Abortion Tourism Reveals Economic Divide in Healthcare Access?
Analysis reveals 7 key thematic connections.
Key Findings
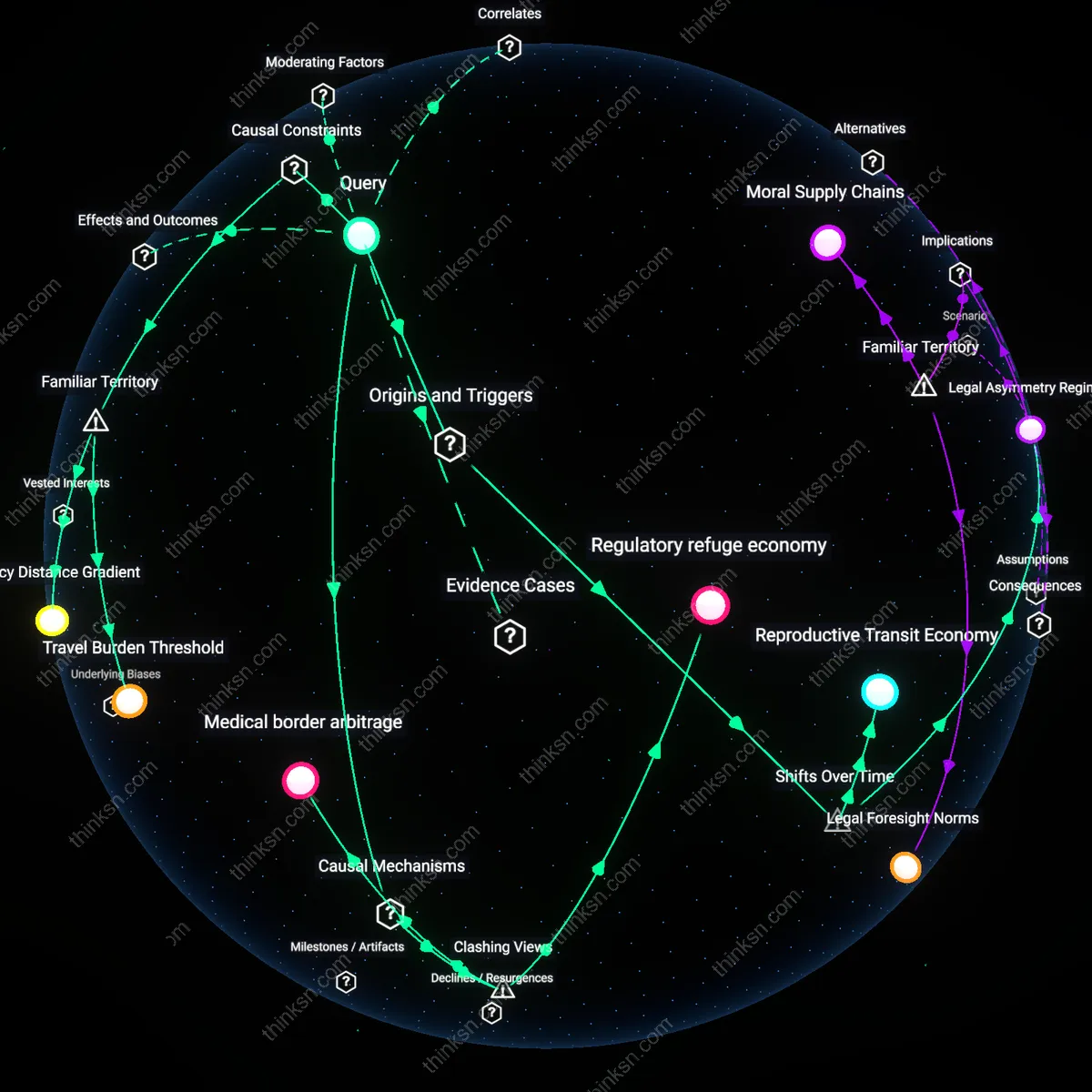
Legal Asymmetry Regime
The rise of abortion tourism since 2022 emerged directly from the abrupt legal fragmentation following the Dobbs v. Jackson decision, which abolished federally protected abortion access and activated trigger laws in 13 states, forcing patients from states like Texas and Missouri to travel over 500 miles on average to clinics in Illinois, Colorado, or New Mexico. This spatial displacement institutionalized a tiered system where mobility—not medical need—determines care access, revealing how a sudden judicial reversal converted constitutional rights into geographically stratified privileges. The non-obvious effect is that pre-Dobbs incremental restrictions (e.g., TRAP laws) had already conditioned healthcare infrastructure for crisis, making the post-Dobbs surge in cross-state travel a spatial escalation of prior regulatory attrition rather than an unforeseen rupture.
