Tougher Drug Sentences or Treatment? Balancing Policy and Evidence
Analysis reveals 7 key thematic connections.
Key Findings
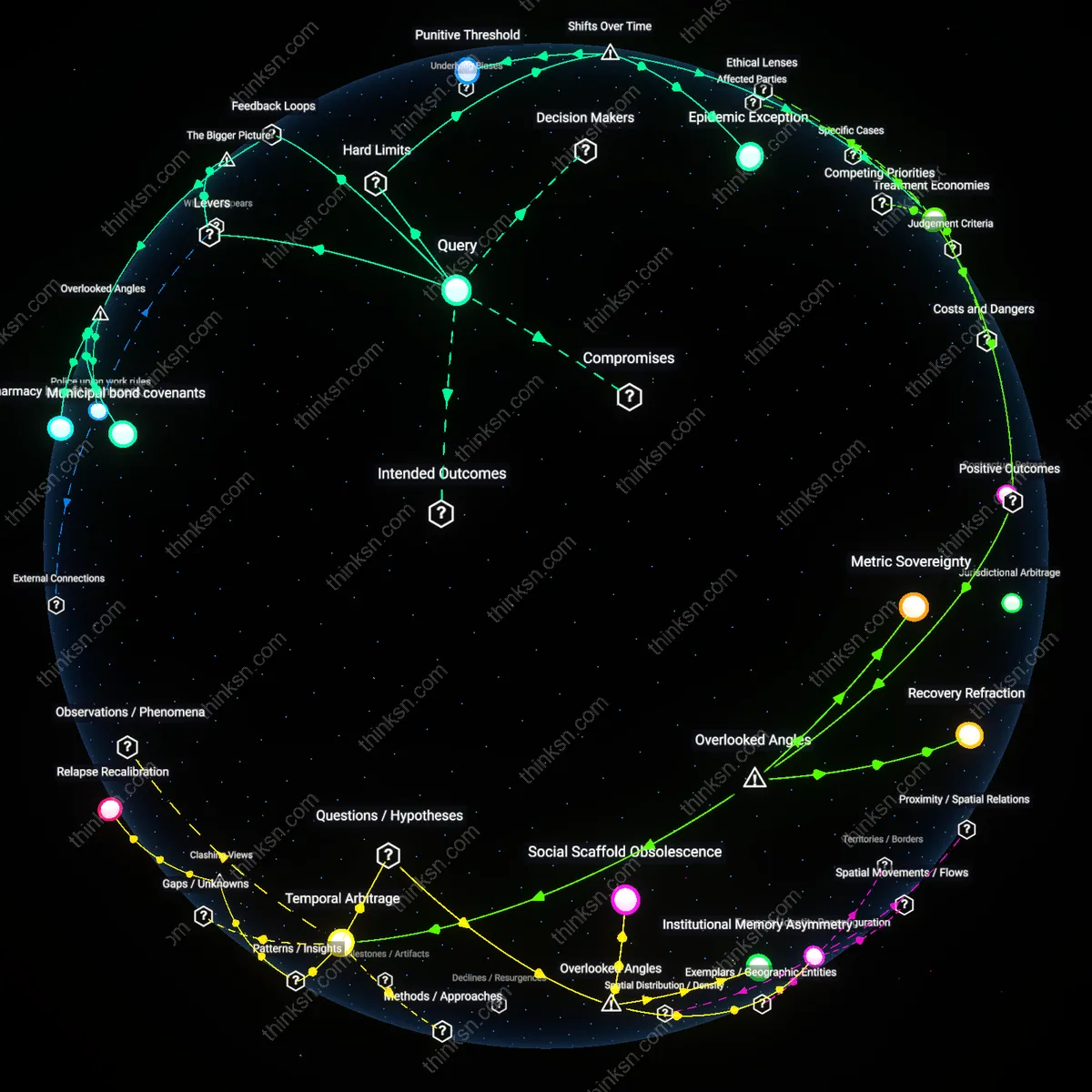
Punitive Threshold
A city can reconcile political demands for harsher drug sentencing with evidence supporting treatment-first strategies by institutionalizing a minimum threshold of recidivism severity required before sentencing overrides treatment referrals, thus preserving punitive credibility while expanding treatment access. This mechanism operates through municipal sentencing guidelines that authorize courts to divert first- and second-time offenders into court-monitored treatment programs unless specific violent or trafficking-related criteria are met—criteria introduced progressively since the 1986 Anti-Drug Abuse Act expanded federal mandatory minimums, revealing how state and local judiciaries absorbed political pressure not by rejecting treatment but by codifying narrow, punitive carve-outs that preserved reform legitimacy. The underappreciated shift is that harsh sentencing demands did not halt treatment expansion but structured its segmentation—defining a residual zone of 'unreformable' offenses to legitimize diversion elsewhere.
