Vitamin D for MS: Worth the Cost for Modest Benefits?
Analysis reveals 6 key thematic connections.
Key Findings
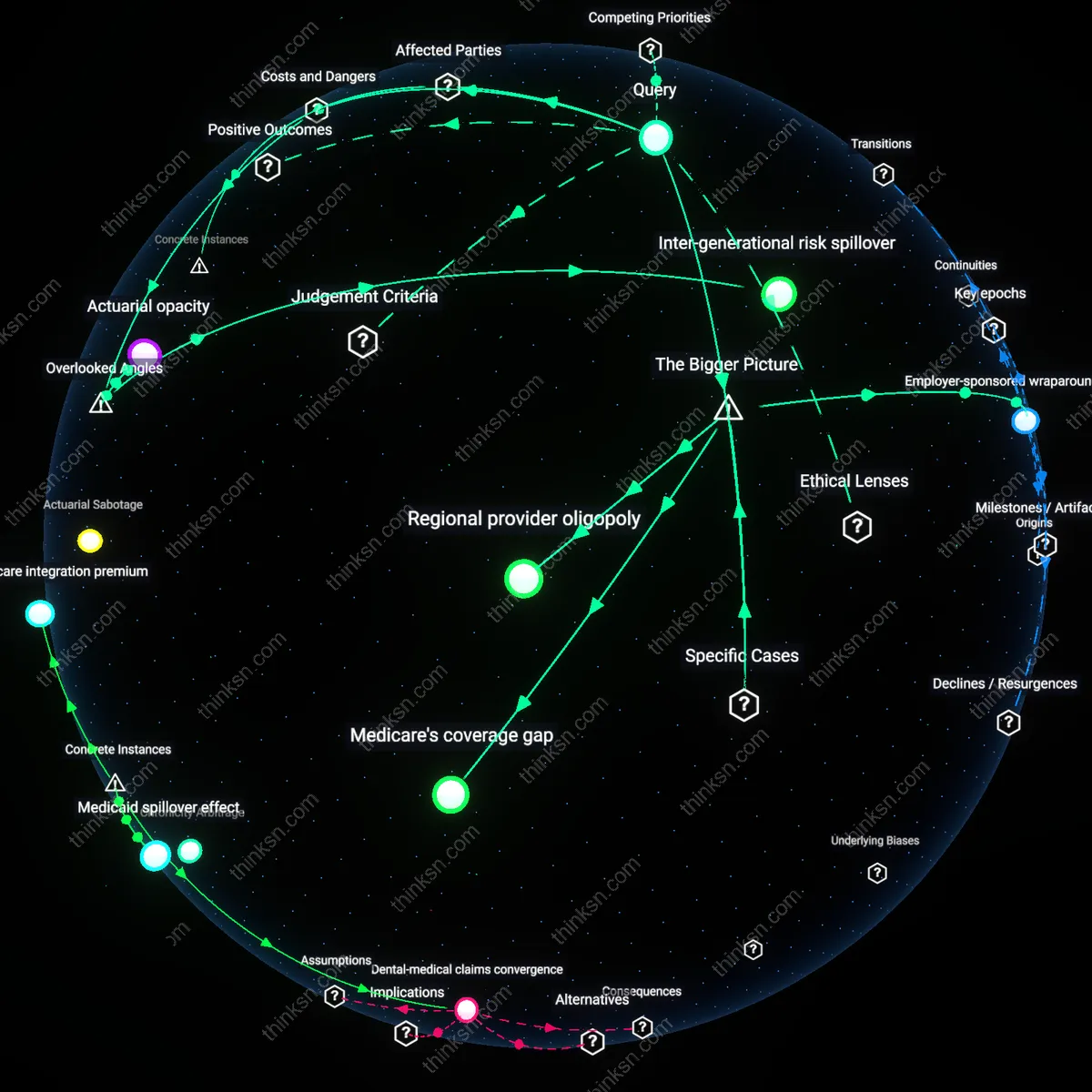
Regulatory Arbitrage
Vitamin D supplementation remains inadequately regulated as a therapeutic intervention for multiple sclerosis because it falls outside the FDA’s drug approval framework, allowing pharmaceutical companies to avoid funding large-scale trials while neurologists and patients bear the burden of uncertain dosing and sourcing. This regulatory gap enables manufacturers of over-the-counter supplements to market vitamin D with minimal oversight, distorting clinical responsibility onto providers who lack pharmacological control over product quality or consistency. The non-obvious consequence is not patient empowerment but institutional deflection—where the absence of formal evidence becomes a self-fulfilling justification for non-intervention by drug developers and payers alike.
