Is Newborn Hearing Screening About Babies or Business?
Analysis reveals 12 key thematic connections.
Key Findings
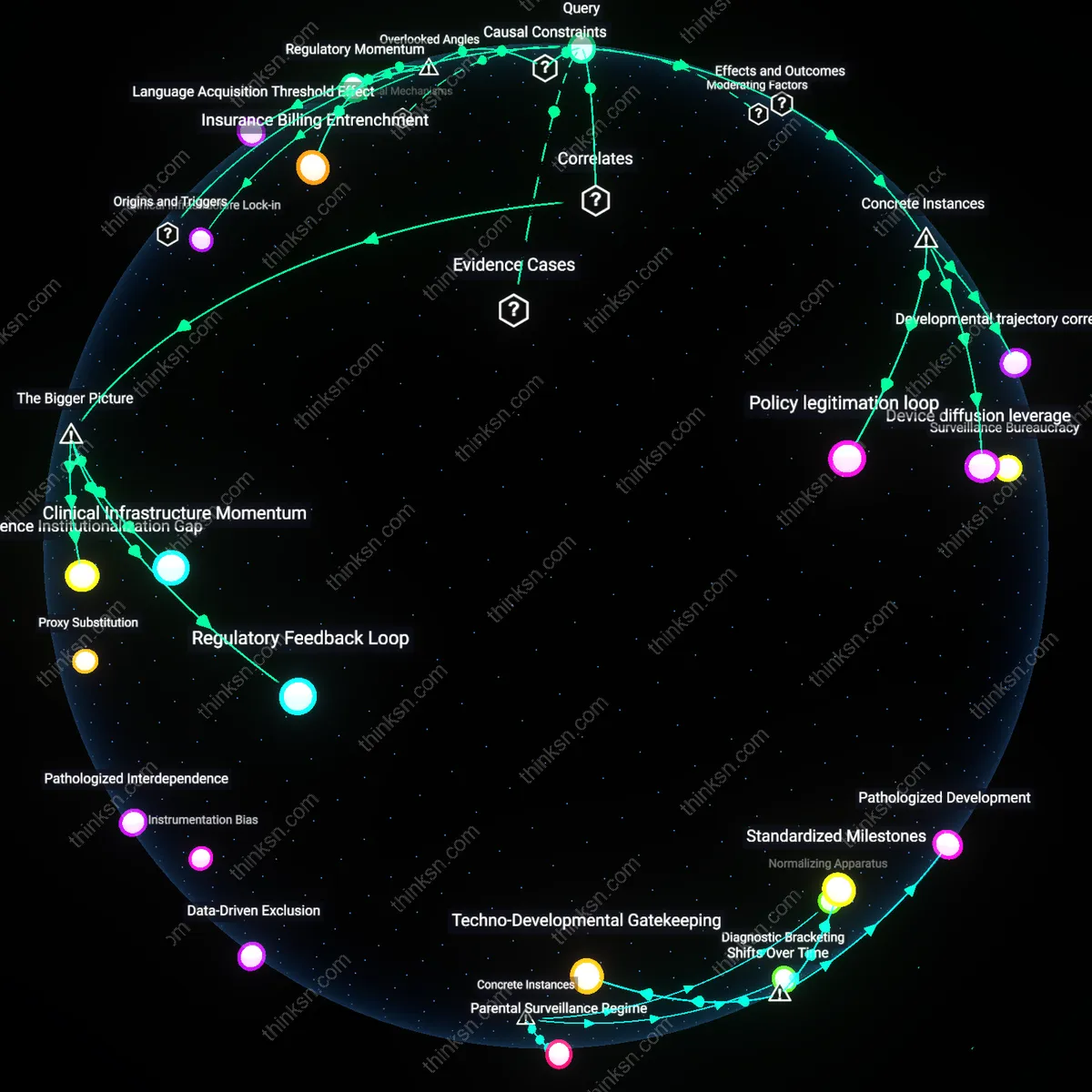
Regulatory Momentum
The motivation behind universal newborn hearing screening emerged primarily from pediatric advocacy networks aligning with state public health mandates, not from equipment sales interests. Pediatric audiologists and developmental pediatricians in the 1990s leveraged longitudinal data from pilot programs—such as the one in Colorado—to demonstrate that early detection before six months reduced language delay, compelling state health departments to institutionalize screening; this created a self-reinforcing policy cascade where clinical guidelines legitimized infrastructure adoption, irrespective of device makers’ lobbying. The non-obvious insight is that the policy predated and dictated market demand rather than the reverse—an inversion of assumed commercial causality.
