Why German Hybrid Healthcare Beats US Efficiency?
Analysis reveals 7 key thematic connections.
Key Findings
Path-dependent standardization
Germany’s 1883 Sickness Fund model established a unified claims-processing architecture among competing insurers, eliminating redundant enrollment and billing systems that later emerged in the U.S. as insurers proliferated under deregulation after the 1980s. This early institutional lock-in pressured all payers to conform to a single administrative interface, drastically reducing transaction costs per capita—what became non-obvious in hindsight is that competition did not increase overhead because it occurred within a narrowly constrained, state-enforced procedural monoculture. The 1883 imperative of insuring industrial workers created a technical consensus that persists as a residual administrative order, unlike the U.S., where no such coordination occurred during employer-based system formation in the mid-20th century.
Mutualized risk legacy
The 1930s consolidation of Germany’s fragmented friendly societies into regional Ersatzkassen created a nationwide network of nonprofit insurers that retained local autonomy while sharing actuarial norms and administrative templates, insulating the system from the kind of risk-segmentation escalation seen in the U.S. post-1970s. This suppressed the incentive for high-cost underwriting and enrollment screening because all funds covered identical benefit packages across the same mandated population, embedding a collective cost discipline that later technological and regulatory reforms merely amplified. The overlooked consequence of this Depression-era stabilization is that it pre-empted administrative bloat not by centralizing risk but by standardizing its distribution.
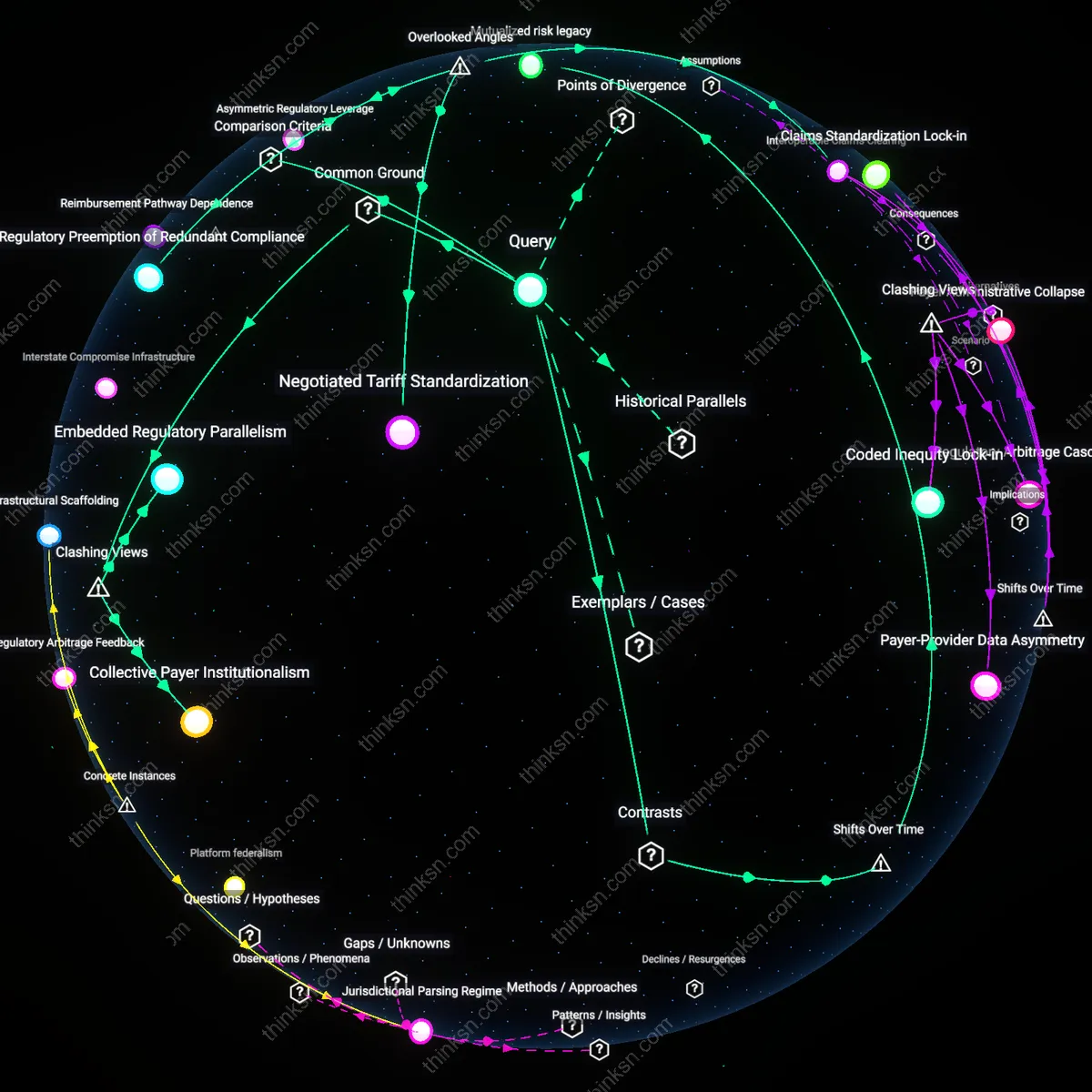
Negotiated Tariff Standardization
Mandatory uniform fee schedules negotiated annually between national associations of physicians and sickness funds eliminate price variability and billing complexity at the point of care. This suppresses administrative overhead by removing the need for providers to manage multiple payer-specific coding, contracting, and collection processes—unlike in the U.S., where fragmented payer negotiations force providers to maintain large billing staffs. The underappreciated factor is not simply cost-sharing or public oversight, but the legally enforced predictability of revenue cycles through synchronized tariff setting, which collapses a core source of transaction cost in healthcare financing.
Regulatory Preemption of Redundant Compliance