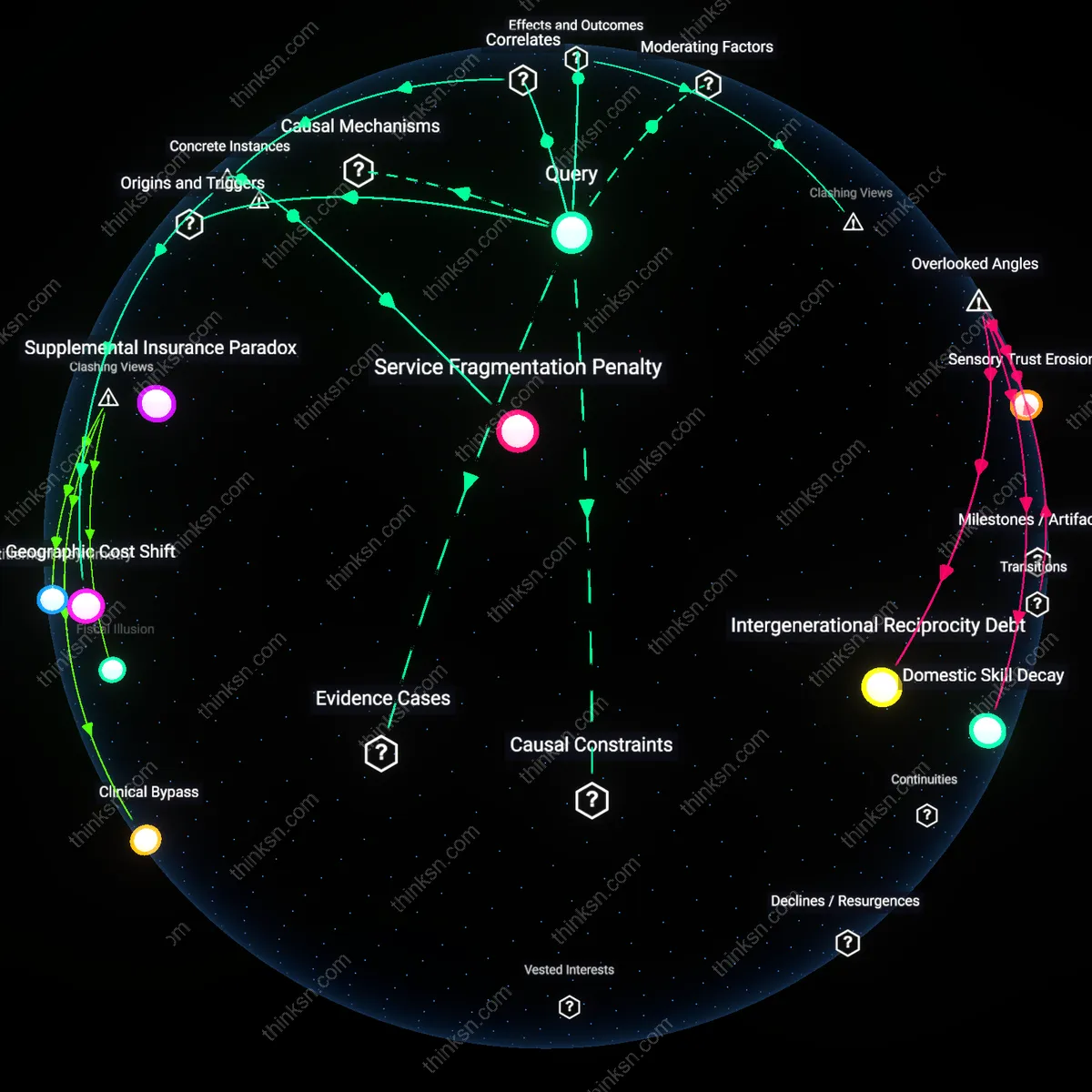
Epistemic Asymmetry
Neurologists propagate inconclusive evidence on vitamin D not due to scientific uncertainty alone, but because they rely on clinical trial standards designed for patented pharmaceuticals, which are structurally unfit for evaluating low-cost, non-patentable nutrients in chronic neuroinflammatory disease. This creates a power imbalance where specialists maintain authority by deferring to high-barrier evidence frameworks, while patients increasingly turn to self-monitoring and online communities to assess efficacy outside clinical paradigms. The dissonance lies in the fact that the rigor intended to protect patients instead marginalizes real-world observational data that could inform personalized management strategies, deepening mistrust in conventional care.