Evidence Asymmetry
The push for universal screening was sustained by a selective interpretation of developmental outcomes that emphasized language acquisition in hearing children while marginalizing data on psychosocial or educational parity in deaf children integrated into signing communities. By centering 'normalized' speech milestones as the gold standard, policymakers privileged a narrow metric of success that amplified the perceived necessity of early intervention, thereby justifying widespread screening even as outcomes for non-oral deaf education pathways were systematically underrepresented in cost-benefit analyses. This reveals how ostensibly evidence-based policy can function as a conduit for cultural bias, framing hearing correction as inherently progressive.
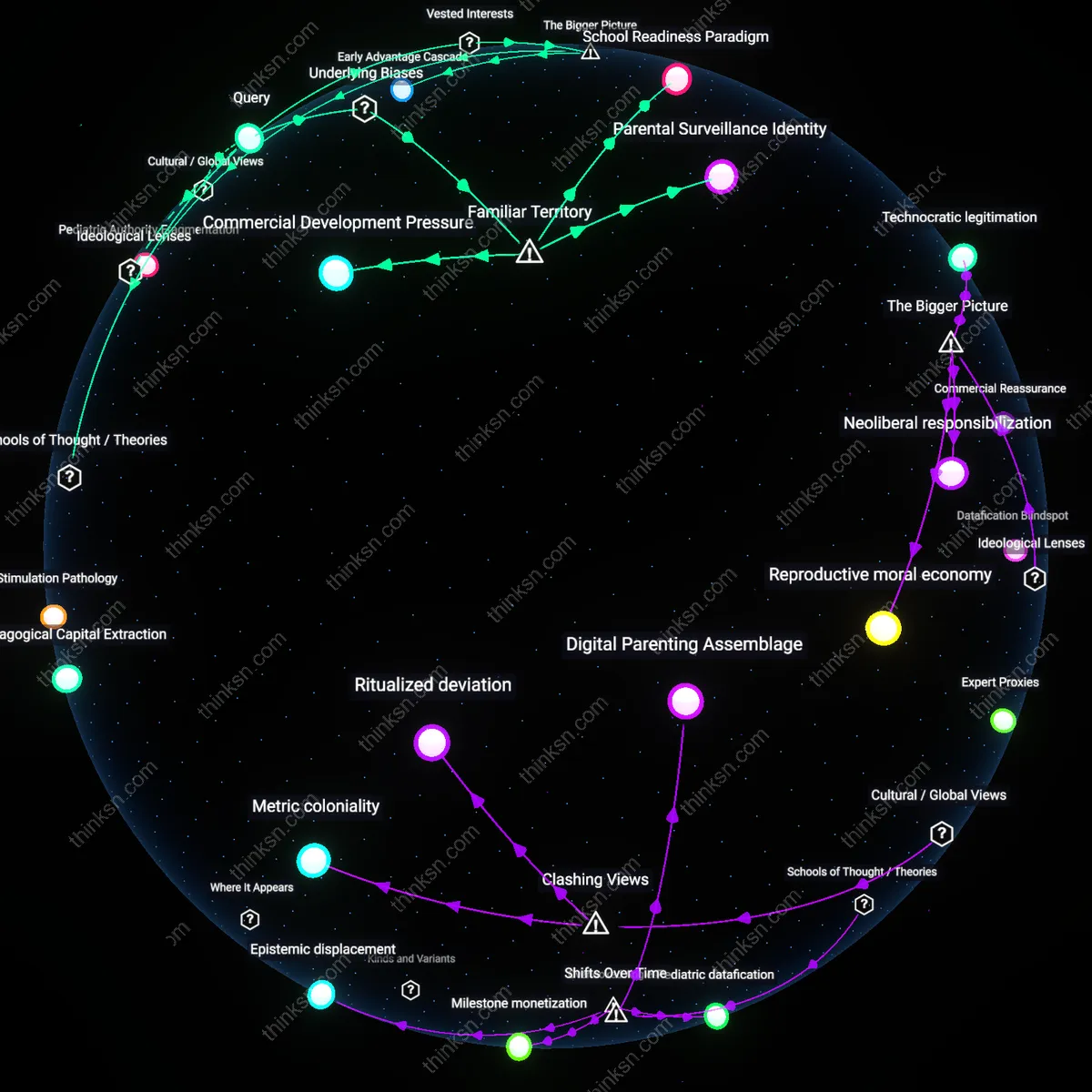
Surveillance Bureaucracy
Universal newborn hearing screening became logistically feasible only through its integration into existing newborn metabolic screening infrastructures, where state-mandated data collection protocols enabled automatic auditory follow-up without requiring new legislative approval or public debate. Public health administrators in states like Rhode Island and Utah embedded hearing tests into established newborn bloodspot screening workflows, leveraging centralized reporting systems and insurance billing codes to make screening appear seamless and non-negotiable. The non-obvious mechanism is thus bureaucratic path dependency—where pre-existing data surveillance systems, not clinical or commercial imperatives, provided the structural enabler for universalization.
