Should I Get the Booster? Herd Immunity vs Personal Risk
Analysis reveals 6 key thematic connections.
Key Findings
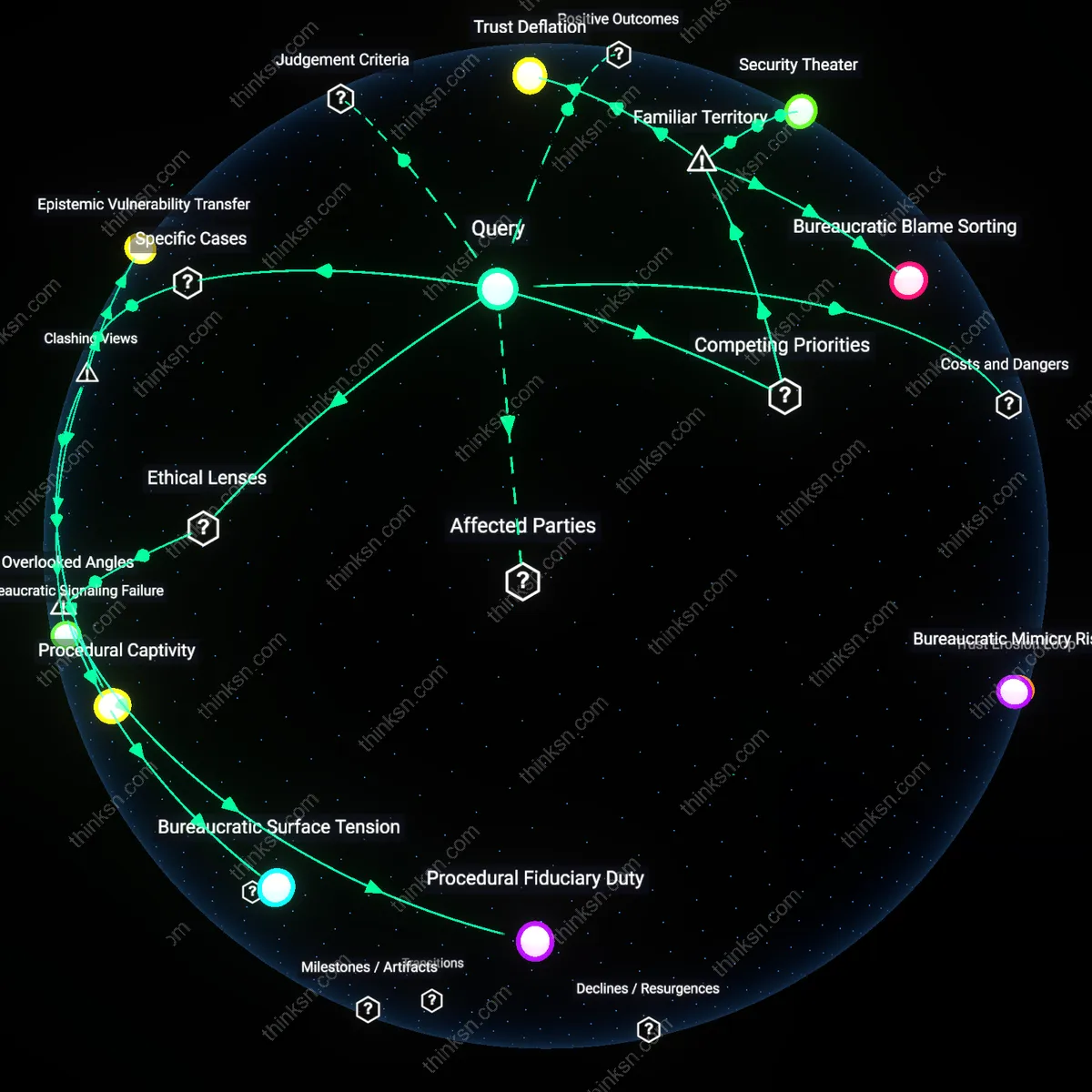
Institutional Trust Deficit
Individuals should defer to public health recommendations on booster uptake because collective compliance sustains healthcare system functionality during viral surges, a mechanism driven by the interdependence between population-level adherence and hospital capacity in urban medical centers. This dynamic hinges on the operational threshold of emergency departments, where even moderate increases in preventable infections can trigger triage overload, a risk exacerbated when vulnerable populations—such as immunocompromised patients and elderly residents in high-density senior facilities—bear disproportionate harm due to delayed care. The underappreciated reality is that personal uncertainty about a new booster’s efficacy is not merely a cognitive bias but a symptom of eroded confidence in regulatory institutions, particularly when fast-tracked approvals by bodies like the FDA or EMA lack transparent, community-accessible data trails, weakening the public’s willingness to absorb individual risk for societal benefit.