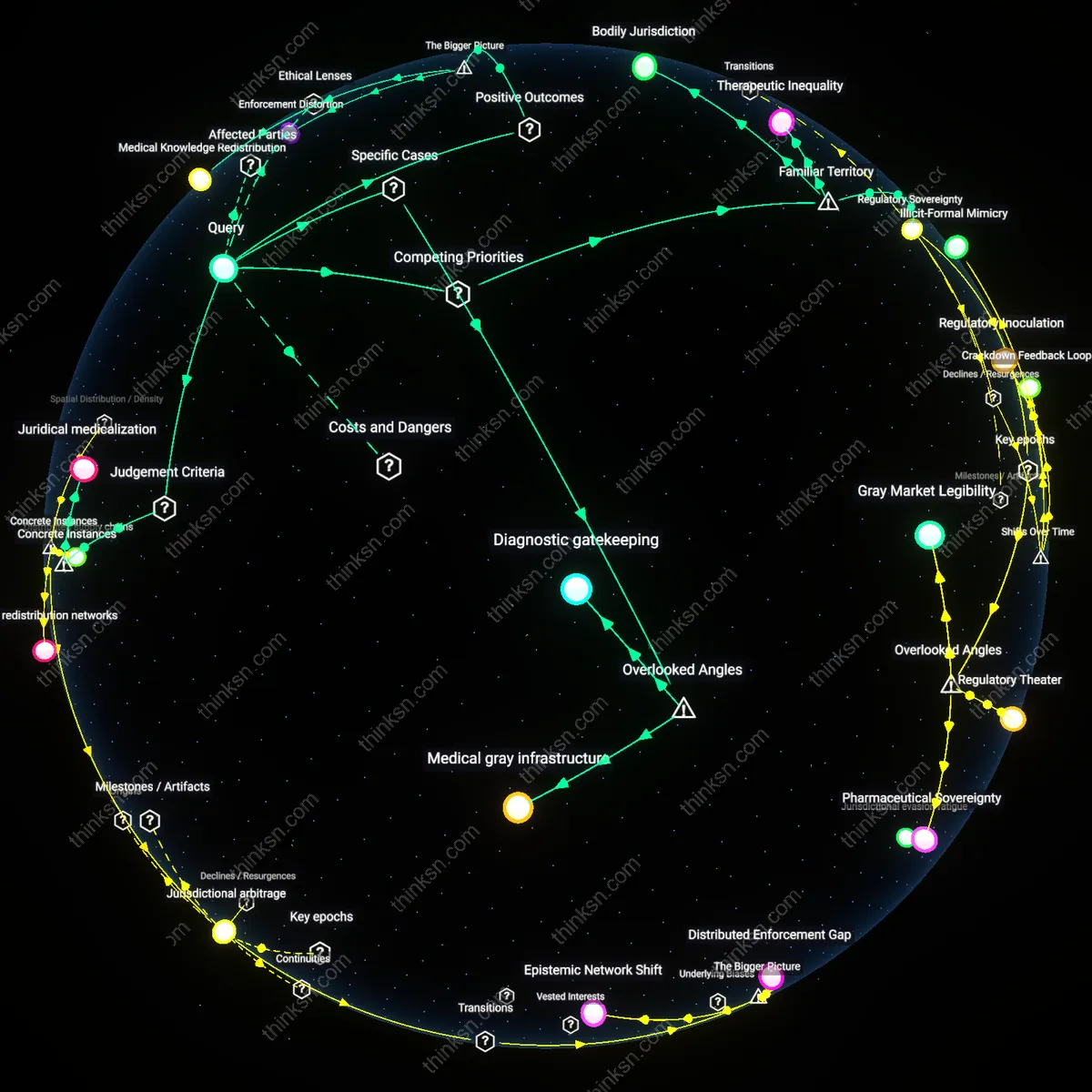
Therapeutic Precarity
Patients with early-stage multiple sclerosis absorb the financial and psychological costs of vitamin D supplementation not because it is proven, but because insurance systems and healthcare providers shift low-risk, low-cost interventions onto individual responsibility, framing them as 'harmless adjuncts' while denying coverage for monitoring or guidance. This cost-shifting turns a biologically plausible intervention into a litmus test for patient diligence, where adherence becomes a proxy for responsibility—regardless of clinical outcome. The overlooked mechanism is not scientific ambiguity but the systematic offloading of preventive care onto individuals under austerity-driven healthcare models, making supplementation a symbol of therapeutic neglect disguised as empowerment.
Therapeutic Ambiguity
Clinical guidelines shifted from precautionary supplementation to evidence-based restraint after 2010, when regulatory agencies like the FDA and EMA began requiring randomized controlled trials for substantiating disease-modifying claims, thereby reclassifying vitamin D from a broadly endorsed adjunct to a contested intervention; this transition exposed the misalignment between patient advocacy groups’ historical reliance on observational data and the pharmaceutical standards now governing neurological therapeutics, revealing how ethical frameworks privileging non-maleficence increasingly override beneficence in chronic disease management when evidence evolves from correlative to interventional.
