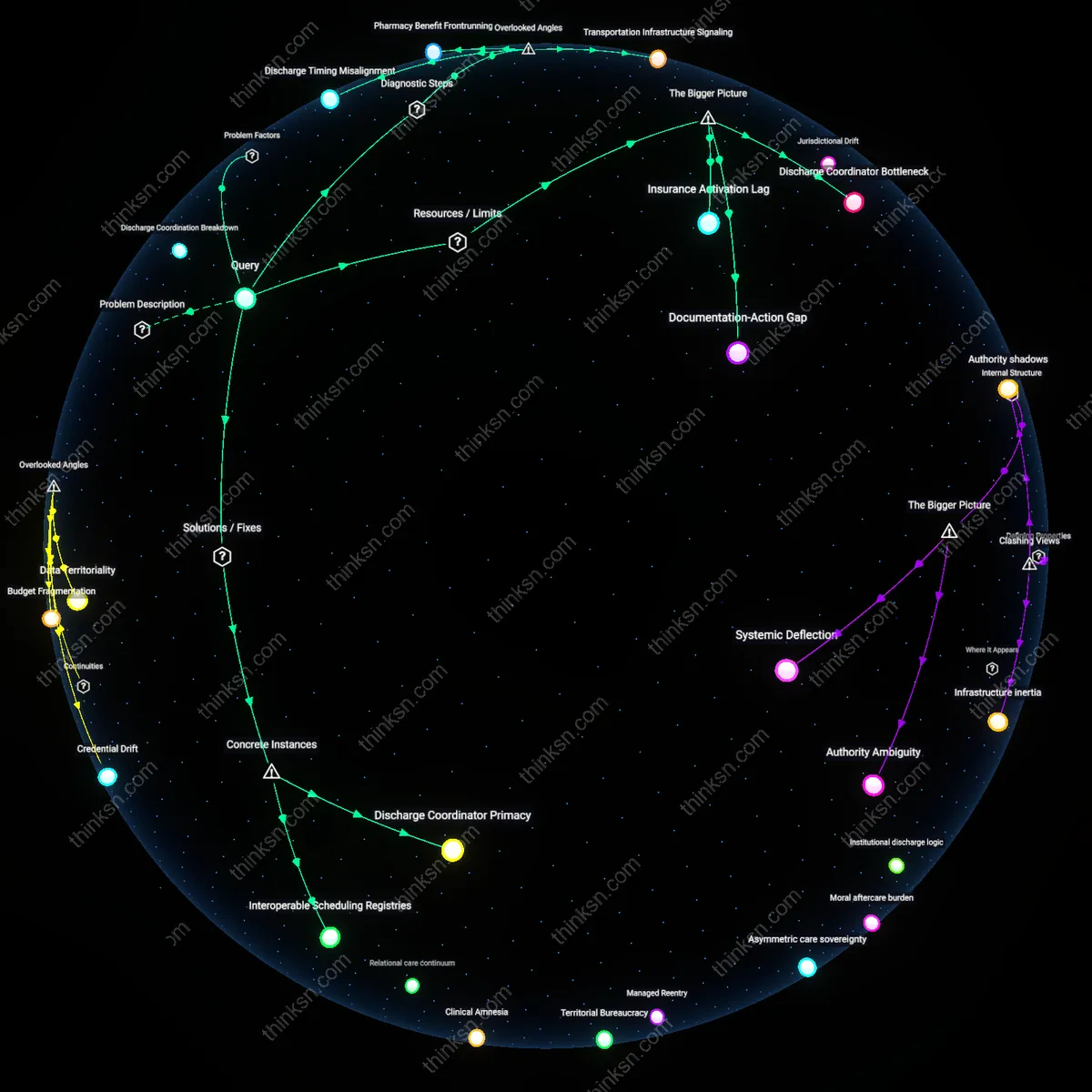
Data Fiefdoms
The expansion of hospital administrative roles disproportionately empowers middle-tier health information managers and revenue cycle analysts who leverage patient data as controlled currency, extracting value through granular coding, billing stratagems, and interoperability gatekeeping, a system that undermines the intuitive belief that data centralization improves care by revealing instead how decentralized data silos are intentionally maintained to maximize reimbursement eligibility and reduce payer pushback, making patients bear hidden costs via fragmented records and misaligned care coordination that serve institutional revenue goals, not clinical outcomes.