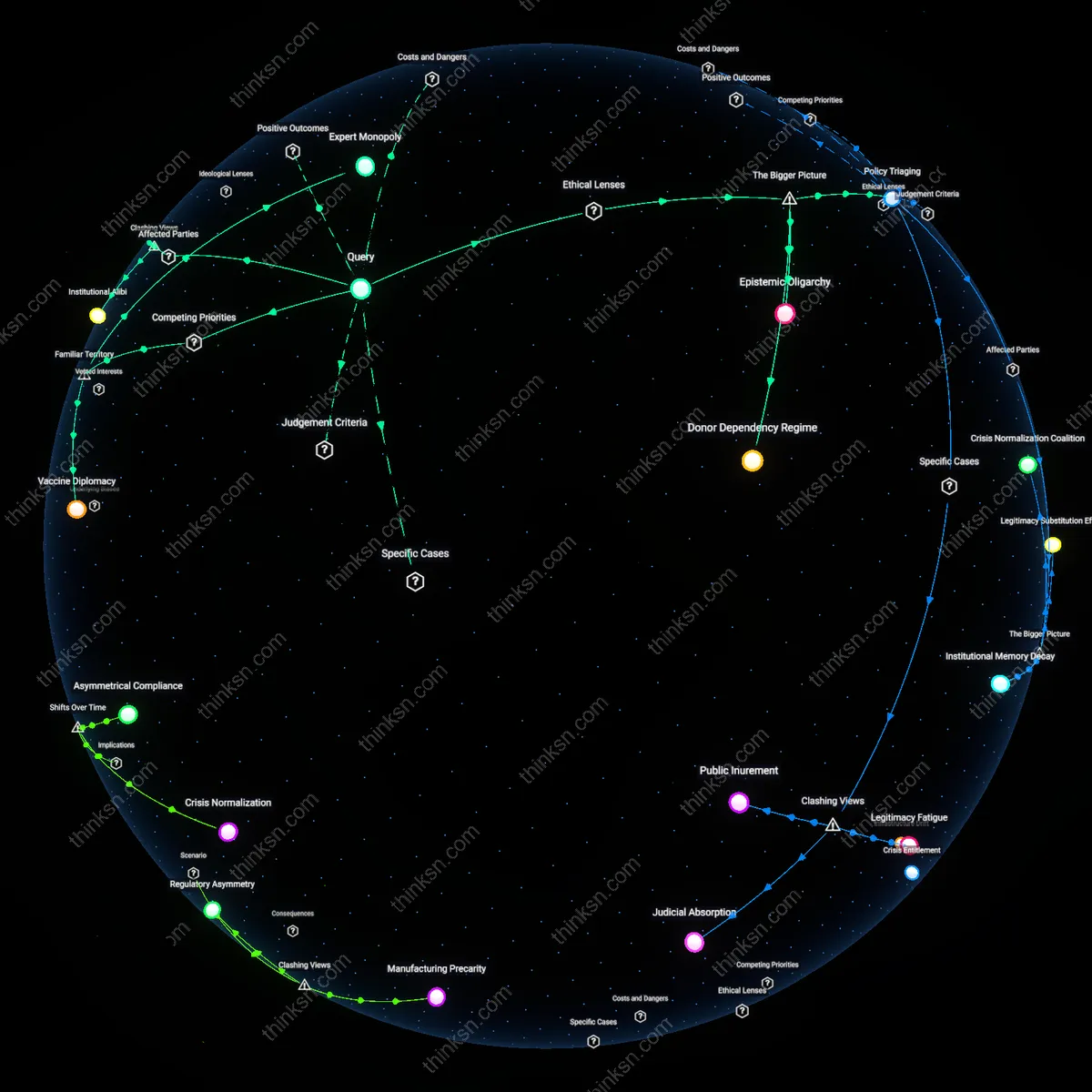
Risk Externalization Dilemma
Individuals must recognize that withholding booster uptake externalizes infection risk onto frontline service workers—especially in transit, retail, and food sectors—who lack remote alternatives and operate in poorly ventilated indoor environments, thereby converting personal medical hesitation into spatialized public health burden along lines of economic precarity. This transfer operates through the labor geography of essential industries, where low-wage, high-contact workers in cities like Chicago or London face elevated exposure rates not due to personal choice but infrastructural constraint, including reliance on shared transportation and congregate housing. The overlooked systemic pressure is that vaccine policy becomes a de facto risk redistribution mechanism when public health goals are pursued without parallel investments in workplace safety mandates or paid sick leave, allowing middle- and upper-income individuals to 'opt out' while shifting morbidity downstream.
Vaccine Fatigue
Individuals should decline the booster due to repeated public health demands eroding trust and compliance. Persistent mandates and shifting guidance from institutions like the CDC and WHO have exhausted public patience, especially among those who already complied with prior doses, creating a backlash against perceived coercion. This fatigue operates through cumulative disillusionment with expert authority, where each new recommendation undermines the perceived legitimacy of the last, making voluntary participation less likely even when medically advisable. The non-obvious consequence is that public health campaigns can become self-sabotaging when they rely on repeated appeals without addressing diminishing psychological returns.
Risk Miscalibration
Individuals should delay the booster because personal uncertainty mirrors systemic inconsistency in communicating evolving risk. The rapid authorization of boosters by the FDA and pharmaceutical companies—based on immune markers rather than real-world disease prevention data—creates confusion about what 'efficacy' actually means for a person in daily life. This mechanism functions through the mismatch between clinical trial outputs (like antibody levels) and public expectations (avoiding illness), leading people to distrust both the product and the process. What’s overlooked is that technical accuracy in regulatory science does not translate into public confidence when the metrics feel detached from lived experience.
Herd Immunity Burden
Individuals should opt out when personal risk is low because the expectation to vaccinate for collective benefit disproportionately affects the cautious and compliant. The logic of herd immunity shifts the cost of public safety onto individuals who are already risk-averse, while those who actively resist face no penalty, creating a moral hazard where responsibility concentrates in the most health-conscious. This dynamic plays out in suburban and urban healthcare networks where vaccinated people bear infection risk from unvaccinated peers despite their own compliance, undermining reciprocity in social contracts. The underappreciated cost is that appeals to solidarity can morph into exploitation of the responsible, weakening long-term civic cooperation.