Treatment Economies
A city reconciles punitive mandates by contracting private providers to deliver state-subsidized treatment programs that are formally integrated into sentencing structures, transforming social services into a publicly funded but market-mediated mechanism of crime reduction. Since the 1990s, as federal block grants under the Substance Abuse and Mental Health Services Administration incentivized performance-based outcomes, cities like Seattle and San Diego shifted from custodial models to competitive bidding for treatment delivery, aligning political rhetoric of 'accountability' with statistical reductions in rearrest rates—masking a deeper transformation where evidence-based practice became viable only through the financialization of recovery. The critical shift is not from punishment to treatment but to treatment governed by the same logics of efficiency and risk management that once justified incarceration, revealing how neoliberal governance made treatment palatable by pricing it.
Epidemic Exception
A city leverages public health crises—such as the opioid epidemic beginning in the early 2010s—to temporarily suspend certain sentencing enhancements and redirect nonviolent drug offenders into treatment, using emergency authority to override rigid sentencing structures that would otherwise satisfy political demands for severity. This shift became visible during the 2017–2019 state of emergency declarations in Ohio and Massachusetts, where governors issued directives allowing instant access to treatment beds and restricted use of incarceration for possession, exploiting a structural loophole in emergency powers to implement de facto decriminalization without legislative reform. The non-obvious insight is that the return of infectious disease frameworks to drug policy—absent since the 1980s HIV crisis—created a new legitimate exception to punishment, revealing 'crisis' as a functional category that permits evidence-based responses within otherwise punitive systems.
Sentencing Safeguards
Introduce judicial override mechanisms that allow courts to divert drug offenses from mandatory minimums into court-supervised treatment programs when specific clinical criteria are met. This lever operates through existing criminal courts but inserts medical assessment as a binding input into sentencing determinations, creating a structured exception to political pressure for uniform severity. The significance lies in preserving the appearance of punitive compliance while creating a backchannel for evidence-based diversion—judges gain discretion not to circumvent law, but to apply it conditionally, which absorbs public demand for 'action' while enabling long-term crime reduction. The non-obvious force here is that political support for harsh sentencing often collapses at the local level when judges face operational consequences of overcrowded dockets and prisons, creating space for technical workarounds.
Municipal bond covenants
Revise standard municipal bond covenants to include public health metrics that trigger fiscal penalties for increases in incarceration without corresponding rises in treatment access, thereby altering the financial incentives baked into city debt structures. Bond markets and credit rating agencies quietly govern urban policy flexibility by pricing risk around stability and long-term fiscal liability; embedding health-adjusted penalties reframes incarceration not as a short-term political signal but as a balance sheet exposure. This leverages an overlooked contractual mechanism—standardized covenants in public debt instruments—that creates a feedback loop where punitive expansion automatically increases borrowing costs, counteracting political pressure through market-mediated balancing. The non-obviousness lies in recognizing that capital markets, not just legislatures, enforce behavioral constraints on city governance.
Pharmacy benefit managers
Integrate public health departments into contract negotiations between city governments and pharmacy benefit managers (PBMs) for opioid antagonists and addiction medications, shifting pricing power toward treatment scalability. PBMs operate as hidden price-setting intermediaries in drug procurement, and their formulary decisions directly determine the cost trajectory of scaling up medication-assisted treatment; by inserting public health outcomes into PBM performance metrics, cities can reduce the unit cost of treatment as utilization increases—a rare reinforcing loop where expanding care lowers per-capita expense. Most policy debates focus on law enforcement or clinician capacity, missing how pharmaceutical logistics infrastructure shapes the feasibility of treatment-first transitions at scale.
Police union work rules
Negotiate modifications to police union work rules that tie overtime eligibility to participation in court-ordered treatment program monitoring, rather than arrest quotas or patrol hours, realigning daily officer incentives with system stability. These contracts contain embedded behavioral scripts—such as compensating only enforcement activity—that silently reinforce punitive feedback loops by making presence in treatment ecosystems professionally inert or even penalized. By introducing compensable time for non-coercive engagement in recovery spaces, the union contract becomes a vehicle for cultural change without legislative overhaul. The overlooked dynamic is how labor agreements, typically seen as static compensation tools, actually structure the temporal habits and risk assessments of frontline actors who determine policy de facto.