Germany’s Federal Joint Committee (G-BA) centrally defines coverage rules, clinical guidelines, and benefit packages that all statutory insurers must follow, preventing individual payers from imposing divergent medical management protocols. This eliminates the need for providers to navigate competing utilization review systems, prior authorization workflows, or quality incentives—each of which generates administrative labor in the U.S. The overlooked dynamic is that administrative bloat in American healthcare stems less from payer multiplicity *per se* than from the regulatory permission for payers to create non-interchangeable compliance demands, a fragmentation actively prohibited in Germany’s hybrid model.
Interoperable Claims Clearing
All German sickness funds and providers route electronic claims through a single, state-mandated interinsurance clearinghouse (KZV) that automatically settles risk-adjusted capitation payments and cross-payer liabilities based on standardized data formats. This infrastructure absorbs reconciliation complexity at the system level, shielding individual providers and insurers from bilateral billing disputes and payment adjudication overhead. Most analyses ignore that the durability of Germany’s multi-payer system relies not on cultural consensus or small-scale organization, but on a hidden backbone of automated financial translation that makes competition administratively lightweight.
Embedded Regulatory Parallelism
Multi-payer systems like Germany’s maintain lower administrative overhead because insurers are structurally prevented from competing on cost-shifting complexity—instead, competition occurs within state-enforced uniformity on billing, coding, and coverage mandates. This constraint forces private payers to act as administrative conduits rather than strategic gatekeepers, reducing redundant verification layers, provider-level billing customization, and patient-facing cost arbitrage—functions that balloon overhead in the U.S. The non-obvious implication is not that public regulation suppresses waste, but that it permits private actors to outsource administrative standardization to the state, effectively embedding regulatory functions inside market mechanisms, which destabilizes the assumed trade-off between public control and private efficiency.
Collective Payer Institutionalism
Administrative efficiency in Germany’s hybrid system stems not from streamlined technology or policy design, but from legally codified power-sharing between sickness funds, providers, and the Federal Joint Committee—ensuring that no payer can unilaterally alter payment rules or documentation demands. This collective decision-making structure removes the incentive for insurers to accumulate administrative capacity for negotiation leverage, a dynamic that drives expansive billing and underwriting departments in U.S. insurers. The friction with dominant interpretations lies in rejecting the notion that scale or digitization reduces overhead; instead, it reveals that administrative bloat in the U.S. is a product of adversarial institutional relationships, not technical inefficiency.