Developmental trajectory correction
Universal newborn hearing screening in the United States, mandated through state-level Early Hearing Detection and Intervention (EHDI) programs since the 1990s, directly altered pediatric audiology outcomes by enabling interventions before six months of age, when language acquisition is most malleable; this systemic shift was validated by the 2000 JCIH Position Statement showing significantly improved speech and language outcomes in screened infants, demonstrating that the primary motivation emerged from longitudinal clinical evidence rather than commercial influence. The mechanism—state public health infrastructure adopting screening protocols using transient otoacoustic emissions (TOAE) and auditory brainstem response (ABR) technologies—was driven by NIH and AAP recommendations, not equipment vendor lobbying, revealing that the developmental benefits themselves became the policy engine. This instance is non-obvious because it highlights how clinical research, not market forces, reconfigured neonatal care standards across 50 states despite the existence of commercial stakeholders.
Device diffusion leverage
In rural India, the 2012 launch of the National Program for Prevention and Control of Deafness initially struggled until private-public partnerships enabled the deployment of portable otoacoustic emissions devices by Otodynamics Ltd., whose training workshops and subsidized equipment donations to district hospitals accelerated statewide screening adoption; this expansion was less tied to proven developmental outcomes in that context and more to the manufacturer’s strategic market entry into underpenetrated regions through infrastructure co-optation. The system here operates through humanitarian technology off-ramps, where firms align with national health goals to gain regulatory familiarity and user dependency, embedding their devices in emerging standards. The non-obvious insight is that commercial actors can shape screening implementation indirectly by solving logistical barriers, making their role structurally invisible while being practically indispensable.
Policy legitimation loop
In Sweden, the nationwide newborn hearing screening program initiated in 2002 at Karolinska University Hospital in Solna became the model adopted nationally only after rigorous health technology assessment by the Swedish Council on Health Technology Assessment (SBU), which prioritized evidence of language development gains over cost or equipment availability, thereby insulating policy formation from vendor interests; this process established a feedback loop where clinical outcomes validated screening, which in turn justified procurement, reversing the assumed causality of device availability driving adoption. The mechanism—centralized, independent evaluation before rollout—demonstrates how institutional credibility can preempt commercial influence by making technology adoption contingent on developmental efficacy. The underappreciated aspect is that policy sequencing, not just intent, determines whether commercial interests remain peripheral or central to program initiation.
Regulatory Feedback Loop
Universal newborn hearing screening is sustained primarily by a regulatory feedback loop in which clinical guidelines, once established, create demand for continued equipment use and reimbursement structures that align with device deployment. Public health agencies and professional medical societies adopt screening protocols based on early efficacy studies, which then become embedded in hospital accreditation standards and insurance billing codes—locking in procurement cycles for audiometers and automated auditory brainstem response (AABR) devices. This dynamic persists independently of ongoing developmental outcome improvements because the system rewards procedural compliance over longitudinal patient assessment, making screening continuation structurally self-reinforcing even if marginal benefits diminish. The non-obvious reality is that the durability of screening programs depends less on evolving evidence of child language outcomes and more on institutional inertia shaped by codified medical practice standards.