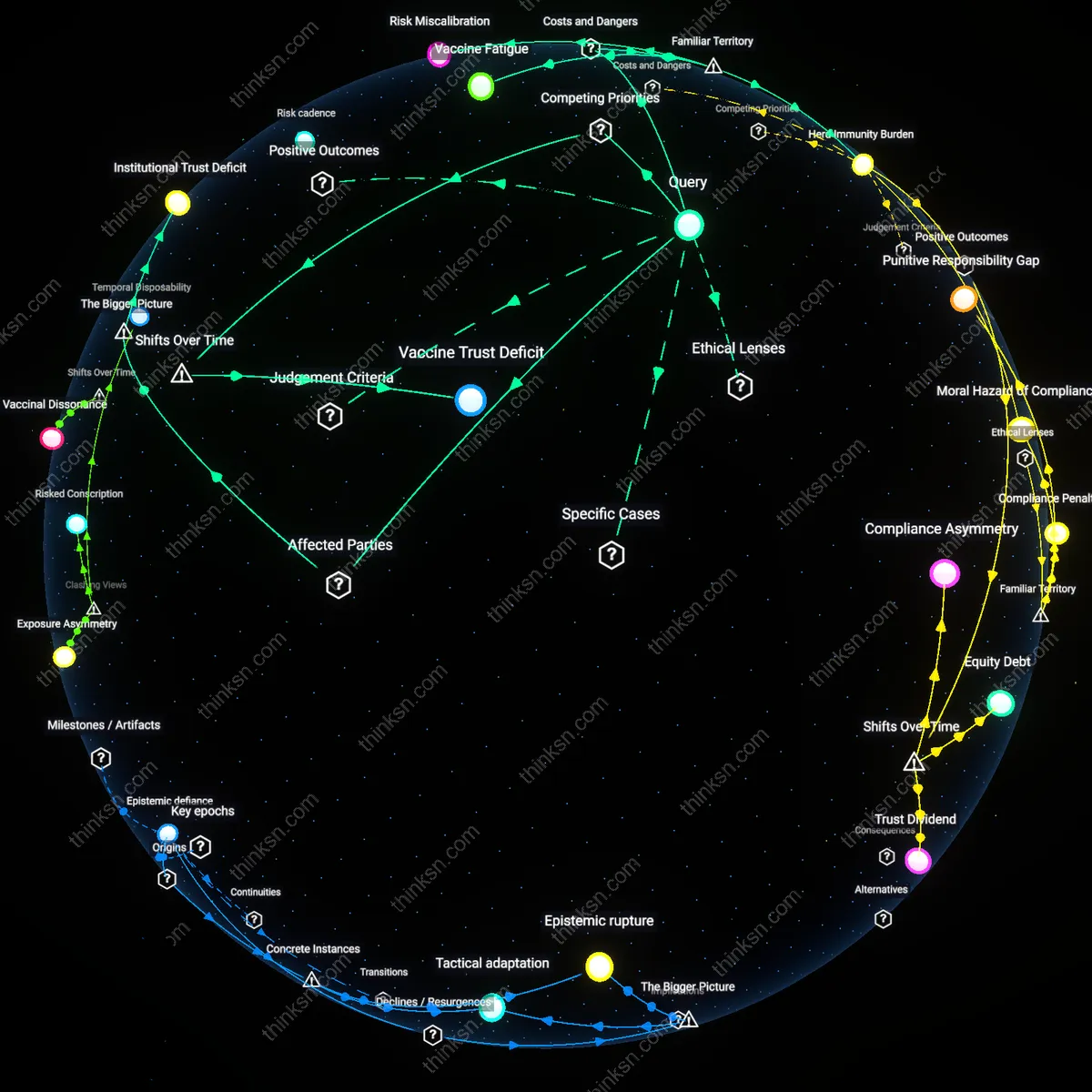
Vaccine Trust Deficit
Individuals should prioritize immediate community protection over personal concerns about booster efficacy because the societal expectation of vaccine compliance has shifted from voluntary public health cooperation to a condition of social reintegration post-2021, particularly as governments and institutions began requiring proof of vaccination for access to public spaces. This transition reframed herd immunity as a gatekeeper to civic participation, making personal uncertainty a secondary consideration in the face of resumed economic and social activity; the mechanism operates through institutional coercion rather than persuasion, revealing an underappreciated erosion in public trust that emerged not during initial rollout but as booster mandates extended the duration of expected compliance.