Reproductive Transit Economy
Abortion tourism grew into a structured logistical enterprise after 2017, as declining clinic density in the South and Midwest—down 32% since 2010—compelled patients to navigate not just distance but transportation, lodging, and wage loss, with low-income individuals disproportionately relying on networks like the Reproductive Health Access Project and Aid Access to fund travel to cities like Atlanta, Cleveland, or Washington, D.C. This shift transformed reproductive care from a clinical encounter into a mobility-dependent service regime, where economic inequality filters access through logistical capacity rather than medical eligibility. The underappreciated dynamic is that transit costs began surpassing procedure costs by 2021 in states like Mississippi, marking a transition where access was determined by infrastructure navigation, not proximity to care.
Medical border arbitrage
Abortion tourism is driven not by economic inequality per se, but by the strategic exploitation of jurisdictional disparities in reproductive law, where middle-income individuals leverage mobility to bypass restrictive local regimes. This mechanism operates through privately funded travel to states like Illinois or New Mexico, where clinics can absorb sudden demand surges due to pre-existing infrastructure and provider density, revealing that access is less about absolute poverty and more about navigational capacity within a fragmented legal landscape. The non-obvious insight is that economic resources function not as a direct enabler of care, but as a passport to legal jurisdiction shopping—challenging the assumption that financial disparity is the primary reproductive access barrier.
Regulatory refuge economy
The growth of abortion tourism reflects the emergence of specialized regional economies in states like New Mexico and Washington, where reproductive care has become a codified export industry sustained by out-of-state patient inflows. These states actively insulate providers from extraterritorial legal risks and scale telehealth infrastructure to capture demand from restrictive regions, functioning as institutional havens rather than passive destinations. This reframes the issue not as inequality in access but as the deliberate concentration of medical sovereignty in politically aligned states—undermining the common narrative that economic disparity drives travel, when instead it is the intentional design of safe-state policy ecosystems that enables it.
Infrastructural chokepointing
Abortion tourism does not simply expose economic inequality but reveals how physical clinic concentration in border-adjacent cities like El Paso and Chicago creates artificial scarcity that benefits established providers at the expense of diffuse rural demand. As patients from Texas or Missouri converge on narrow urban entry points, local clinics gain pricing power and scheduling control, effectively rationing care through logistical bottlenecks rather than medical necessity. This mechanism challenges the moral framing of travel as equitable adaptation, exposing instead a quiet capture of reproductive access by urban healthcare nodes that profit from displacement—a dynamic obscured when analysis focuses solely on income gaps.
Travel Burden Threshold
Abortion tourism increases only among individuals with sufficient income to cross state lines. The mechanism hinges on access to transportation, lodging, and time off work—resources unequally distributed along economic lines. This reveals that restrictive state laws do not uniformly affect all populations; instead, they create a de facto filter where reproductive access depends on whether a person can meet the logistical and financial demands of interstate travel. What is underappreciated is that even when legal pathways exist, spatial access remains gated by a minimum economic threshold, not just political geography.
Policy Distance Gradient
The spread of abortion tourism depends on how far patients must travel to reach the nearest legal provider, a distance amplified by economic status. Individuals in rural southern states may face 500-mile trips to clinics in liberal states, a journey feasible only through private vehicles or costly logistics coordinated via apps and nonprofits. The overlooked dynamic is that distance doesn’t reflect political borders alone but the uneven geographic distribution of both reproductive services and economic capital—where proximity becomes a proxy for wealth, making mobility not just a personal choice but a geospatial cost function.