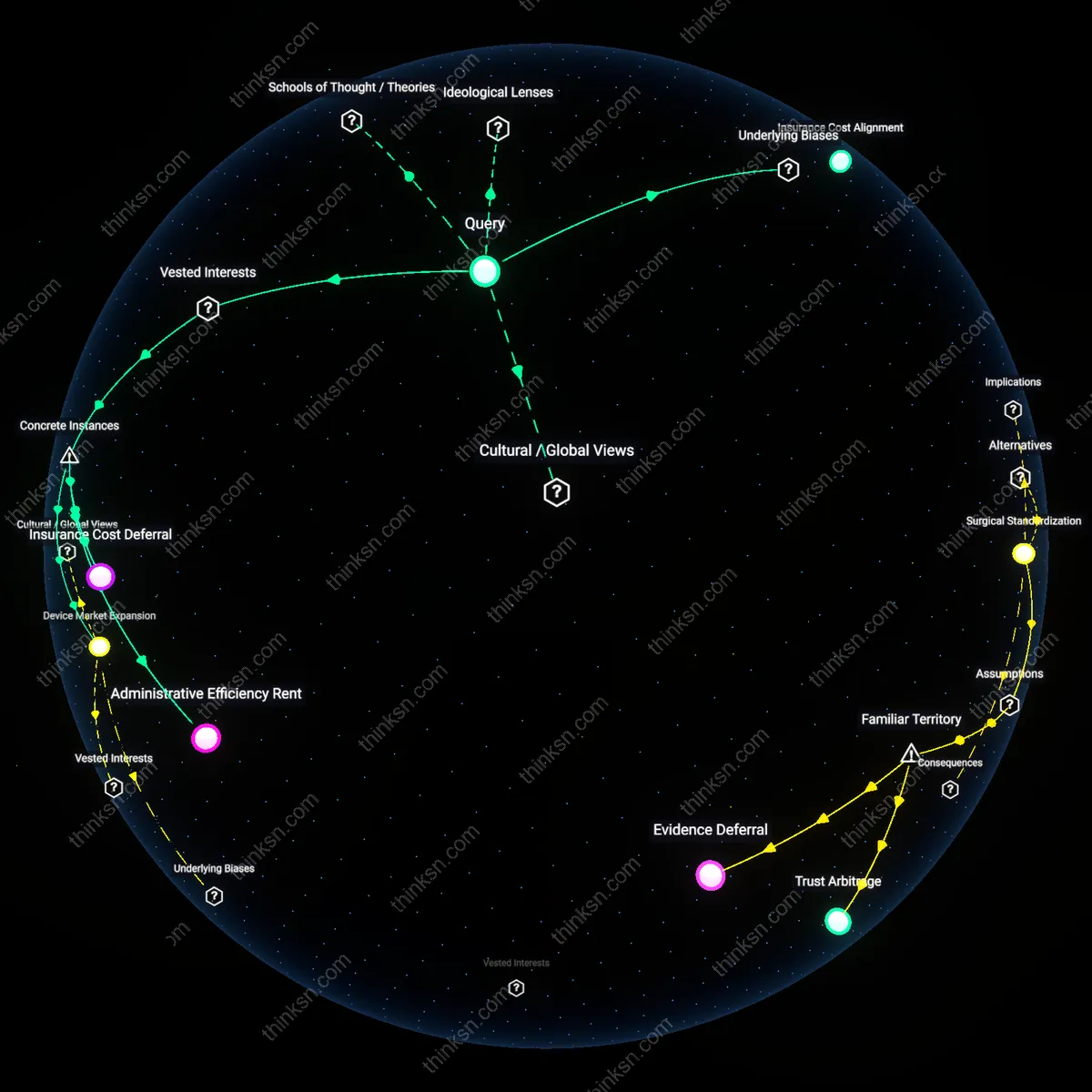
Regulatory Arbitrage
Federal and state regulatory frameworks incentivize hospitals to staff administrators as financial instruments rather than service enhancers, where skilled grant writers, compliance officers, and billing specialists convert regulatory complexity into revenue streams through Medicare disproportionate share hospital (DSH) payments, Medicaid waivers, and value-based billing loopholes, subverting the assumption that regulation inherently protects patients by showing how those same rules are gamed to extract public funds while offloading cost and access burdens onto uninsured and underinsured populations, whose hidden costs include exclusion from care pathways deliberately engineered to favor billable encounters over preventive support.