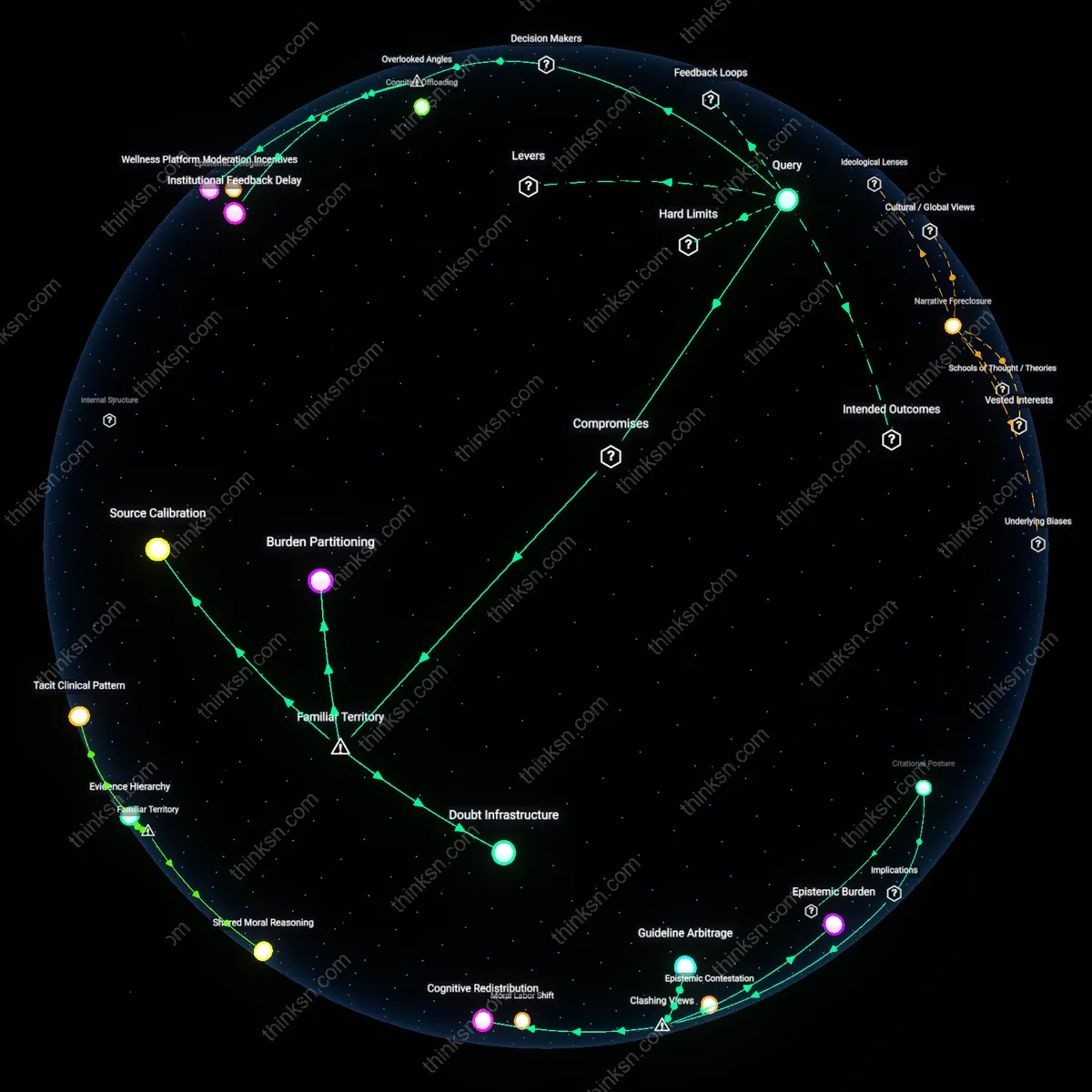
Epistemic Threshold
The standard of proof for recommending vitamin D supplementation shifted decisively during the 2015–2020 revision cycles of the McDonald Criteria for MS diagnosis and monitoring, when methodological rigor in neuroimmunology advanced to prioritize biomarker-confirmed disease activity over clinical symptom reports, rendering earlier population-level studies—once influential in shaping low-cost public health advice—insufficient for individualized treatment protocols; this transformation in evidentiary hierarchy reflects a broader political-ethical turn toward technocratic medicine, where utilitarian cost-benefit analyses are subordinated to epistemic reliability, even at the expense of accessible interventions.
Asymmetric Burden
Following the 2018 European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) guidelines, which conditionally decoupled vitamin D recommendations from disease-modifying therapies, the ethical burden of proof shifted from clinicians to patients, who now must navigate out-of-pocket costs and self-monitoring without institutional support—a transition rooted in neoliberal health policy reforms that reframe preventive self-care as personal responsibility rather than collective welfare, thereby entrenching a moral economy where low-cost supplements are neither prohibited nor endorsed, but deliberately left in evidentiary limbo.