Clinical Infrastructure Momentum
The expansion of universal newborn hearing screening is driven significantly by clinical infrastructure momentum, whereby hospitals that have invested in specialized audiological equipment and staff training maintain screening programs to justify prior capital expenditures and avoid devaluation of sunk costs. Neonatal intensive care units and birthing hospitals, particularly in high-income countries, have integrated AABR machines into routine postnatal workflows, making discontinuation politically and operationally disruptive despite uncertain long-term cognitive gains. This path dependency emerges not from active profiteering by manufacturers but from institutional resistance to reversing established care pathways once technological and bureaucratic systems are in place. The underappreciated force here is how healthcare delivery systems become committed to technologies through organizational learning and workflow integration, not just through financial incentives or proven developmental outcomes.
Evidence Institutionalization Gap
The motivation behind universal newborn hearing screening persists due to an evidence institutionalization gap, where initial studies showing modest language development advantages in early-identified children became the justification for widespread policy adoption before long-term, population-level outcome data could be assessed. Once adopted by bodies like the U.S. Joint Committee on Infant Hearing, these recommendations triggered funding allocations, equipment procurement, and training pipelines that outpaced later critiques about overdiagnosis, false positives, and limited neurodevelopmental impact in mild cases. This gap allows commercial suppliers to operate within a stable, publicly funded ecosystem not because they drive policy, but because policy has hardened around early, incomplete efficacy signals. The overlooked mechanism is how preliminary clinical correlations become entrenched as standards of care, creating durable markets without requiring ongoing demonstration of benefit.
Clinical Infrastructure Lock-in
The motivation behind universal newborn hearing screening is primarily constrained by the prerequisite of existing audiological infrastructure, which limits scalability and dictates standardization around equipment-compatible protocols. Most neonatal intensive care units in high-income countries depend on transient evoked otoacoustic emissions (TEOAE) and automated auditory brainstem response (AABR) technologies that were adopted before long-term developmental outcomes were fully validated, creating path dependency where hospital systems retrofit clinical guidelines to match vendor-locked workflows rather than developmental metrics. This bottleneck—where technology procurement precedes evidence accumulation—means that once manufacturers align with accreditation bodies like the Joint Commission, screening becomes self-reinforcing through regulatory mimicry, not proven cognitive gains. The non-obvious insight is that the cause (universal screening) depends not on outcome efficacy but on the prior saturation of proprietary diagnostic ecosystems, making equipment availability a de facto gatekeeper to policy implementation.
Language Acquisition Threshold Effect
Universal newborn hearing screening is causally dependent on the unstated prerequisite that early linguistic exposure must occur before age six months to prevent irreversible syntactic deficit formation, a neurodevelopmental window which functions as a biological bottleneck for spoken language mastery. This threshold, demonstrated in cochlear implant cohort studies, means that even if screening delays were only six months, the downstream capacity for phonemic discrimination collapses, rendering later interventions ineffective—a fact that pressures policymakers to adopt screening irrespective of manufacturer influence. What is overlooked is that the motivation arises not from commercial availability nor even general developmental benefit, but from a narrow, irreversible neuroplasticity window that makes timing non-negotiable, thus decoupling the urgency from equipment profit motives and anchoring it instead to a silent, time-limited neural critical period.
Insurance Billing Entrenchment
The expansion of universal newborn hearing screening is bottlenecked by the requirement for procedurally billable codes that integrate seamlessly into hospital revenue cycles, making CPT code 92551 (automated ABR) a de facto policy enabler independent of clinical necessity. Without reimbursement alignment—where screening generates compensable data streams—hospitals in fee-for-service systems cannot sustain screening programs, thereby giving manufacturers implicit power not through direct lobbying but by controlling which devices map to existing billing architectures. The overlooked dynamic is that the causal chain from detection to intervention is gated not by developmental evidence or device accuracy, but by the compatibility of screening outputs with insurance adjudication systems, revealing that the primary reinforcement mechanism is financial workflow integration, not either science or sales.