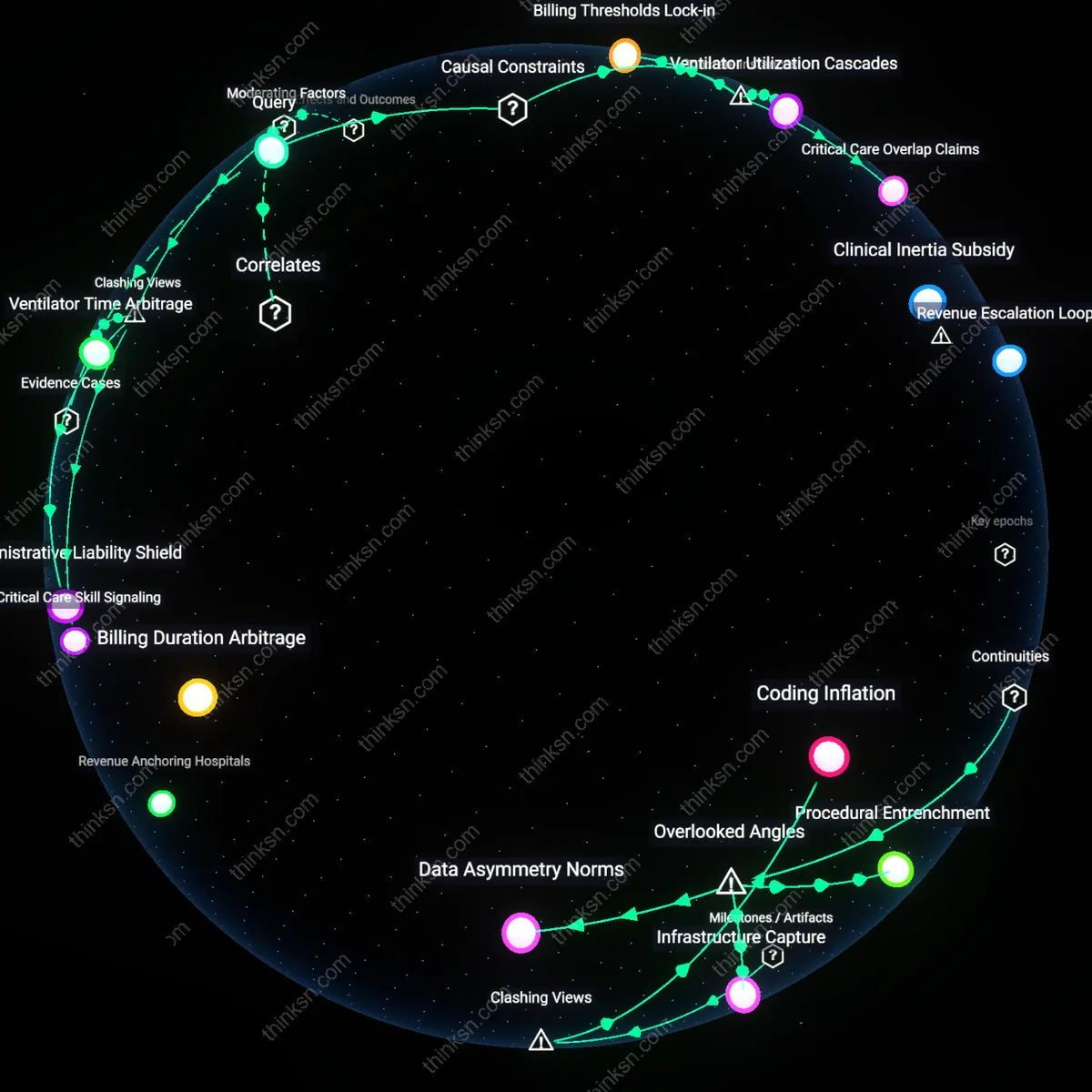
Revenue Cycle Entropy
Hospital billing departments with oversized administrative staffs directly increase the complexity and opacity of patient invoices, which benefits third-party collection agencies that profit from unresolved or misrouted debt. This occurs because large administrative units fragment billing workflows across multiple contractors and software platforms, creating data gaps that make it harder for patients to dispute charges—especially at hospitals like HCA Healthcare, where outsourced collections are systemically embedded. The non-obvious insight is that administrative bloat does not merely raise overhead; it actively generates financial friction that becomes a revenue stream for allied debt entities, shifting the cost of inefficiency onto vulnerable patients through unanticipated collections.
Compliance Theater
Accreditation-driven administrative hiring in hospitals such as those within the Kaiser Permanente network benefits internal compliance officers and external auditors by creating elaborate documentation rituals that appear to meet regulatory standards without improving care. This occurs because federal mandates like EMTALA and HIPAA are enforced through paperwork audits, not patient outcome reviews, incentivizing hospitals to deploy staff in roles that produce reportability rather than accountability. The overlooked dynamic is that administrative staffing functions less as support and more as performative governance—masking care deficiencies beneath layers of procedural demonstration, which indirectly raises patient risk when clinical needs are deprioritized to meet artifact-producing benchmarks.
Clinical Divestment Spiral
High administrative staffing in urban safety-net hospitals like Cook County Hospital redirects budget allocations away from care coordination roles, disproportionately harming low-income patients who rely on social work and navigation services. This occurs because fixed funding pools are increasingly captured by IT and management positions tied to federal reimbursement tracking, leaving frontline clinical support roles underfilled despite rising patient complexity. The hidden dependency revealed is that administrative expansion does not just add cost—it actively cannibalizes non-physician clinical capacity, degrading the very services most critical to patient adherence and outcomes in marginalized populations.